










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.74 n.5 Johannesburg Jun. 2019
https://doi.org/10.17159/2519-0105/2019/v74no5a6
LITERATURE REVIEW
Errors in root canal preparation: a review of the literature and clinical case reports
PJ van der VyverI; M VorsterII; F PalekerIII; FA de WetIV
IBChD, PG Dip Dent (Endo), PG Dip Dent (Aesthet Dent), MSc, PhD (Pret), Department of Odontology, School of Dentistry, University of Pretoria, Pretoria, South Africa and Private Practice, Sandton, South Africa. ORCID Number 000-0003-1951-6042. Responsible for some of the scientific writing and planning of the article. Provided most of the clinical cases reported in the article
IIBChD (Pret), PG Dip Dent (Endo), MSc (Pret), Department of Odontology, School of Dentistry, University of Pretoria, Pretoria, South Africa. ORCID Number 0000-0003-4470-1530. Responsible for some of the scientific writing, contributed to the writing of the abstract, literature review as well as concluding remarks and was also involved in the editing and proofreading of the article as well as editing and verifying of references
IIIBChD (Stell), Dip Odont (Endo), MSc (Pret), Department of Odontology, School of Dentistry, University of Pretoria, Pretoria, South Africa. ORCID Number 0000-0002-5446-309X. Responsible for some of the scientific writing, final layout of the article and collecting cases that were not provided by Prof P vd Vyver
IVBChD, MSc, DSc (Pret), Department of Odontology, School of Dentistry, University of Pretoria, Pretoria, South Africa. ORCID Number 0000-0003-4279-3902. Responsible for some of the scientific writing and for proofreading of the article
SUMMARY
Chemo-mechanical preparation and the removal of infected dentine in order to eliminate microorganisms and avoid apical periodontitis remain the main objectives in endodontic treatment.
Mechanical preparation of the root canal system not only provides the space for obturation but also facilitates disinfection of the root canal system through the use of irrigation solutions.
Iatrogenic preparation errors affect the root canal anatomy and can result in apical canal transportation, uncentered preparations, ledge formation, or perforations. These errors are all associated with inferior outcomes of endodontic treatment.
In this paper, the authors will discuss a review of the literature which considers some of these procedural errors and, using clinical case studies, will illustrate the appropriate clinical management when errors do occur.
INTRODUCTION
The goal of root canal shaping procedures is to treat apical periodontitis through the removal of infected dentine from root canal walls. Endodontic treatment focuses on eliminating microorganisms by chemo-mechanical preparation of the root canal.1,2
Ideal "chemo-mechanical preparation" refers to an adequately shaped canal that is sufficiently accessible by disinfecting solutions. Root canal shaping by means of mechanical preparation not only provides the space for obturation but also facilitates disinfection by disrupting the biofilms that adhere to canal surfaces.3
Correct mechanical instrumentation of the root canal should result in a continuously tapered, funnel-shaped canal that corresponds to the original canal anatomy. This objective is often difficult to achieve when a dentist is faced with the complex internal morphology of curved root canals.4,5 Iatrogenic preparation errors affecting the root canal anatomy remain a problem in this type of anal and can result in apical canal transportation, un-centered preparations, ledge formation, or perforation. Procedural errors that occur during root canal shaping are associated with inferior outcomes.4,5
1. Ledge formation
A ledge is an iatrogenically created irregularity or platform on the inside of the greater curvature of the canal. It may form in the original canal path, create a new false canal, and/or block the apical part of the root canal.6 A ledge that cannot be bypassed impedes instruments and, in some cases, prevents irrigants from entering the apical portion of the canal.
This occurrence results in inadequate instrumentation and incomplete obturation.4,5 Ledges have been associated with persistent peri-apical infection after endodontic treatment.7
Typically, ledge formation occurs when stiff files with sharp inflexible cutting tips are used in a rotational motion in curved root canals. This common procedural error usually occurs on the outer side of the curvature when instruments are used aggressively, with exaggerated cutting during root canal instrumentation.6 Ledges are formed either within the original canal path or through creating a new false canal (Figure 1).

Another study on ledge formation in maxillary and mandibular first and second molars treated endodontically by undergraduate students showed that canal curvature influenced ledge formation more than did the other variables examined.9 As canal curvature increased, so did the number of ledges. Canal curvature in this study was measured by using Schneider's technique.10 Canals with a curvature of less than 10° were rarely ledged, whereas canals with a curvature of more than 20° were ledged over 56% of the time.11 The study also showed that canal location influences the incidence of ledging. The mesio-buccal and the mesiolingual canals were more frequently ledged than were the distal, lingual, or distobuc-cal canals.9 Similar results were also reported in a study which demonstrated that the frequency of occurrence of ledged root canals was significantly greater in molars compared with that seen in anterior teeth.12
According to Lambrianidis (2009) the most common causes of ledge formation are:6
• Incorrect or insufficient access cavity preparation that does not allow adequate and unobstructed access to the apical constriction;
• An incorrect assessment of the root canal direction;
• Incorrect length determination of the root canal;
• Use in a curved canal of stainless steel instruments that are not pre-curved;
• Use of over-curved stiff instruments;
• An attempt to retrieve or by-pass a fractured instrument or a foreign object;
• Removing obturation materials during endodontic retreatment;
• An attempt to negotiate a calcified or a very narrow root canal; and
• During preparation of space for a post after completion of root canal treatment.
Several authors have highlighted additional causes:
• Forcing and driving the instrument into the canal;7
• Using a non-curved stainless steel instrument that is too large for a curved canal;11
• Failing to use the instruments in sequential order;11
• Rotating files excessively at working length;13
• Inadequate irrigation and/or lubrication during instrumentation;14
• Relying too heavily on chelating agents;13 and
• Creating an apical blockage by inadvertently packing debris in the apical portion of the canal during instru-mentation.14
Lateral perforations might occur when the ledge is created during initial instrumentation or as a strip perforation on the concave side of the curvature of the root as the canal is straightened out (a perforation that occurs along the inner wall of a curved root canal).7
Case report 1
The patient, a 49 year old female presented with percussion sensitivity on her mandibular, right second molar. A peri-apical radiograph revealed that all the root canals were prepared short of working length, and showed evidence of peri-apical pathology around the mesial roots (Figure 2).

The tooth was anaesthetised and isolated before the previous obturation material was removed from the root canals using Endosolv E (Septodont) and a size 15 Hedstrom files. A size 10 K-File was introduced into the distal and mesio-buccal root canals, and it was possible to negotiate them to full working length. The same protocol was followed in the mesio-buc-cal root canal but it was impossible to negotiate the canal further. The tip of the instrument was hitting against a solid wall of dentin (Figure 3). A ledge formation in the canal was confirmed at the beginning of the root curvature.

A size 08 C+ - File, 21mm long, with a distinct curve in the apical 2-3mm of the file was selected in the attempt to bypass the ledge. The directional marker on the rubber stop was positioned to indicate the direction of the curve placed on the tip of the file (Figure 4).

The canal was filled with 6% sodium hypochlorite (Chlor-Xtra, Vista Dental). The file was introduced into the canal, ensuring that the curved tip was directed towards the wall opposite the ledge. A slight rotation motion combined with a light "picking motion" was used to try to discover the original canal entrance. After several attempts, re-orientating the file in different positions, the pre-curved file tip advanced for about 0.5 mm (Figure 5).

The file was slightly retracted, and advanced again. This procedure was repeated and the file progressively advanced further down the canal for another 2.5mm. The 08 C+-File, with the tip placed apically to the ledge, was used with a filing motion combined with push-pull motions, pushing the file against the canal wall in the endeavour to reduce the internal canal irregularity.
The C+-File was removed and the canal was irrigated before a pre-curved size 08 K-File was negotiated to full working length and patency. The working length was confirmed radiographically after using an electronic apex locator (ProPex Pixi, Dentsply Sirona).
Figure 6 shows the final result after glide path preparation with a ProGlider (Dentsply Sirona), canal preparation with a Primary WaveOne Gold (Dentsply Sirona) instrument and canal obturation with gutta-percha and Pulp Canal Sealer (SybronEndo, Orange, California) using warm vertical condensation technique.

2. Canal transportation
Canal transportation is a sustained deviation from the original axis of the canal during root canal instrumentation (Figures 7a and 7b).
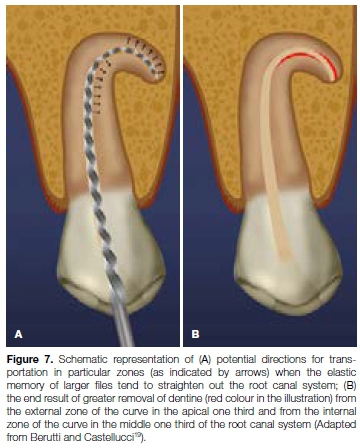
Apical canal transportation is described as the removal of canal wall structure on the outside curve in the apical half of the canal due to the tendency of files to recover to their original linear shape during canal preparation.15
As a result, the main axis of the root canal is transported away from its original axis. Other terms for canal transportation include "canal straightening" and "zipping".4
Stiff endodontic instruments, particularly large-sized stainless steel files, tend to exert elevated lateral forces in curved canals and can result in straightening, especially in the middle and apical thirds.16
This straightening or transportation can create problems with canal cleaning, obturation and, ultimately, healing.4,5 Apical canal transportation can cause enlargement of the apical foramen (Figures 8a and 8b), which compromises the apical seal.17 Lack of an apical stop might result in extrusion of irrigants and/or obturation materials and cause irritation to the peri-radicular tissues.4,18

Figures 9 and 10 illustrate micro-computed tomographic images of two curved mesio-buccal root canal systems of extracted, maxillary first molar teeth at a level 1mm from the apical foramen. The example in Figure 9 shows minimal canal transportation after root canal preparation compared with that in Figure 10 which clearly shows an excessive amount of canal transportation.


Case report 2
The patient, a 54 year old female, presented with irreversible pulpitis on her maxillary left first premolar, caused by extensive decay under a previously placed porcelain veneered crown (Figure 11). After removal of the defective crown and decay a core build-up was done prior to root canal treatment. A size 10 K-File was negotiated to full working length and confirmed radiographically (Figure 12). Note the sharp apical curvature in the last 3mm of the root canal system.


The root canal system was prepared with the Pro-Taper Universal (Dentsply Sirona) system. Incorrect use of the X3 file (30/09) resulted in apical transportation. This was visible on the peri-apical radiograph taken to confirm the cone-fit of the gutta-percha point (Figure 13). After root canal obturation it became more evident that an excessive amount of the root canal wall structure on the outside curve in the apical part of the canal was removed by the rotary file. This resulted in the loss of the original apical curvature, lack of an apical stop and subsequent extrusion of the obturation material (Figure 14).


3. Perforation
A direct perforation is a channel or communication between the root canal space and surrounding cementum (Figures 15a and 15b). Such a perforation can result in the destruction of cementum and the irritation and/or infection of the periodontal ligament in the surrounding area. As with ledging, perforation of curved canals is associated with stiff instruments with sharp cutting tips used in a rotational motion.

Depending on the location, a perforation cannot easily be sealed and/or bypassed, which results in an inadequately prepared and sealed root canal.4,5
A perforation that occurs along the inner wall of a curved root canal is referred to as a "strip perforation" (Figure 15c).
This results from over-preparation and straightening along the concavity and is of particular concern in the mesiobuccal roots of maxillary molars and mesial roots of mandibular first molars.20,21 The root walls facing the furcal aspect of roots are often extremely thin and are therefore termed "the danger zone".22
Case report 3
The patient, a 37 year old female presented with irreversible pulpitis on her maxillary left first second premolar. The tooth had been previously restored with a large composite resin restoration and two retention pins. A preoperative peri-apical radiograph (Figure 16) and a length determination radiograph (Figure 17) revealed and confirmed a challenging "S" shaped or bayonet-shaped root canal configuration.


Due to the lack of proper glide path preparation and management in this case, the operator was faced with a rotary file fracture in the apical part of the root canal and a strip perforation at the point of maximum curvature on the distal aspect of the root. It was impossible to even attempt the retrieval of the fractured instrument and it was left in situ.
After canal irrigation, the perforation was repaired with ProRoot MTA (Dentsply Sirona) before conventional canal obturation (Figure 18).

The access cavity was restored with composite resin and placement of a fibre post. Figure 19 shows a four-year follow up radiograph with some evidence of resorption of the extruded ProRoot MTA material.

4. Uncentered preparations
The ability of an instrument to stay centered in the canal can be measured by the mean centering ratio.23 The importance of maintaining preparations that are centered (Figure 20a) and correspond to the original canal anatomy has been pointed out by Berutti et al.24 A study by Pasqualini et al. examined rotary glide path files and concluded that files with a high root canal centering ability resulted in fewer modifications of the canal curvature and therefore fewer canal aberrations.25 Several studies have shown that more flexible instruments produce more centered preparations.26,27 Flexibility can be defined as the elastic bending of an endodontic instrument when subject to a load applied at its extremity in the direction that is perpendicular to its long axis.28

Flexibility may influence an instrument's ability to properly shape curved root canals. Inflexible files, on the other hand, may cause a deviation from the original canal axis, which can result in canal straightening, transportation, thinning of the canal wall and perforation (Figure 20A and 20B).
5. Instrument separation
A common problem with the use of rotary files is the potential risk of separation or breakage within the canals.29 In most clinical situations, the breakage of the instrument occurs in the apical third of the canal and the remaining portion is often difficult or impossible to remove.30,31 Attempts at removal may even result in other procedural errors like perforation. The fragment that is left behind blocks the root canal system and results in inadequate cleaning, shaping and sealing (Figure 21A and 21B).32

Fracture of rotary instruments can occur because of tor-sional overload33, or fatigue through flexure.34 The torsio-nal fracture occurs when the tip or any other part of the instrument binds to the canal walls while the hand piece keeps turning. When this binding occurs and the elastic limit of the metal is exceeded, fracture of the instrument is inevitable.
This type of fracture has been associated with the application of excessive apical force during instrumentation. Fracture resulting from flexural fatigue occurs when an instrument that has already been weakened by metal fatigue is placed under stress.
The instrument does not bind to the canal wall but rotates freely until the fracture occurs at the point of maximum flexure.33 This type of failure is believed to be an important factor in the fracture of nickel-titanium (NiTi) rotary instruments in clinical usage, and might result from their use in curved canals.30 Various factors have been associated with the fracture of rotary instruments: rotational speed and angle and radius of curvature,30 instrument design and instrumentation technique35, torque36, and operator experience.37
Case report 4
The patient, a 21 year old male presented with a fractured rotary file in his maxillary left upper central incisor. The fragment (14mm long) was located approximately 4mm apically from the cemento-enamel junction at the coronal aspect extending apically to about 5 mm from the apical foramen (Figure 22). Under 15x microscope magnification, the fractured instrument was clearly visible in the canal (Figure 23).


It was decided to use the Terauchi File Retrieval Kit (TFRFK) (Dental Cadre) to assist in removal of the fractured instrument. The 12 o'clock Micro-spoon ultrasonic tip (Figure 24) was used to penetrate through between the file and the canal wall in circular motion until it was noticed that the fractured file was loose in the canal. Considering the length of the fragment it was decided to attempt retrieval using the Yoshi Loop (Dental Cadre) (Figure 25a and 25b), a stainless steel micro-lasso that extends from the end of a stainless steel cannula attached to a handle with a retraction button for tightening the loop around the file segment.



Under magnification, the preformed loop was carefully placed around the exposed coronal aspect of the file. The loop was tightened around the fractured file by moving the retraction button on the loop system. The loop device was then used to slowly pull the loosened fragment from the root canal system (Figure 26). Figure 27 shows a magnified view of the retrieved instrument attached to the micro-lasso from the Yoshi Loop. Note that the tip of instrument is missing, indicating that the file tip must have been fractured in a previous clinical application prior to the case presented in this case report.


Having removed the fractured instrument, a size 30 K-File was fitted loose in the root canal up to working length as confirmed radiographically and with an electronic apex locator (ProPex, Dentsply, Sirona). According to the file selection criteria outlined by Van der Vyver et al. (2019)38 for WaveOne Gold files, a size large WaveOne Gold File (45/05) was selected for canal preparation.
After canal preparation and irrigation with heated 3.5% sodium hypochlorite and 17% EDTA solutions, a size Large WaveOne Gold Gutta Percha Point (Dentsply Sirona) was fitted and the position verified radiographically.
The canal was obturated with the selected gutta percha point and Pulp Canal Sealer (SybronEndo), using the continuous wave condensation technique with the Calamus Dual Obturation Unit (Dentsply Sirona).
6. Apical bacterial extrusion
All root canal preparation techniques cause apical debris extrusion to some degree, in spite of stringent control of working length of instruments during debridement. Some amount of debris in the form of dentinal chips, pulp fragments, necrotic debris, microorganisms, and intra-canal irrigants is unavoidably pushed out from the root canal into the peri-apical tissues.
The volume of materials that are extruded depends on canal/apical foramen size, instrumentation technique, instrument type, instrument size, preparation end-point and irrigation solution (Figure 26).39



The extruded material is referred to as the ''worm of necrotic debris'' and has been linked to peri-apical inflammation and postoperative flare-ups that will likely interfere with healing.40 The incidence of flare-ups during root canal treatment is reported to range between 1.4% and 16%.41
In asymptomatic chronic peri-radicular lesions a balance exists between host defences and microbial aggression from the root canal microbiota associated with infected canals in peri-radicular tissues.42 If bacteria are extruded apically during root canal treatment procedures, there will be a transient disruption in this balance and the host will mobilise an acute inflammatory response to re-establish the equilibrium. The intensity of this acute inflammatory response depends on the number and/or virulence of the bacteria.41
According to Reddy and Hicks (1994) the variation in levels of apical extrusion is primarily due to different root canal preparation techniques and instrument designs.43 Many studies have shown that techniques involving a push-pull filing motion result in a greater mass of apical debris compared with techniques that involve some sort of rotational action.39,44
Luisi et al. have demonstrated that the direction of instrumentation, either in cervico-apical or apico-cervical, is also an important factor influencing apical extrusion.44 Crown-down techniques, irrespective of whether hand-driven- or engine-driven instruments are used, usually extrude less debris.45,46
CONCLUSION
Procedural errors during endodontic treatment are associated with a reduction in treatment success and possible non-resolution of apical periodontitis. Correct clinical management of these iatrogenic procedural errors could aid in proper preparation, allowing for disinfection of root canal systems and an increase in successful outcomes of endodontic treatment.
References
1. Sjogren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root Alling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J. 1997; 30:297-306. [ Links ]
2. Shuping G, 0rstavik D, Sigurdsson A, Trope M. Reduction of intracanal bacteria using nickel- titanium rotary instrumentation and various medications. J Endod. 2000; 26:751 -5. [ Links ]
3. Haapasalo M, Endal U, Zandi H, Coil J. Eradication of endo-dontic infection by instrumentation and irrigation solutions. Endod Top. 2005; 10:77-102. [ Links ]
4. Hülsmann M, Peters O, Dummer P. Mechanical preparation of root canals: shaping goals, techniques and means. Endod Top [Internet]. 2005; 10(1):30-76. Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1601-1546.2005.00152.x/abstrac. [ Links ]
5. Cheung G, Liu C. A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. J Endod. 2009; 35(7):938-43. [ Links ]
6. Lambrianidis T. Ledging and blockage of root canals during canal preparation: causes, recognition, prevention, management, and outcomes. Endod Top. 2009; 15:56-74. [ Links ]
7. Jafarzadeh H, Abbott P. Ledge formation: review of a great challenge in endodontics. J Endod. 2007; 33:1155-62. [ Links ]
8. Oikonomou I, Spanaki-Voreadi A, Georgopoulou M. Procedural errors during root canal treatment performed by undergraduate students in Athens: a prospective study. Int Endod J. 2007; 40:982. [ Links ]
9. Greene K, Krell K. Clinical factors associated with ledged canals in maxillary and mandibular molars. Oral Surg Oral Med Oral Pathol. 1990; 70:490-7. [ Links ]
10. Schneider S. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontology. 1971; 32:271-5. [ Links ]
11. Kapalas A, Lambrianidis T. Factors associated with root canal ledging during instrumentation. Endod Dent Traumatol. 2000; 16:220-31. [ Links ]
12. Eleftheriadis G, Lambrianidis T. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. Int Endod J. 2005; 38:725-34. [ Links ]
13. Weine F. Endodontic therapy. 5th ed. St Louis: Mosby; 1996. 324-30, 545-7. p. [ Links ]
14. Walton R, Torabinejad M. Principles and practice of endodontics. 3rd ed. Philadelphia: WB Saunders; 2002. 184, 222-3, 319-20. p. [ Links ]
15. American Association of Endodontists. Glossary of Endodontic Terms [Internet]. 2012. Available from: http://www.aae.org/publications-and-research/glossaries-and-guides/glossaries-guides.aspx [ Links ]
16. Lam T, Lewis D, Atkins D, Macfarlane R, Clarkson R, Whitehead M, et al. Changes in root canal morphology in simulated curved canals over-instrumented with a variety of stainless steel and nickel titanium files. Aust Dent J. 1999; 44:12-9. [ Links ]
17. Wu M, Fan B, Wesselink P. Leakage along apical root fillings in curved root canals. Part I: effects of apical transportation on seal of root fillings. J Endod. 2000; 26:210-6. [ Links ]
18. Schäfer E, Dammaschke T. Development and sequelae of canal transportation. Endod Top. 2009; (4):75-90. [ Links ]
19. Berutti E, Castellucci A. Cleaning and shaping of the root canal system. Endodontics. 2009; 2 (IL Tridente, Florence, Italy). [ Links ]
20. Kessler J, Peters D, Lorton L. Comparison of the relative risk of molar root perforations using various endodontic instrumentation techniques. J Endod. 1983; 9:439-47. [ Links ]
21. Allam C. Treatment of stripping perforations. J Endod. 1996; 22:699-702. [ Links ]
22. Abou-Rass M, Frank A, Glick D. The anticurvature filing method to prepare the curved root canal. J Am Dent Assoc. 1980; 101:792-4. [ Links ]
23. Yamamura B, Cox T, Heddaya B, Flake N, Johnson J, Paranjpe A. Comparing canal transportation and centering ability of endosequence and vortex rotary files by using micro-computed tomography. J Endod [Internet]. 2012; 38(8):1121 -5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22794219. [ Links ]
24. Berutti E, Cantatore G, Castellucci A, Chiandussi G, Pera F, Migliaretti G, et al. Use of nickel-titanium rotary PathFile to create the glide path: comparison with manual preflaring in simulated root canals. J Endod. 2009 Mar; 35(3):408-12. [ Links ]
25. Pasqualini D, Bianchi C, Paolino D, Mancini L, Cemenasco A, Cantatore G, et al. Computed micro-tomographic evaluation of glide path with nickel-titanium rotary PathFile in maxillary first molars curved canals. J Endod. 2012; 38(3): 389-93. [ Links ]
26. Short J, Morgan L, Baumgartner J. A comparison of canal centering ability of four instrumentation techniques. J Endod. 1997; 23:503-7. [ Links ]
27. Gergi R, Rjeily J, Sader J, Naaman A. Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. J Endod. 2010; 36(5):904-7. [ Links ]
28. Lopes H, Elias C, Siqueira JJ, Soares R, Souza L, Oliveira J, et al. Mechanical behavior of pathfinding endodontic instruments. J Endod. 2012; 38:1417-21. [ Links ]
29. Pereira E, Peixoto I, Viana A, Oliveira I, Gonzalez B, Buono V, et al. Physical and mechanical properties of a thermome-chanically treated NiTi wire used in the manufacture of rotary endodontic instruments. Int Endod J. 2011; 45(5):469-74. [ Links ]
30. Pruett J, Clement D, Carnes DJ. Cyclic fatigue testing of nickeltitanium endodontic instruments. J Endod. 1997; 23:77-85. [ Links ]
31. Schrader C, Ackermann M, Barbakow F. Step-by-step description of a rotary root canal preparation technique. Int Endod J. 1999; 32:312-20. [ Links ]
32. Haikel Y, Serfaty R, Bateman G, Senger B, Allemann C. Dynamic and cyclic fatigue of engine-driven rotary nickeltitanium endodontic instruments. J Endod. 1999; 25:434-40. [ Links ]
33. Sattapan B, Palamara J, Messer H. Torque during canal instrumentation using rotary nickel-titanium files. J Endod. 2000; 26:156-60. [ Links ]
34. Al-Hadlaq S, AlJarbou F, AlThumairy R. Evaluation of cyclic flexural fatigue of m-wire nickel-titanium totary instruments. J Endod [Internet]. 2010; 36(2):305-7. Available from: http://dx.doi.org/10.1016/j.joen.2009.10.032. [ Links ]
35. Bryant S, Thompson S, Al-Omari M, Dummer P. Shaping ability of Profile rotary nickel-titanium instruments with ISO sized tips in simulated root canals: Part 1. Int Endod J. 1998; 31:275-81. [ Links ]
36. Gambarini G. Rationale for the use of low-torque endodontic motors in root canal instrumentation. Endod Dent Traumatol. 2000; 16:95-100. [ Links ]
37. Yared G, Bou Dagher F, Machtou P. Influence of rotational speed, torque and operator's proficiency on ProFile failure. Int Endod J. 2001; 34:47-53. [ Links ]
38. Van der Vyver P, Paleker F, Vorster M. de Wet F. Root canal shaping using Nickel Titanium, M Wire and Gold Wire: a micro-computed tomographic comparative study of One Shape, Pro-Taper and Wave One Gold instruments in maxillary first molars. J Endod. 20129; 45(1):62-7 [ Links ]
39. Bürklein S, Schäfer E. Apically extruded debris with reciproting single-file and full sequence rotary instrumentation systems. J Endod. 2012; 38: 850-2. [ Links ]
40. Siqueira JJ. Microbial causes of endodontic flare-ups. Int Endod J. 2003; 36:453-63. [ Links ]
41. Siqueira JJ, Rôças I, Favieri A, Machado A, Gahyva S, Oliveira J, et al. Incidence of postoperative pain after intracanal procedures based on an antimicrobial strategy. J Endod. 2002; 28:457-60. [ Links ]
42. Türker S, Uzunoglu E, Aslan M. Evaluation of apically extruded bacteria associated with different nickel-titanium systems. J Endod. 2015; 41:953-5. [ Links ]
43. Reddy S, Hicks M. Apical extrusion of debris using two hand and two rotary instrumentation techniques. J Endod. 1994; 24:180-3. [ Links ]
44. McKendry D. Comparison of balanced forces, endosonic and step-back filing instrumentation techniques: quantification of extruded apical debris. J Endod. 1990; 16:24-7. [ Links ]
45. Luisi S, Zottis A, Piffer C, de Mello Vanzin A, Ligabue R. Apical extrusion of debris after hand, engine driven reciprocating and continuous preparation. Rev Odonto Ciência. 2010; 25:288-91. [ Links ]
46. Al-Omari M, Dummer P. Canal blockage and debris extrusion with eight preparation techniques. J Endod. 1995; 21:154-8. [ Links ]
 Correspondence:
Correspondence:
PJ van der Vyver
Tel: +27 (0)11 781 1020
Email: peetv@iafrica.com
