










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.73 n.1 Johannesburg Feb. 2018
CLINICAL REVIEW
Intraoral repair protocols for fractured metal-ceramic restorations - Literature review
A AslamI; SH HassanII; M NayyerIII; B AhmedIV
IBDS, M.Sc., CHPESenior Registrar, Department of Prosthodontics, AMC / AFID, National University of Medical Sciences (NUMS), Islamabad, Pakistan
IIBDS, FCPS, M.Sc. Med Edu Assistant Professor, Department of Prosthodontics, AMC / AFID, National University of Medical Sciences (NUMS), Islamabad, Pakistan
IIIBDS, M.Phil. Senior Lecturer, Department of Dental Materials, AMC / AFID, National University of Medical Sciences (NUMS), Islamabad, Pakistan
IVFCPS, BDS, FFD FRCSI-II (IRE), CMT, PhD Res. Professor, Department of Prosthodontics, Abottabad International Medical Institute, Abottabad, Pakistan
ABSTRACT
Metal ceramic restorations are still widely used for prosthodontic rehabilitation of compromised teeth and in general are durable and long lasting. However, post-fitting complications in metal-ceramic crowns and fixed partial dentures do occur. One of the most frequently encountered complications in metal-ceramic systems is the fracture of veneering porcelain, becoming a dental emergency, especially when located in the anterior region. Replacing the entire restoration may not be the most practical solution. Intraoral repair of the fractured porcelain offers an easy and cost-effective alternative. The exact protocol for repair varies with the type of fracture that has occurred. This paper provides an overview of various methods of repairing different types of porcelain fractures with an aim to help clinicians manage these dental emergencies in a more effective and conservative manner.
Key words: fracture, ceramics, intra-oral repair, veneering porcelain
1. INTRODUCTION
Metal ceramic restorations are still widely used for the prosthodontic rehabilitation of compromised teeth.1 A single metal-ceramic restoration simultaneously offers significant strength and optimal esthetics, owing, respectively, to the metal framework and the veneering porcelain .2 These restorations also demonstrate longer life and durability in clinical service as compared with all-ceramic and fibre-reinforced composite restorations.3-7 Survival rates of 98% after 5 years, 97% after 10 years and 85% after 15 years of intraoral service have been reported in the literature.8
Post-insertion problems of metal-ceramic crowns and fixed partial dentures do occur. Complications can either be biological, including secondary caries, pulp pathologies and periodontal problems, or technical, such as loss of retention, ceramic de-lamination or fractures.9 A retrospective study calculated a mean complication incidence of 27% in fixed dental prostheses between periods of five and 14 years of service,10 while a 25% incidence of problems in metal-ceramic prostheses serving for more than five years has been reported.11
The most frequently encountered issue with metal-ceramic restorations is the fracture of veneering porcelain.12 A systematic review13 calculated a 34% frequency of porcelain chipping in metal-ceramic fixed dental prostheses over a period of three years. In contrast, another study reported a mean chipping rate of only 2.9% after a five year observation period,14 whilst a prevalence of chipping of between 5% and 10% over 10 years of use has also been claimed.15 Despite these differences in the reported rates, it can be concluded that porcelain fractures in metal-ceramic restorations are problems which will face most dentists, usually in emergency situations.
Fracture of the veneering porcelain does not always mean a failure of the restoration.16 However, the misadventure becomes a dental emergency if located in the anterior region of the mouth, compromising aesthetics.17 In such a clinical scenario, replacing the entire restoration may not be the most practical solu-tion.18 Not only is the replacement time consuming and costly, but there is also the risk of damaging the prepared abutment while attempting to remove the restoration.19 Repairing the fractured porcelain intraorally, on the other hand, is relatively easy and offers a cost- and time-effective alternative to the patient and the dentist, adequately restoring both function and esthetics.20
Composite resins are the recommended materials for repairing porcelain fractures.16,21 The exact protocol for repair, however, varies depending upon the type of fracture that has occurred. This paper aims to provide an overview of various methods of repairing different types of porcelain fractures, albeit possibly in a temporary manner. The knowledge will help clinicians manage such dental emergencies in a more effective and conservative manner.
2. TYPES OF PORCELAIN FRACTURES
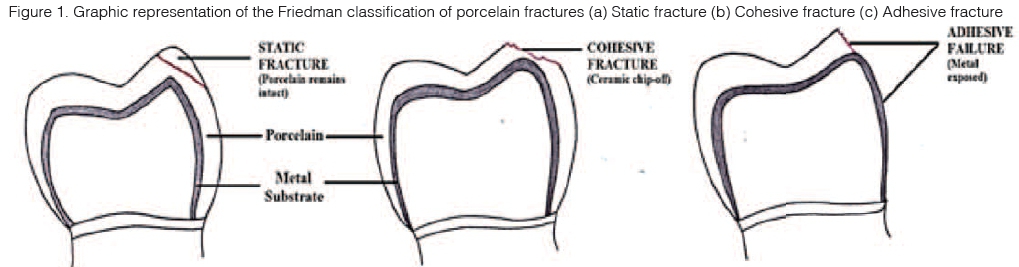
The type of porcelain fracture as well as the material involved will determine the repair protocol. Porcelain fractures have been classified in a number of different ways. A system for porcelain fractures, proposed by Friedman in 1998,22 describes three types of fractures (Figure 1):
i. Static Fracture - where a segment of porcelain fractures but remains in place
ii. Cohesive Fracture - fracture occurring within the body of porcelain; also known as chipping fracture
iii. Adhesive fracture - failure of the bonding interface between veneering and core porcelain or between porcelain and metal substrate
Another system is based on treatment need according to severity of the situation.13 The Heintz and Rousson13 classification has three grades :
1. Grade 1: Fractures requiring polishing only
2. Grade 2: Fractures requiring repair
3. Grade 3: Fractures requiring replacement
Although this classification system is practical and simple, it does not elaborate the criteria used to determine the severity of the fracture. In 2012, four criteria were added to the system to determine the need for replacement of the crown rather than the repair of fractured porcelain i.e. Grade 3 fractures :23
i. When fracture extends into a function area and repair is not possible
ii. When a recontouring attempt will badly alter the anatomic form
iii. When recontouring poses significant risk of thermal damage to the pulp
iv. When repair will result in poor aesthetics
Another classification system was put forward specifically for fractures occurring in metal-ceramic restorations.24 The authors suggested two categories simple fractures that involve only porcelain or complex fractures that result in exposure of metal substrate.
In this article, a combination of the classification systems proposed by Heintz and Rousson and Friedmann will be used.13,22
3. INTRAORAL REPAIR OF FRACTURED PORCELAIN
3.1 Isolation of the Tooth
Regardless of the type of repair being undertaken, it is recommended that the involved teeth be effectively isolated. The ideal means of achieving field isolation is the use of a rubber dam, either conventional or paint-on, ensuring isolation at the gingival margin. This not only helps control moisture but also protects the hard and soft tissues of the patient from undue damage.25,26 Moisture control is mandatory when procedures involving composite resins are undertaken.
3.2 Fractures Requiring Polishing (Static Fracture):
The easiest way to repair a static fracture of porcelain is to polish the fractured surface thoroughly. This is done to minimize surface flaws that might lead to future failure. Polishing also eliminates any probability of accumulation of microorganisms on the fractured surface. This method of repair can also be employed for small chippings of porcelain that do not affect aesthetics or function in the posterior region. In case of larger defects, more polishing time is required with subsequent generation of heat.23 Overheating may lead to plastic deformation of the porcelain,27 and overheating of the pulp...hence the use of air-water cooling is recommended to prevent further fracture of the ceramic mass.28
A variety of polishing techniques for porcelain have been described in the literature. Polishing kits are available that consist of diamond burs, abrasive rubber cups, felt wheels and polishing pastes.29 However, the published literature fails to recommend any standard surface-finishing protocol for porcelain and the choice depends largely on the preference of the clinician.30,31
3.3 Fractures Requiring Repair:
3.3.1 Cohesive Fracture:
Cohesive fracture, occurring within the body of porcelain, can be repaired intraorally by either recementing the broken porcelain fragment with a resin cement or by restoring the broken porcelain with composite resin.12 In both the situations, the restoration substrate first needs to be surface treated, as described below, to facilitate bonding between porcelain and the repair material.32 Despite this enhancement, the bond is not infallible.
Surface Modification:
The fractured porcelain surface is modified and a long bevel is created to facilitate optimal bonding and to achieve esthetically merging margins of porcelain and the repair material.33 If the broken porcelain chip is to be reattached, then that fragment must also be slightly beveled.
Surface Roughening:
The porcelain is then prepared for micromechanical bonding with the resin cement. The surfaces are first roughened with diamond burs, air abrasion using an intraoral sandblaster or by etching with Hydrofluoric (HF) acid.34-36 Table I summarizes the recommended roughening protocols for different types of ceramics. Etching with 2.5 - 10% HF acid for 60 seconds is the recommended method for the chairside surface preparation of fractured silicate ceramics.12 However, the use of HF acid demands extreme caution as any spills could be hazardous to the soft tissues.37 Acidulated phosphate fluoride (APF) in a concentration of 1.23% has also been used for surface etching.38 It is safe to the oral tissues but an etching time of at least 6 minutes on both sides is required.39 Alternatively, effective surface roughening can be achieved by using an intraoral sandblaster. Air abrasion with 50 micrometer aluminium oxide particles at an air pressure of 2-3 bars sufficiently roughens and activates the surface, improving its wettability.40,41 The major drawback of air abrasion is its potential to generate small surface flaws, which might lead to crack propagation in ceramics.42 For pure silicate ceramics, air abrasion should not be used as HF acid etching provides adequate surface roughening.43 For oxide based ceramics, however, acid etching does not produce sufficient surface roughening. Zirconia, in particular, is resistant to etching due to its dense polycrystalline structure and lack of a glass phase.44-46 This makes air particle abrasion the method of choice for surface roughening of these materials. Surface damage in such cases can be minimized by decreasing the air pressure to 0.5 bars without compromising the results.12
More recently, lasers have been used as an alternative to HF acid etching and air abrasion to achieve a roughened ceramic surface.47,48 Lasers such as CO2, erbium: yttrium-aluminium-garnet (Er: YAG) and neodymium: yttrium-aluminium-garnet (Nd: YAG) have been used on ceramic surfaces to promote micromechanical adhesion.49 Nd:YAG laser melts the ceramic surface which, upon solidification, results in a surface with blisters.47 CO2 laser, in contrast, results in the formation of conchoidal tears in the ceramic surface that aid in mechanical retention.50 Published literature suggests that Er: YAG laser surface roughening does not yield a durable resin-ceramic bond51,52 and although CO2 and Nd:YAG lasers show better results53,54, the effect is inferior to that achieved with HF acid.55 The generation of heat also contradicts the use of some lasers.
Surface Treatment:
Irrespective of the method used for roughening, the surfaces must also be treated with a coupling agent that would promote chemical bonding between ceramic and resin (Table II). Usually silane coupling agents are employed.61 These are bifunctional molecules, one end binding to the silanol group present in the silicate material through a condensation reaction while the other end binds to the resin via an addition polymerization reaction.32 Silane also increases the wettability of the surface, thereby allowing enhanced surface penetration of the resin.62 The most widely used silane is 3-Methacryloxypropyltrimethoxysilane (MPS).
Oxide ceramic materials lack the silanol groups and are unable to bond with silane.12 This can be overcome by 'silicatizing' them beforehand. The procedure involved is called tribochemical coating,63 made possible by the development of a chairside system "CoJet silicate-ceramic surface treatment system, 3M ESPE".64 It involves aluminium oxide particles 30 micrometer in size doped with silica. When the surface is bombarded with these particles, it not only helps in roughening the ceramic but also incorporates silica into the ceramic.44, 65 This silicatized ceramic is then able to bond with silane.
Alternatively, primers may be used for oxide ceramics. These are bifunctional phosphate monomers capable of bonding to oxide ceramics on one side and to the resin on the other side.66 One such monomer is 10-meth-acryloyloxy-decyl dihydrogenphosphate (MDP). Primers are often added to resin materials67 which are then referred to as modified resins.12 They eliminate the need for separate treatment with primers. Panavia68,69 is one such MDP-containing resin luting cement, widely used for cementation of indirect restorations. Certain manufacturers provide a combination of silane and primers in a single product. So far, MDP-containing resin cements appear to be the most effective, owing to the chemical interaction between the hydroxyl groups of the oxide ceramic surface and the MDP phosphate esters.60
Another (laboratory) method to condition the surface of zirconia ceramics is selective infiltration etching (SIE).32,70 In SIE, the zirconia surface is covered with a glass-containing conditioner and heated to a temperature above the glass transition temperature of the conditioner. Once cooled to room temperature, the glass is rinsed in an acid bath. The process results in the formation of a new retentive surface, which when combined with a silane coupling agent, yields significant improvement in resin-zirconia bond.71,72 However, studies reporting the clinical efficacy of SIE need to be carried out before any recommendations can be made.
Repair:
In rare cases where the patient is able to salvage and produce the broken porcelain fragment, the fragment may be recemented using a resin cement. This, however, requires careful evaluation of the fragment to assess whether it is suitable for reattachment. The fragment and the porcelain substrate should both first be surface treated as described above. Recementation can then be achieved with the help of a resin cement. If the broken porcelain fragment is large, recementation is not recommended as the repair resin might impair the correct positioning of the fragment.25
Small chipped off parts can be built up using composite resins. Porcelain is first roughened and surface treated. The lost part is restored using a nanohybrid composite restorative material. A layering technique may be used to achieve optimum aesthetics,73 reducing the undesirable effect of the underlying metal shining through..
The third option to repair a cohesive porcelain fracture is to bond a new ceramic veneer on to the existing restoration. To achieve this, the existing restoration will have to be modified. The entire porcelain is removed with the help of rotary instruments and preparation margins are created.74 Impressions are recorded and sent to a laboratory for the fabrication of a porcelain veneer.75 The patient can be provided with temporary restorations until the next appointment. When the final restorations are received, they can be cemented using a resin based adhesive.
Cerec (CAD/CAM) system can be used to fabricate porcelain veneers at the chairside by trimming a single block of porcelain. A study on 617 Cerec veneers reported that CAD/Cam veneers fabricated with the Cerec system demonstrated a high survival rate of 94% after nine years and favourable clinical results.76 A number of materials can be used by the Cerec system including VITA Mark II (Vident, Brea, California), ProCad (Ivoclar Vivadent, Inc., Amherst, New York), In-Ceram Alumina and Spinell (VITA Zahnfabrik, Bad Säckingen, Germany).
3.3.2 Adhesive Fracture:
Adhesive failure of porcelain is the failure of the bonding interface. The failure may occur between the veneer layer and the core porcelain, or between the porcelain and the metal substrate resulting in exposure of the underlying metal framework.15 Intraoral repair of such a damage can be quite challenging as it may prove difficult for the clinician to mask the opaque core or framework colour with a ceramic veneer, thereby restricting the aesthetic outcome.12,74 Adhesive failure between core and veneer porcelain is managed in the same way as cohesive porcelain fractures. Where the metal substrate is exposed, the repair protocol needs to be slightly modified as described below.
Surface Roughening for Micromechanical Bonding:
The metal surface should be roughened using air abrasion as described for oxide ceramics. Etching with an acid is not sufficient since no currently available acid is capable of breaking metallic bonds.43 Undercuts can also be created to promote mechanical retention. Lasers have also been used as a means of etching the alloy surface. In comparison with air abrasion, alloy treatment with XeCl lasers showed improved bond strengths to composite resins77 whereas treatment with the Er:YAG laser did not yield effective surface roughening sufficient to promote the metal-resin bond.41,78
Surface Treatment for Chemical Bonding:
Similar to oxide ceramics, metal needs to be silicatized using tribochemical coating.79 To promote chemical bonding between the silica-coated metal and the repair material, a silane coupling agent must be used. Higher bond strengths between metal and resin have been reported if the metal is pretreated with silica.80,81 Alternatively, alloy primers can create a direct chemical bond between metals and resin, without the need for any silicatization. These primers contain carboxylic or phosphoric acid functional monomers which react with oxides present on the metal surface.8283 Products combining both silane and primers are recommended for enhancing bond strength in the intraoral repair of base metal alloys bonded to ceramic restorations where the metal has been exposed.84
A newer method to enhance bonding between metal and resin is silica-lasing. It involves coating the metal with an opaque porcelain slurry and irradiating it with a laser such as Nd:YAG or Er:YAG.48 Madani et al. reported that laser treatment of alloys in conjunction with air-borne particle abrasion yields significantly better bond strengths than laser treatment alone.41 However, silica lasing is a newer method and no appreciable data exists regarding its clinical performance.
Repair with Composite Resin: To repair an adhesive fracture with composite material, a more opaque shade is selected for the first layers to emulate the dentin and to mask the colour of underlying metal, whereas lighter and more translucent shades are then utilized for surface restoration.25 The use of fibre-reinforced composites has been recommended for the repair of metal-ceramic crowns and fixed partial dentures85 as they offer increased fatigue resistance, thereby increasing the longevity of the repair.86
A laboratory-fabricated composite or ceramic veneer can also be bonded to the facial surface of the damaged prosthesis with the help of a resin based cement.87 This is a more feasible clinical option if complete porcelain delamination occurs.
4. LONG TERM SUCCESS OF INTRAORAL REPAIR
Studies reporting the long-term success of repaired restorations are rather scarce. Özcan and Niedermeier reported an 89% survival rate over a mean period of 36.4 months of metal-ceramic restorations repaired intraorally with composite resins.88 Another study reported a 97.6% survival rate for metal-ceramic restorations repaired with composite after 3.5 years of clinical service.89 There exists a need for more in vivo studies with adequate follow-ups to evaluate the long-term success of such repairs.
5. RECOMMENDATIONS
See figure below.
6. CONCLUSION
Fractures involving the veneering porcelain of metal-ceramic restorations are routinely encountered in dental practice. The decision to repair or replace such a restoration revolves around a number of different factors including time and cost. While replacing the failed restoration may be the ideal treatment, it is not always practical. Repair of fractured porcelain should be attempted whenever possible. Repair protocols further vary depending upon the type of porcelain fracture. To ensure clinical success and longevity of the restorations, a clinician must be well-versed with the various surface conditioning and surface treatments required to promote bond formation between the resin and the porcelain. This will help in optimizing the performance of metal-ceramic restorations as well as in achieving better patient satisfaction.
Acronyms
MDP :10-methacryloyloxy-decyl dihydrogen phosphate
MPS : 3-Methacryloxypropyltrimethoxysilane
SIE : selective infiltration etching
References
1. Zarone F, Russo S, Sorrentino R. From porcelain-fused-to-metal to zirconia: clinical and experimental considerations. Dent Mater 2011;27:83-96. [ Links ]
2. KS KM, Stratos A, Hirayama H, K KK, Touloumi F, Oishi Y. Fracture resistance of metal ceramic restorations with two different margin designs after exposure to masticatory simulation. J Prosthet Dent 2009;102(3):172-8. [ Links ]
3. Shadid R, Sadaqah N, Abu-Nab'a L, Al-Omari W. Porcelain fracture of metal-ceramic tooth-supported and implant-supported restorations: A review. OJST. 2013;3 :411-8. [ Links ]
4. Bjarni Elvar Pjeturssona, Sailer I, Makarov NA, Zwahlen M, Thoma DS. All-ceramic or metal-ceramic tooth-supported fixed dental pros-theses (FDPs) A systematic review of the survival and complication rates. Part II: Multiple-unit FDPs. Dent Mater. 2015;31:624-39. [ Links ]
5. Sasse M, Kern M. Survival of anterior cantilevered all-ceramic resin-bonded fixed dental prostheses made from zirconia ceramic. J Dent 2014;42:660-3. [ Links ]
6. C.M.vanHeumen C, JohannaTanner, JanW.V.vanDijken, Pikaar R, V.J.Lassila L, H.J.Creugers N, et al. Five-year survival of 3-unit fiber-reinforced composite fixed partial dentures in the posterior area. Dent Mater. 2010;26:954-60. [ Links ]
7. Vallittu PK. Survival rates of resin-bonded, glass fiber-reinforced composite fixed partial dentures with a mean follow-up of 42 months: A pilot study. J Prosthet Dent. 2004;91:241-6. [ Links ]
8. Eliasson A, Arnelund C, Johansson A. A clinical evaluation of cobalt chromium metal ceramic fixed partial dentures and crowns: A three to seven year retrospective study. J Prosthet Dent. 2007;98:06-16. [ Links ]
9. Zafar N, Ghani F. Common post-fitting complications in tooth-supported fixed-fixed design metal-ceramic fixed dental prostheses. Pak J Med Sci. 2014;30(3):619-25. [ Links ]
10. Goodacre C, G GB, Rungcharassaeng K, Kan J. Clinical complications in fixed prosthodontics. J Prosthet Dent. 2003;90:31-41. [ Links ]
11. F FG, Memon M. Complications in metal ceramic fixed dental pros-theses among patients reporting to a teaching dental hospital. JLUMHS 2010;9(1):17-22. [ Links ]
12. Kimmich M, Stappert CF. Intraoral treatment of veneering porcelain chipping of fixed dental restorations: a review and clinical application. J Am Dent Assoc. 2013;144(1):31-44. [ Links ]
13. Heintze SD, Rousson V. Survival of zirconia- and metal-supported fixed dental prostheses: a systematic review. Int J Prosthodont. 2010;23(6):493-502. [ Links ]
14. Sailer I, Pjetursson BE, Zwahlen M, Hammerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin Oral Implants Res. 2007;18 Suppl 3:86-96. [ Links ]
15. Özcan M. Fracture reasons in ceramic-fused-to-metal restorations. J Oral Rehabil. 2003;30(3):265-9. [ Links ]
16. Özcan M. Evaluation of alternative intra-oral repair techniques for fractured ceramic-fused-to-metal restorations. J Oral Rehabil. 2003;30(2):194-203. [ Links ]
17. Haneda I, Almeida-Junior A, Fonseca R, Adabo G. Intraoral repair in metal-ceramic prosthesis: a clinical report. Revista de Odontologia da Universidade Cidade de São Paulo 2009;21(3):282-7. [ Links ]
18. Meshramkar R. A review on repair of fracture porcelain. IJDE. 2010;3(3):133-8. [ Links ]
19. Macura A, Kasperski J, Urbaniak M, Klimek A. Materials and methods used for repairing damaged veneering porcelain in permanent complex prosthetic restorations - review of literature. J Stoma. 2013;66(2):221-30. [ Links ]
20. Al-Moaleem M, Al-Qahtani NM. A combination of intra and extra oral technique for repairing a multi-unit metal ceramic fixed partial den-ture2012. [ Links ]
21. Prabu P, Prabu N. Composite as a ceramic repair material - an in vitro study. JIADS. 2010;1(4):27-32. [ Links ]
22. Friedman M. A 15-Year Review of porcelain veneefailure - a clinician's observations. Compend Contin Educ Dent 1998;19:625-8. [ Links ]
23. Anusavice KJ. Standardizing failure, success, and survival decisions in clinical studies of ceramic and metal-ceramic fixed dental prostheses. Dent Mater. 2012;28(1):102-11. [ Links ]
24. Blum IR, Jagger DC, Wilson NH. Defective dental restorations: to repair or not to repair? Part 2: All-ceramics and porcelain fused to metal systems. Dent Update. 2011;38(3):150-2, 4-6, 8. [ Links ]
25. Raposo LH, Neiva NA, da Silva GR, Carlo HL, da Mota AS, do Prado CJ, et al. Ceramic restoration repair: report of two cases. J Appl Oral Sci. 2009;17(2):140-4. [ Links ]
26. Abd Wahab MHK, Bakar WZW, Husein A. Different surface preparation techniques of porcelain repaired with composite resin and fracture resistance. Journal of Conservative Dentistry : JCD. 2011;14(4):387-90. [ Links ]
27. Nidhal Sahib M. Correlation between surface roughness and fracture toughness of dental porcelain treated with different polishing materials and glazing techniques ءدارصرال ءيحدل ل ا ٠٠ ديب هى,'لعلا ل قص ل'وعيملت؛ا داوم ف'خمب جل'عملا نانس'لا فزخل ،؛■١. AL-TAQANI ينقتلا ةلجم. 2010;23(5):30-40. [ Links ]
28. Petrescu EL, Negrutiu MI, Pop DM, Rominu RO, Topala FI, Fabricky M, et al. Comparative and non-invasive study of two different ceramic materials. REVISTA DE CHIMIE. 2012;63(2):179-81. [ Links ]
29. Flury S, Lussi A, Zimmerli B. Performance of different polishing techniques for Direct CAD/CAM ceramicrestorations. Operative Dentistry. 2010;35(4):470-81. [ Links ]
30. da Silva TM, Salvia ACRD, de Carvalho RF, Pagani C, da Rocha DM, da Silva EG. Polishing for glass ceramics: Which protocol? Journal of Prosthodontic Research. 2014;58(3):160-70. [ Links ]
31. Coskun Akar G, Pekkan G, Çal E, Eskitasçioglu G, Òzcan M. Effects of surface-finishing protocols on the roughness, color change, and translucency of different ceramic systems. The Journal of Prosthetic Dentistry. 2014;112(2):314-21. [ Links ]
32. Lung CYK, Matinlinna JP. Aspects of silane coupling agents and surface conditioning in dentistry: An overview. Dental Materials. 2012;28(5):467-77. [ Links ]
33. Malhotra N, Acharya S. Conservative approach for esthetic repair of fractured ceramic facing in ceramic-fused-to-metal crowns: A case series. Compend Contin Educ Dent. 2012;29(6):2-13. [ Links ]
34. Attia A. Influence of surface treatment and cyclic loading on the durability of repaired all-ceramic crowns. J Appl Oral Sci. 2010;18(2):194-200. [ Links ]
35. Colares RC, Neri JR, Souza AM, Pontes KM, Mendonca JS, Santiago SL. Effect of surface pretreatments on the microtensile bond strength of lithium-disilicate ceramic repaired with composite resin. Braz Dent J. 2013;24(4):349-52. [ Links ]
36. Neis CA, Albuquerque NL, Albuquerque Ide S, Gomes EA, Souza-Filho CB, Feitosa VP, et al. Surface treatments for repair of feldspath-ic, leucite - and lithium disilicate-reinforced glass ceramics using composite resin. Braz Dent J. 2015;26(2):152-5. [ Links ]
37. Özcan M, Allahbeickaraghi A, Dundar M. Possible hazardous effects of hydrofluoric acid and recommendations for treatment approach: a review. Clin Oral Investig. 2012;16(1):15-23. [ Links ]
38. Tian T, Tsoi JK-H, Matinlinna JP, Burrow MF. Aspects of bonding between resin luting cements and glass ceramic materials. Dental Materials. 2014;30(7):e147-e62. [ Links ]
39. Kukiattrakoon B, Thammasitboon K. Optimal acidulated phosphate fluoride gel etching time for surface treatment of feldspathic porcelain: on shear bond strength to resin composite. European Journal of Dentistry. 2012;6(1):63-9. [ Links ]
40. Borges GA, Sophr AM, de Goes MF, Sobrinho LC, Chan DC. Effect of etching and airborne particle abrasion on the microstructure of different dental ceramics. J Prosthet Dent. 2003;89(5):479-88. [ Links ]
41. Madani AS, Astaneh PA, Nakhaei M, Bagheri HG, Moosavi H, Alavi S, et al. Effectiveness of silica-lasing method on the bond strength of composite resin repair to Ni-Cr alloy. J Prosthodont. 2015;24(3):225-32. [ Links ]
42. Zhang Y, Lawn BR, Malament KA, Van Thompson P, Rekow ED. Damage accumulation and fatigue life of particle-abraded ceramics. Int J Prosthodont. 2006;19(5):442-8. [ Links ]
43. Della Bona A, Anusavice KJ. Microstructure, composition, and etching topography of dental ceramics. Int J Prosthodont. 2002;15(2):159-67. [ Links ]
44. Cheng HCK, Tsoi JKH, Zwahlen RA, Matinlinna JP. Effects of silica-coating and a zirconate coupling agent on shear bond strength of flowable resin-zirconia bonding. International Journal of Adhesion and Adhesives. 2014;50(0):11-6. [ Links ]
45. Özcan M, Dündar M, Erhan Çõmlekoglu M. Adhesion concepts in dentistry: tooth and material aspects. Journal of Adhesion Science and Technology. 2012;26(24):2661-81. [ Links ]
46. Sanli S, Çömlekoglu MD, Çömlekoglu E, Sonugelen M, Pamir T, Darvell BW. Influence of surface treatment on the resin-bonding of zirconia. Dental Materials. 2015;31(6):657-68. [ Links ]
47. Paranhos MP, Burnett LH, Jr., Magne P. Effect Of Nd:YAG laser and CO2 laser treatment on the resin bond strength to zirconia ceramic. Quintessence Int. 2011;42(1):79-89. [ Links ]
48. Sadat Madani A, Astaneh PA, Shahabi S, Nakhaei MR, Bagheri HG, Chiniforush N. Influence of different power outputs of intraoral Nd:YAG laser on shear bond strength of a resin cement to nickel-chromium dental alloy. Lasers Med Sci. 2013;28(1):229-34. [ Links ]
49. Akin H, Ozkurt Z, Kirmali O, Kazazoglu E, Ozdemir AK. Shear bond strength of resin cement to zirconia ceramic after aluminium oxide sandblasting and various laser treatments. Photomed Laser Surg. 2011;29(12):797-802. [ Links ]
50. Ural Ç, Külünk T, Külünk S, Kurt M. The effect of laser treatment on bonding between zirconia ceramic surface and resin cement. Acta Odontologica Scandinavica. 2010;68(6):354-9. [ Links ]
51. Foxton RM, Cavalcanti AN, Nakajima M, Pilecki P, Sherriff M, Melo L, et al. Durability of resin cement bond to aluminium oxide and zirco-nia ceramics after air abrasion and laser treatment. J Prosthodont. 2011;20(2):84-92. [ Links ]
52. Saraç D, Saraç YS, Külünk S, Erkocak A. Effect of various surface treatments on the bond strength of porcelain repair. The International Journal of Periodontics & Restorative Dentistry. 2012;33(4):e120-6. [ Links ]
53. Akyil MJ, Uzun IH, Bayindir F. Bond strength of resin cement to yttrium-stabilized tetragonal zirconia ceramic treated with air abrasion, silica coating, and laser irradiation. Photomedicine and Laser Surgery. 2010;28(6):801-8. [ Links ]
54. Kasraei S, Rezaei-Soufi L, Heidari B, Vafaee F. Bond strength of resin cement to CO2 and Er: YAG laser-treated zirconia ceramic. Restorative Dentistry & Endodontics. 2014;39(4):296-302. [ Links ]
55. Shirinzad M, Fekrazad R, Rezaei-Soufi L, Yarmohammadi E, Jalalian S. Evaluation of shear bond strength of composite to feldspathic porcelain after porcelain surface treatment with CO2 and Er: Yag lasers. Journal of Islamic Dental Association of Iran. 2013;25(2):110-5. [ Links ]
56. Colares RCR, Neri JR, Souza AMBd, Pontes KMdF, Mendonca JS, Santiago SL. Effect of surface pretreatments on the microtensile bond strength of lithium-disilicate ceramic repaired with composite resin. Brazilian Dental Journal. 2013;24(4):349-52. [ Links ]
57. Neis CA, Albuquerque NLG, Albuquerque IdS, Gomes EA, Souza-Filho CBd, Feitosa VP, et al. Surface treatments for repair of feld-spathic, leucite-and lithium disilicate-reinforced glass ceramics using composite resin. Brazilian Dental Journal. 2015;26(2):152-5. [ Links ]
58. Ho G, Matinlinna J. Insights on ceramics as dental materials. Part II: Chemical surface treatments. Silicon. 2011;3(3):117-23. [ Links ]
59. Han I-H, Kang D-W, Chung C-H, Choe H-C, Son M-K. Effect of various intraoral repair systems on the shear bond strength of composite resin to zirconia. The Journal of Advanced Prosthodontics. 2013;5(3):248-55. [ Links ]
60. Papia E, Larsson C, du Toit M, Vult von Steyern P. Bonding between oxide ceramics and adhesive cement systems: a systematic review. J Biomed Mater Res B Appl Biomater. 2014;102(2):395-413. [ Links ]
61. Madani M, Chu FC, McDonald AV, Smales RJ. Effects of surface treatments on shear bond strengths between a resin cement and an alumina core. J Prosthet Dent. 2000;83(6):644-7. [ Links ]
62. Matinlinna JP, Lassila LV, Ozcan M, Yli-Urpo A, Vallittu PK. An introduction to silanes and their clinical applications in Dentistry. Int J Prosthodont. 2004;17(2):155-64. [ Links ]
63. Heikkinen TT, Lassila LV, Matinlinna JP, Vallittu PK. Effect of operating air pressure on tribochemical silica-coating. Acta Odontol Scand. 2007;65(4):241-8. [ Links ]
64. 3M ESPE Cojet System [cited 2015 6/2/2015]. Available from: http://multimedia.3m.com/mws/media/386161O/cojet-adhesive-system-technical-profile.pdf [ Links ]
65. Atsu SS, Kilicarslan MA, Kucukesmen HC, Aka PS. Effect of zirconium-oxide ceramic surface treatments on the bond strength to adhesive resin. J Prosthet Dent. 2006;95(6):430-6. [ Links ]
66. Chen L, Suh B. Bonding of resin materials to all-ceramics: A review. Current Research in Dentistry 2012;3(1):7-17. [ Links ]
67. I kemura K, Tanaka H, Fujii T, Deguchi M, Negoro N, Endo T, et al. Design of a new, multi-purpose, light-curing adhesive comprising a silane coupling agent, acidic adhesive monomers and dithiooc-tanoate monomers for bonding to varied metal and dental ceramic materials. Dent Mater J. 2011;30(4):493-500. [ Links ]
68. Blatz MB, Sadan A, Martin J, Lang B. In vitro evaluation of shear bond strengths of resin to densely-sintered high-purity zirconium-oxide ceramic after long-term storage and thermal cycling. J Pros-thet Dent. 2004;91(4):356-62. [ Links ]
69. Manso AP, Silva NR, Bonfante EA, Pegoraro TA, Dias RA, Carvalho RM. Cements and adhesives for all-ceramic restorations. Dent Clin North Am. 2011;55(2):311-32, ix. [ Links ]
70. Aboushelib MN, Feilzer AJ, Kleverlaan CJ. Bonding to zirconia using a new surface treatment. J Prosthodont. 2010;19(5):340-6. [ Links ]
71. Aboushelib MN, Kleverlaan CJ, Feilzer AJ. Selective infiltration-etching technique for a strong and durable bond of resin cements to zirconia-based materials. J Prosthet Dent. 2007;98(5):379-88. [ Links ]
72. Aboushelib MN, Matinlinna JP. Combined novel bonding method of resin to zirconia ceramic in dentistry: a pilot study. Journal of Adhesion Science and Technology. 2011;25(10):1049-60. [ Links ]
73. Fahl N. Mastering composite artistry to create anterior masterpieces - Part 2. J Cosmetic Dent. 2011;26(4):42-55. [ Links ]
74. Galiatsatos AA. An indirect repair technique for fractured metal-ceramic restorations: A clinical report. J Prosthet Dent. 2005;93(4):321-3. [ Links ]
75. Wady AF, Paleari AG, Queiroz TP, Margonar R. Repair technique for fractured implant-supported metal-ceramic restorations: A clinical report. Journal of Oral Implantology. 2014;40(5):589-92. [ Links ]
76. Wiedhahn K, Kerschbaum T, Fasbinder DF. Clinical long-term results with 617 Cerec veneers: a nine-year report. International Journal of Computerized Dentistry. 2005;8(3):233-46. [ Links ]
77. Murray AK, Attrill DC, Dickinson MR. The effects of XeCl laser etching of Ni-Cr alloy on bond strengths to composite resin: a comparison with sandblasting procedures. Dent Mater. 2005;21(6):538-44. [ Links ]
78. Kunt GE, Guler AU, Ceylan G, Duran I, Ozkan P, Kirtiloglu T. Effects of Er:YAG laser treatments on surface roughness of base metal alloys. Lasers Med Sci. 2012;27(1):47-51. [ Links ]
79. Frankenberger R, Kramer N, Sindel J. Repair strength of etched vs silica-coated metal-ceramic and all-ceramic restorations. Oper Dent. 2000;25(3):209-15. [ Links ]
80. dos Santos JG, Fonseca RG, Adabo GL, dos Santos Cruz CA. Shear bond strength of metal-ceramic repair systems. J Prosthet Dent. 2006;96(3):165-73. [ Links ]
81. Haneda IG, Fonseca RG, de Almeida JG, Cruz CA, Adabo GL. Shear bond strength of metal-ceramic repair systems. Gen Dent. 2009;57(6):644-51; quiz 52-3, 595, 680. [ Links ]
82. Almilhatti HJ, Giampaolo ET, Vergani CE, Machado AL, Pavarina AC, Betiol EA. Adhesive bonding of resin composite to various Ni-Cr alloy surfaces using different metal conditioners and a surface modification system. J Prosthodont. 2009;18(8):663-9. [ Links ]
83. Sarafianou A, Seimenis I, Papadopoulos T. Effectiveness of different adhesive primers on the bond strength between an indirect composite resin and a base metal alloy. J Prosthet Dent. 2008;99(5):377-87. [ Links ]
84. Antoniadou M, Kern M, Strub JR. Effect of a new metal primer on the bond strength between a resin cement and two high-noble alloys. J Prosthet Dent. 2000;84(5):554-60. [ Links ]
85. Vallittu PK. Use of woven glass fibres to reinforce a composite veneer. A fracture resistance and acoustic emission study. J Oral Re-habil. 2002;29(5):423-9. [ Links ]
86. Özcan M, van der Sleen JM, Kurunmaki H, Vallittu PK. Comparison of repair methods for ceramic-fused-to-metal crowns. J Prosthodont. 2006;15(5):283-8. [ Links ]
87. Ömar H, Atta O, El-Mowafy O, Khan SA. Effect of CAD-CAM porcelain veneers thickness on their cemented color. J Dent. 2010;38 Suppl 2:e95-9. [ Links ]
88. Özcan M, Niedermeier W. Clinical study on the reasons for and location of failures of metal-ceramic restorations and survival of repairs. Int J Prosthodont. 2002;15(3):299-302. [ Links ]
89. Özcan M. Longevity of repaired composite and metal-ceramic restorations: 3.5-year clinical study. 2006. [ Links ]
 Correspondence:
Correspondence:
Ayesha Aslam
Department of Prosthodontics, AMC / AFID, National University of Medical Sciences (NUMS)
Islamabad, Pakistan
dr.ayesha.aslam@hotmail.com

{kind=link}
{kind=link}
{kind=link}
{kind=link}