










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 n.3 Pretoria Mar. 2013
GUIDELINE
Guideline for the management of acute asthma in children: 2013 update - Part 3: March 2013
S KlingI; H J ZarIV; M E LevinV; R J GreenVI; P M JeenaVII; S M RisengaIX; S A ThulaVIII; P GoussardII; R P GieIII; for the South African Childhood Asthma Working Group (SACAWG)
IDepartment of Paediatrics and Child Health, Stellenbosch University and Tygerberg Children's Hospital, Parow, Cape Town, MB ChB, DCH (SA), FCPaed (SA), MMed (Paed), MPhil (Applied Ethics)
IIDepartment of Paediatrics and Child Health, Stellenbosch University and Tygerberg Children's Hospital, Parow, Cape Town, MB ChB, MMed (Paed)
IIIDepartment of Paediatrics and Child Health, Stellenbosch University and Tygerberg Children's Hospital, Parow, Cape Town, R P Gie, MB ChB, FCPaed (SA), MMed (Paed)
IVDepartment of Paediatrics and Child Health, Red Cross War Memorial Children's Hospital, University of Cape Town, MB BCh, BC Peds (USA), FCP (SA), BC Ped Pulm (USA), PhD
VDepartment of Paediatrics and Child Health, Red Cross War Memorial Children's Hospital, University of Cape Town, MB ChB, FCPaed (SA), Dip Allerg (SA), MMed (Paed), PhD
VIDepartment of Paediatrics and Child Health, Steve Biko Academic Hospital, University of Pretoria, PhD, FRCP
VIIDepartment of Paediatrics and Child Health, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, MB ChB, FCPaed (SA), Cert Pulmonol
VIIIDepartment of Paediatrics and Child Health, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, MB ChB, FCPaed (SA)
IXDepartment of Paediatrics and Child Health, University of Limpopo, Polokwane, MB ChB, MMed (Paed), Dip Allerg (SA), Cert Pulmonol (SA) Paed
ABSTRACT
BACKGROUND: Acute asthma exacerbations remain a common cause of hospitalisation and healthcare utilisation in South African children.
AIM: To update the South African paediatric acute asthma guidelines according to current evidence, and produce separate recommendations for children above and below 2 years of age.
METHODS: A working group of the South African Childhood Asthma Group was established to review the published literature on acute asthma in children from 2000 to 2012, and to revise the South African guidelines accordingly.
RECOMMENDATIONS: Short-acting inhaled bronchodilators remain the first-line treatment of acute asthma. A metered dose inhaler with spacer is preferable to nebulisation for bronchodilator therapy to treat mild to moderate asthma. Two to four puffs of a short-acting bronchodilator given every 20 - 30 minutes, depending on clinical response, should be given for mild attacks; up to 10 puffs may be needed for more severe asthma. Children with severe asthma or oxygen saturation (SpO2) <92% should receive oxygen and frequent doses of nebulised β2-agonists, and be referred to hospital. Nebulised ipratropium bromide (via nebulisation or multidosing via pMDI-spacer combination) should be added if there is a poor response to three doses of β2-agonist or if the symptoms are severe. Early use of corticosteroids reduces the need for hospital admission and prevents relapse; oral therapy is preferable. Assessment of acute asthma in children below the age of 2 years can be difficult, and other causes of wheezing must be excluded. Treatment of acute asthma in this age group is similar to that of older children.
CONCLUSION: Effective therapy for treatment of acute asthma - primarily inhaled short-acting β2-agonists, oral corticosteroids and oxygen with appropriate delivery systems - should be available in all healthcare facilities and rapidly instituted for treatment of acute asthma in children.
ENDORSEMENT: The guideline document is endorsed by the Allergy Society of South Africa (ALLSA), the South African Thoracic Society (SATS), the National Asthma Education Programme (NAEP), the South African Paediatric Association (SAPA) and the South African Academy of Family Practice.
Asthma is the most common chronic disease of childhood. Acute asthma exacerbations cause considerable morbidity and health cost utilisation, as well as substantial mortality. Asthma exacerbations are an indication of loss of asthma control and should prompt re-evaluation of the child's illness and the use of controller therapy. The last South African paediatric acute asthma guidelines were published in 1993.[1] The current revision was prompted by the following:
- subsequent publication of several studies of different management strategies for acute asthma
- changes in international guidelines
- updated recommendations for the recognition and assessment of acute severe asthma
- increasing recognition of the importance of preschool wheezing, and the need for different treatment strategies in very young compared with older children
- the development of new formulations and asthma drugs.

1. Methodology
The acute asthma working group guideline was developed as part of the South African Childhood Asthma Working Group (SACAWG) guideline, with the chronic management guideline published in 2009.[2] A Pubmed literature search was performed for English language publications on treatment of acute asthma in children, from 2000 to 2012 inclusive. The search strategy used the following terms: 'asthma' and 'child' and 'treatment', and 'acute asthma attack' and 'status asthmaticus'.
Although many of the drugs used in the treatment of acute asthma in children are used off-label, the recommendations are based on the best available evidence and the drugs are in common use.
1.1 Levels of evidence
The strategies recommended in this guideline are classified according to the evidence categories in Table 1 and denoted as evidence A, B, C or D.

1.2 Definitions
Acute asthma is characterised by a progressive increase in shortness of breath, cough, wheeze or tight chest that does not respond to the patient's usual bronchodilator therapy.
Mild asthma exacerbations are just outside the normal range of variation for an individual patient and are difficult to distinguish from transient loss of asthma control.[4]
Moderate asthma exacerbations are defined as at least one of the following occurring for at least 2 days without the need for systemic corticosteroids (CS): increasing asthma symptoms, worsening lung function, and/or increased rescue bronchodilator use.[4] Emergency department (ED) visits not requiring CS are classified as moderate disease exacerbations.
Severe asthma exacerbations necessitate urgent action by the patient/parent and doctor to prevent a serious outcome, such as hospitalisation or death. The definition requires either an asthma-related hospitalisation or a visit to the ED or an urgent care facility, together with treatment with systemic CS for at least 3 days.[4] The features of a severe asthma exacerbation are: inability to complete sentences in one breath and/or too breathless to talk or feed; use of accessory muscles of respiration; tachycardia; tachypnoea; agitation; oxygen saturations (SpO2) <92%; peak expiratory flow rate (PEFR) 33 - 50% best or predicted.[3]
Acute severe asthma, formerly known as status asthmaticus, is defined as severe asthma unresponsive to repeated courses of β2 agonist therapy. It is a medical emergency that requires immediate recognition and treatment.
Near-fatal asthma is acute severe asthma associated with a respiratory arrest or hypercarbia.[5]
2. Assessment
The management of acute asthma depends on the assessment of severity. The initial quick assessment should determine whether the child shows any risk factors for (Table 2) or symptoms or signs of life-threatening asthma (Table 3).[3,6] The PEFR can usually only be measured in children older than 6 years, and who are accustomed to having their PEF measured.

Before children can receive appropriate treatment for acute asthma, the severity of their symptoms must be assessed accurately. The following clinical signs should be recorded:
- pulse rate
- respiratory rate and degree of breathlessness (ability to complete sentences in one breath or to feed)
- use of accessory muscles of respiration
- amount of wheezing (how audible it is)
- degree of agitation and level of consciousness.
Increasing tachycardia generally denotes worsening asthma, whereas a fall in heart rate in life-threatening asthma is a pre-terminal event. Although wheezing initially becomes more apparent as airway obstruction increases, severe airway obstruction decreases air flow, with wheezing becoming softer and then diminishing completely (silent chest).
It is important to realise that clinical signs correlate poorly with the severity of airways obstruction.[6-10] Some children may have very severe airways obstruction without appearing to be obviously distressed.
3. Investigations
3.1 Pulse oximetry
Oxygen saturation monitors should be available at all facilities that treat children with acute asthma. Low arterial oxygen saturation in room air (SpO2 <92%) after the initial bronchodilator therapy suggests a more severe group of patients and is an indication for admission.[6-8,10] All children with SpO2 <92% in room air after initial bronchodilator therapy must be admitted for inpatient treatment and monitoring.
3.2 Chest X-ray (CXR)
Routine CXRs are unnecessary. Indications for a CXR in acute asthma are:
- failure to respond to standard therapy
- subcutaneous emphysema or chest pain, suggesting an air leak or pneumothorax
- clinical signs suggesting lung collapse, consolidation or pneumothorax
- life-threatening asthma not responding to maximal therapy. A CXR may also be indicated to rule out alternative or concomitant diagnoses, especially in children not responding to treatment.
3.3 Arterial blood gas (ABG)
Indications for doing an ABG include severe or life-threatening asthma not responding to treatment. The PaCO2 is low in the early stages of acute asthma as a compensatory mechanism. A normal or raised PaCO2 indicates worsening asthma and respiratory failure.
4. Initial and first-line management of acute asthma
The initial treatment of an acute asthma attack consists of repeated doses of rapidly acting inhaled β2-agonists, systemic CS, and oxygen if hypoxic; all these therapies are supported by existing evidence as indicated in the text.
4.1 Oxygen
Children with life-threatening asthma, severe asthma or oxygen saturations less than 92% should receive oxygen via a high-flow face mask or nasal cannulas to maintain normal saturations (evidence A) and be admitted (evidence B). There is currently no consensus as to whether the oxygen should be humidified.[11,12] In hospitals, nebulisers should preferably be oxygen-driven.
4.2 Short-acting beta-2 (β2)-agonist bronchodilators
Short-acting inhaled β2-agonists are the mainstay of therapy for acute asthma, and the first-line treatment (evidence A). They stimulate β2 receptors on airway smooth muscle, resulting in smooth muscle relaxation.[13] However, receptors are also found in the heart, blood vessels, skeletal muscle, liver, pancreas and uterus, accounting for some of the side effects of β2-agonists including tachycardia, tremor, hypokalaemia and hyperglycaemia. The most commonly used agents in South Africa are salbutamol and fenoterol; salbutamol is the β2 agonist of choice in the majority of international acute asthma guidelines.[3,6]
Inhaled β2-agonists are preferably delivered by pressurised metered dose inhaler (pMDI) with a spacer (2 - 10 puffs, each inhaled separately with five tidal breaths at 15 - 30-second intervals) or by oxygen-driven nebuliser (evidence A).[14] A pMDI plus spacer is the preferred drug-delivery device for the treatment of mild to moderate acute asthma, while oxygen-driven nebulisers are preferred for severe or life-threatening acute asthma (evidence A). In young children (<3 years old), a spacer with a mask should be used; in older children, a pMDI and spacer with mouthpiece is preferable. Homemade spacers are as effective as commercial spacers in the treatment of acute asthma.[15,16] If using a pMDI and spacer with a mask, ensure that the mask fits closely onto the child's face.
Frequent doses of β2-agonists are safe for the treatment of acute asthma (evidence A). Two to four puffs repeated every 20 - 30 minutes depending on clinical response should be given for mild attacks; up to 10 puffs may be needed for more severe asthma. Bronchodilator therapy should be individualised depending on the severity of the acute asthma and the response to treatment. If hourly bronchodilators are required for more than 4 - 6 hours, the pMDI-spacer combination should be changed to a nebuliser.[6] Children who have not improved after receiving up to 10 puffs of β2-agonist should be referred to hospital. Children with severe or life-threatening asthma should receive nebulised β2-agonists (2.5 - 5 mg salbutamol or 0.5 - 1 mg fenoterol) and oxygen and should be transferred urgently to hospital. Nebulisation with β2-agonists can be repeated every 20 - 30 minutes or given continuously. The results of studies comparing intermittent and continuous nebulised short-acting β2-agonists are conflicting. A recent Cochrane review reported that continuous nebulised β2 agonists offered a small advantage over intermittent nebulisation in terms of hospital admission and lung function, with no increase in side-effects (evidence A).[17]

4.3 Steroid therapy
CS are standard first-line treatment for acute asthma, as they treat the underlying cause of asthma: inflammation (evidence A). They increase β2 receptor sensitivity by upregulating β2 expression on airway smooth muscle.[11,18] CS have been shown to decrease mortality, relapses, hospital admission and bronchodilator use. As systemic steroids require 6 - 24 hours to promote the anti-inflammatory response, early administration after presentation is necessary to reduce hospital admission.[12] The earlier they are administered in the acute attack, the better the outcome (evidence A).[19,20] Oral steroids are as effective as intravenous therapy, and preferable because of their ease of administration, cost-effectiveness and fewer side-effects. [21-23] The recommended dose of oral prednisone or prednisolone is 1 mg/kg/d, i.e. 20 mg in children aged 2 - 5 years and 30 - 40 mg in children aged >5 years.[24] Children on maintenance oral CS should receive 2 mg/kg/d up to a maximum dose of 60 mg.[6] A 3-day course is usually sufficient for children who are not hospitalised; however, if the asthma attack has not completely resolved then a longer course (7 - 14 days) may be needed.[6,25] It is unnecessary to taper the steroid dose unless it is used for longer than 14 days.[26,27] Intravenous steroids (which include hydrocortisone, methylprednisolone and dexamethasone), should be reserved for children with life-threatening asthma or those who cannot tolerate oral CS.

4.4 Ipratropium bromide
Ipratropium bromide (IB) is an anticholinergic agent that produces bronchodilatation within 20 - 30 minutes. Nebulised IB (250 µg/dose mixed with the nebulised β2-agonist solution) should be added if the child does not respond to three doses (nebulisation or multidosing via pMDI-spacer combination) of β2-agonists, or if the symptoms are severe (evidence A). Frequent doses of IB can be used every 20 - 30 minutes, together with β2-agonists, for the first 2 hours of a severe asthma attack[6] The dose frequency should be reduced to 4 - 6-hourly as clinical improvement occurs. Inhaled IB may be especially useful in patients who have been using high doses of β2-agonists before seeking medical care. IB alone is a less effective bronchodilator than a β2-agonist alone, but the combination of nebulised IB with a nebulised β2-agonist results in greater bronchodilatation than a β2-agonist on its own.[28,29]
Pre-mixed combination β2-agonist and anticholinergic inhalant solutions should be used with caution in children, as the concentrations of the individual drugs are higher than recommended for the paediatric population (Table 4).

5. Additional therapy for acute asthma
The following therapies may be considered in the management of acute severe asthma not responding to standard treatment.

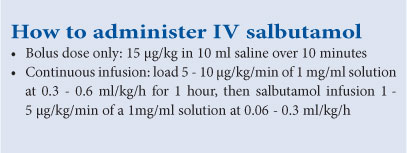
5.1 Intravenous low-dose bolus salbutamol
The use of IV low-dose salbutamol (15 pg/kg as a once-off bolus dose), added to standard therapy in the early management of acute severe asthma in children presenting to the emergency department (ED), may reduce the duration of the exacerbation and hasten the children's discharge from hospital (evidence B).[30,31] IV salbutamol alone is not better than inhaled β2-agonists.[32]
5.2 Intravenous salbutamol by continuous infusion
In the paediatric intensive care unit (PICU) a high IV loading dose of salbutamol (5 - 10 pg/kg/min of 1 mg/ml solution infused at 0.3 - 0.6 ml/kg/h for 1 hour) followed by continuous infusion (1 -5 pg/kg/min at 0.06 - 0.3 ml/kg/h) may be effective, and is probably safer than aminophylline. Continuous intravenous infusion should be considered when there is uncertainty about reliable inhalation of ß2-agonists or for severe refractory asthma. Electrolytes should be monitored regularly (evidence C).[6] Nebulised bronchodilator therapy should be continued while the patient is receiving IV salbutamol.[61
5.3 Intravenous aminophylline
Theophylline and its water-soluble salt, aminophylline, are methylxanthine derivatives that have largely fallen out of favour due to their narrow therapeutic index and potentially severe side-effects, such as cardiac arrhythmias or convulsions. Neither theophylline nor aminophylline is indicated in patients with mild to moderate acute asthma (evidence A), but may be used in cases of near-fatal or life-threatening asthma in the PICU (evidence C).[33-36] A 5 mg/kg loading dose should be given over 20 minutes under continuous ECG monitoring, followed by a continuous infusion at 0.5 - 1 mg/kg/h; the loading dose should be omitted in children receiving maintenance oral theophylline (evidence B).
5.4 Magnesium sulphate
Magnesium sulphate competes with calcium at smooth muscle binding sites, resulting in bronchodilation.[37] A single dose of intravenous magnesium sulphate 25 - 75 mg/kg (recommended dose 50 mg/kg, maximum dose 2 g) given over 20 minutes has been shown to be safe and effective in adults and children with acute severe asthma, who have had a poor response to initial therapy.[37,38] The response to magnesium appears to be best in patients who present with very severe illness (evidence C). [39-41]
The benefits associated with the use of nebulised magnesium sulphate remain controversial. Nebulised magnesium sulphate (0.4 ml 50% MgSO4 added to total volume of 4 ml nebuliser volume to achieve an isotonic solution) added to inhaled β2-agonists in the treatment of an acute asthma exacerbation has been shown to improve lung function in patients with severe asthma, with a trend towards fewer hospital admissions.[42]
5.5 Adrenaline
Intramuscular adrenaline is given for acute anaphylaxis (which may be confused with acute asthma) and angio-oedema, but it is not routinely indicated for acute asthma. Subcutaneously administered adrenaline may be used in patients who are moribund on presentation to the ED, or in an emergency situation where inhaled therapy is not available (evidence D).[43]
5.6 Inhaled steroids (ICS)
Insufficient evidence exists to recommend the use of ICS as alternative or additional therapy in acute asthma. Maintenance doses of ICS should be continued or started as soon as possible to form the basis of the chronic asthma management plan, and to allow the educational process regarding controller therapy to start even while the patient is hospitalised.[6,44-48]
5.7 Rapid-onset long-acting β2-agonists (formoterol)
Formoterol is a long-acting β2-agonist with a rapid onset of bronchodilation. Formoterol should never be used as monotherapy, as the use of long-acting β2-agonists is associated with increased risk of asthma mortality. Combination products containing formoterol and budesonide have been used as reliever medication for mild acute asthma symptoms in children older than 4 years (evidence B).49 However, there are currently insufficient data to make a recommendation regarding the use of formoterol as a reliever instead of short-acting β2-agonists in acute asthma.[50,51]
5.8 Leukotriene receptor antagonists
There is no evidence to support the use of leukotriene receptor antagonists for the treatment of acute asthma in children. In three trials comprising 194 children with acute asthma, there was no difference between oral leukotriene receptor antagonists (LTRA) and controls (evidence A).[52] One trial in 276 children compared intravenous LTRA to placebo and resulted in decreased hospital admission, but this was not statistically significant (evidence B).[52,53] Further research is required regarding the role of IV LTRA in acute asthma, but there is currently no IV LTRA that is registered in South Africa.
5.9 Antibiotics
Antibiotics are not routinely indicated in acute asthma, which is usually precipitated by a viral infection (evidence D).[54]
5.10 Heliox
Current evidence does not support the use of heliox in the initial treatment of acute asthma, but it may have a small role in acute asthma in children with severe obstruction, provided hypoxaemia is not severe. (evidence B).[55,56]
5.11 Intravenous fluids
Patients with prolonged severe asthma may become dehydrated as a result of poor intake or vomiting. It is, however, inadvisable to overhydrate patients with acute asthma as they are prone to transcapillary fluid migration and alveolar flooding.[57,58]
6. Indications for hospitalisation
The indications for hospitalisation are listed in Table 5.

7. Indications for PICU admission
The indications for PICU admission are listed in Table 6. Any child with acute severe asthma who is not responding to maximal inhaled therapy and systemic steroids, or who has features of life-threatening asthma not responding to initial therapy, should be admitted to the PICU.

7.1 Treatment of acute severe asthma in ICU
The detailed management of acute severe asthma in the ICU is beyond the scope of this guideline, but it includes continuous nebulised β2-agonists with oxygen, inhaled IB added to the salbutamol, systemic (IV) steroids and possibly either or both IV aminophylline and IV salbutamol.[55,60] Non-invasive ventilation is increasingly used for the management of respiratory failure in acute asthma, but requires the patient to be co-operative.[61-63] If intubation and mechanical ventilation are required, the currently preferred mode of ventilation is pressure control or pressure support ventilation, with slower rates allowing a sufficiently long expiratory time to permit emptying of the lungs.[63,64] Ketamine is recommended for sedation in intubated patients, and inhaled anaesthetic gases may be required in very severe cases not responding to maximal other therapy.[63]
8. Acute asthma in very young children
The assessment of acute asthma in children younger than 2 years can be very difficult, as objective measures of severity are not always reliable and other conditions, such as foreign body inhalation, gastro-oesophageal reflux with aspiration, lower respiratory tract infection, compression of the airways due to a congenital abnormality or tuberculous lymph nodes, and cystic fibrosis, may mimic asthma. Signs of severe acute asthma are: low oxygen saturation (SpO2 <92%), marked respiratory signs (using accessory muscles of respiration, marked retraction, tachypnoea) and inability to feed because of shortness of breath. Any one of these signs should place the child into the severe category. Apnoea, bradycardia or poor respiratory effort are features of life-threatening acute asthma.[6]
8.1 Treatment of acute asthma in children aged <2 years
Oxygen via close-fitting mask or nasal prongs must be administered to attain SpO2 >92%.
A trial of inhaled β2-agonist bronchodilator therapy should be instituted, in the same doses as for the older child. If there is a poor response to this treatment, the diagnosis of asthma should be reviewed. The optimal delivery system is a pMDI with spacer and mask for mild to moderate acute asthma, and oxygen-driven nebuliser for severe acute asthma (evidence A).[65-67] Oral β2-agonists are not recommended for the treatment of acute asthma in infants (evidence B).
Oral steroids, tablets or liquid (prednisone or prednisolone) should be given early in the management of severe acute asthma, and should be continued for up to three days (evidence B).[24,68-70]
If there is a poor response to inhaled β2-agonist therapy (after 3 treatments) or if the symptoms are more severe, add IB in the same dose as for older children (evidence B).[6,71]
9. Hospital discharge and follow-up[6]
A child can be discharged when:
- he/she is stable on 3 - 4-hourly inhaled bronchodilators that can be continued at home
- he/she is feeding well, is not tachypnoeic and no chest wall indrawing is present
- SpO2 >94% in room air
- PEFR and/or FEV1 should be >75% of best or predicted
- appropriate care can be provided at home.
Caregivers and children should receive asthma education with the emphasis placed on treatment and inhaler technique. Children should be discharged on appropriate maintenance therapy with a spacer, educated and with a written action plan to manage exacerbations. They should have a follow-up appointment with their primary care provider within a week of discharge. Patients with severe exacerbations or life-threatening asthma should preferably be referred to a clinic with a special interest in severe asthma and should be discharged on ICS controller therapy. Caregivers should be counselled regarding environmental triggers, especially for the child to avoid exposure to passive smoke or indoor air pollution.
Conflict of interest. S Kling: member of executive committee of the Allergy Society of South Africa; MSD speakers' bureau; instructor on Certificate of Asthma Care of National Asthma Education Programme. H Zar: president, South African Thoracic Society; president, Pan African Thoracic Society; Forum International Respiratory Societies; Global Advisory Committee Allergic Rhinitis and its Impact on Asthma (ARIA); World Allergy Organisation Special Committee on Paediatric Asthma. M Levin: member of executive committee of the Allergy Society of South Africa; instructor on Certificate of Asthma Care of National Asthma Education Programme; speaker at events sponsored by ThermoFisher, Pharma Dynamics, Nestlé, Cipla, Sanofi Aventis and Schering Plough; advisory board: Cipla; research support from ThermoFisher, ALLSA, GSK and Nestlé; advisor, Pharma Dynamics. R Green: chair, Allergy Society South Africa; executive member, South African Thoracic Society, National Asthma Education Programme; advisory board, Aspen, Cipla, MSD, Pfizer; speakers bureau: Abbott, Aspen, Cipla, MSD, Nycomed, Pfizer, Sanofi Aventis. P Jeena: chair of Paediatric Essential Drug Committee of South Africa; no conflict of interest. S Risenga: member of executive committee of the Allergy Society of South Africa; speaker for Nestlé and SAMA. S Thula, P Goussard, R Gie declare no conflicts of interest.
References
1. South African Childhood Asthma Working Group. Management of acute asthmatic attacks in children. S Afr Med J 1993;83:286-289. [ Links ]
2. Motala C, Green RJ, Manjra AI, Potter PC, Zar HJ, South African Childhood Asthma Working Group. Guideline for the chronic management of asthma in children - 2009 update. S Afr Med J 2009;99(12 Pt 2):898-912. [ Links ]
3. Global Initiative for Asthma. GINA Report: Global strategy for asthma management and prevention (2009 Update). http://www.ginasthma.com (accessed 24 February 2010). [ Links ]
4. Reddel HK, Taylor DR, Bateman ED, et al. An official American Thoracic Society / European Respiratory Society statement: Asthma control and exacerbations: Standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med 2009;180(1):59-99. [http://dx.doi.org/10.1164/rccm.200801-060ST] [ Links ]
5. Holley AD, Boots RJ. Review article: Management of acute severe and near-fatal asthma. Emerg Med Australas 2009;21(4):259-268. [http://dx.doi.org/10.1111/j.1742-6723.2009.01195.x] [ Links ]
6. British Thoracic Society/Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. May 2008; revised June 2009. http://www.sign.ac.za (accessed 23 January 2011). [ Links ]
7. Connett GJ, Lenney W. Use of pulse oximetry in the hospital management of acute asthma in childhood. Pediatr Pulmonol 1993;15(6):345-349. [http://dx.doi.org/10.1002/ppul.1950150606]
8. Geelhoed GC, Landau LI, Le Souëf PN. Evaluation of SaO2 as a predictor of outcome in 280 children presenting with acute asthma. Ann Emerg Med 1994;23(6):1236-1241. [http://dx.doi.org/10.1016/S0196-0644(94)70347-7] [ Links ]
9. Schuh S, Johnson D, Stephens D, et al. Hospitalization patterns in severe acute asthma in children. Pediatr Pulmonol 1997;23:184-192. [http://dx.doi.org/10.1002/(SICI)1099-0496(199703)23:3<184::AID-PPUL3>3.0.CC;2-C] [ Links ]
10. Wright RC, Santucci KA, Jay GD, Steele DW. Evaluation of pre- and posttreatment pulse oximetry in acute childhood asthma. Acad Emerg Med 1997;4(2):114-117. [http://dx.doi.org/10.1111/j.1553-2712.1997.tb03716.x] [ Links ]
11. Roy SR, Milgrom H. Management of the acute exacerbation of asthma. J Asthma 2003;40(6):593-603. [http://dx.doi.org/10.1081/JAS-120018776] [ Links ]
12. Richards G. Management strategies for acute and life threatening asthma. S Afr Respir J 2007;13:161-164. [ Links ]
13. Johnson M. Beta2-adrenoceptors: Mechanisms of action of beta2-agonists. Paediatr Resp Rev 2001;2(1):57-62. [http://dx.doi.org/10.1053/prrv.2000.0102] [ Links ]
14. Cates CJ, Crilly JA, Rowe BH. Holding chambers versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev 2006;3:CD000052. [http://dx.doi.org/10.1002/14651858.CD000052]
15. Zar HJ, Brown G, Donson H et al. Home-made spacers for bronchodilator therapy in children with acute asthma: A randomised trial. Lancet 1999;354(9183):979-982. [http://dx.doi.org/10.1016/S0140-6736(98)12445-5] [ Links ]
16. Rodriguez-Martinez CE, Sossa M, Lozano JM. Commercial versus home-made spacers in delivering bronchodilator therapy for acute therapy in children. Cochrane Database Syst Rev 2008;2:CD005536. [http://dx.doi.org/10.1002/14651858.CD005536] [ Links ]
17. Camargo Jr CA, Spooner C, Rowe BH. Continuous versus intermittent beta-agonists for acute asthma (Review). Cochrane Database Syst Rev 2003;4:CD001115. [http://dx.doi.org/10.1002/14651858.CD001115] [ Links ]
18. Roy SR, Milgrom H. Managing outpatient asthma exacerbations. Curr Allergy Asthma Rep 2010;10(1):56-66. [http://dx.doi.org/10.1007/s11882-009-0083-5] [ Links ]
19. Streetman DD, Bhatt-Mehta V, Johnson CE. Management of acute severe asthma in children. Ann Pharmacother 2002;36(7-8):1249-1260. [http://dx.doi.org/10.1345/aph.1A189] [ Links ]
20. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev 2001;1:CD002178. [http://dx.doi.org/10.1002/14651858.CD002178] [ Links ]
21. Manser R, Reid D, Abramson M. Corticosteroids for acute severe asthma in hospitalised patients. 2001;1:CD001740. [http://dx.doi.org/10.1002/14651858.CD001740] [ Links ]
22. Becker JM, Arora A, Scarfone RJ, et al. Cral versus intravenous corticosteroids in children hospitalized with asthma. J Allergy Clin Immunol 1999;103(4):586-590. [http://dx.doi.org/10.1016/S0091-6749(99)70228-9] [ Links ]
23. Barnett PL, Caputo GL, Baskin M, Kuppermann N. Intravenous versus oral corticosteroids in the management of acute asthma in children. Ann Emerg Med 1997;29(2):212-217. [http://dx.doi.org/10.1016/S0196-0644(97)70270-1] [ Links ]
24. Langton HS, Hobbs J, Reid F, Lenney W. Prednisolone in acute childhood asthma: Clinical response to three dosages. Respir Med 1998;92(3):541-546. [ Links ]
25. Chang AB, Clark R, Sloots TP, et al. A 5- versus 3-day course of oral corticosteroids for children with asthma exacerbations who are not hospitalised: A randomised controlled trial. Med J Aust 2008;189(6):306-310. [ Links ]
26. Hatton MQ, Vathenen AS, Allen MJ, Davies S, Cooke NJ. A comparison of 'abruptly stopping' with 'tailing off' oral corticosteroids in acute asthma. Respir Med 1995;89(2):101-104. [http://dx.doi.org/10.1016/0954-6111(95)90191-4Links ] Arial, Helvetica, sans-serif" size="2">]
27. C'Driscoll BR, Kalra S, Wilson M, Pickering CA, Carroll KB, Woodcock AA. Double-blind trial of steroid tapering in acute asthma. Lancet 1993;341(8841):324-327. [http://dx.doi.org/10.1016/0140-6736(93)90134-3]
28. Teoh L, Cates CJ, Hurwitz M, Acworth JP, van Asperen P, Chang AB. Anticholinergic therapy for acute asthma in children. Cochrane Database Syst Rev 2012;4:CD003797. [http://dx.doi.org/10.1002/14651858.CD003797.pub2] [ Links ]
29. Plotnick LH, Ducharme FM. Acute asthma in children and adolescents: Should inhaled anticholinergics be added to beta(2)-agonists? Am J Respir Med 2003;2(2):109-115. [ Links ]
30. Browne GJ, Penna AS, Phung X, Soo M. Randomised trial of intravenous salbutamol in early management of acute severe asthma ins children. The Lancet 1997;349(9048):301-305. [http://dx.doi.org/10.1016/S0140-6736(96)06358-1] [ Links ]
31. Browne GJ, Lam LT. Single-dose intravenous salbutamol bolus for managing children with acute severe asthma in the emergency department: Reanalysis of data. Pediatr Crit Care Med 2002;3(2):117-123. [http://dx.doi.org/10.1097/00130478-200204000-00005] [ Links ]
32. Travers AA, Jones AP, Kelly KD, Camargo CAJ, Barker SJ, Rowe BH. Intravenous beta2-agonists for acute asthma in the emergency department. Cochrane Database Syst Rev 2001;1:CD002988. [http://dx.doi.org/10.1002/14651858.CD002988] [ Links ]
33. Parameswaran K, Belda J, Rowe BH. Addition of intravenous aminophylline to beta2-agonists in adults with acute asthma. Cochrane Database Syst Rev 2000;4:CD002742. [http://dx.doi.org/10.1002/14651858.CD002742] [ Links ]
34. Goodman DC, Littenberg B, O'Connor GT, Brooks JG. Theophylline in acute childhood asthma: A meta-analysis of its efficacy. Pediatr Pulmonol 1996;21(4):211-218. [http://dx.doi.org/10.1002/(SICI)1099-0496(199604)21:4<211::AID-PPUL2>3.0.CO;2-R] [ Links ]
35. Roberts G, Newsom D, Gomez K, et al. Intravenous salbutamol bolus compared with an aminophylline infusion in children with severe asthma: A randomised controlled trial. Thorax 2003;58(4):306-310. [http://dx.doi.org/10.1136/thorax.58.4.306] [ Links ]
36. Mitra AAD, Bassler D, Watts K, Lasserson TJ, Ducharme FM. Intravenous aminophylline for acute severe asthma in children over two years receiving inhaled bronchodilators. Cochrane Database Syst Rev 2005;2:CD001276. [http://dx.doi.org/10.1002/14651858.CD001276.pub2]
37. Carroll W, Lenney W. Drug therapy in the management of acute asthma. Arch Dis Child - Education and practice edition. 2007;92(3),ep82-86. [http://dx.doi.org/10.1136/adc.2006.107631] [ Links ]
38. Ciarallo L, Brousseau D, Reinert S. Higher-dose magnesium therapy for children with moderate to severe acute asthma. Arch Pediatr Adolesc Med 2000;154(10):979-983. [http://dx.doi.org/10.1001/archpedi.154.10.979] [ Links ]
39. Rowe BH, Bretzlaff JA, Bourdon C, Bota GW, Blitz S, Camargo CA. Magnesium sulfate for treating exacerbations of acute asthma in the emergency department. Cochrane Database Syst Rev 2000;1:CD0011490. [http://dx.doi.org/10.1002/14651858.CD001490]
40. Cheuk DK, Chau TC, Lee SL. A meta-analysis on intravenous magnesium sulphate for treating acute asthma. Arch Dis Child 2005;90(1):74-77. [http://dx.doi.org/10.1136/adc.2004.050005] [ Links ]
41. Rowe BH, Camargo CA Jr. The role of magnesium sulfate in the acute and chronic management of asthma. Curr Opin Pulm Med 2008;14(1):70-76. [http://dx.doi.org/10.1097/MCP.0b013e3282f19867] [ Links ]
42. Blitz M, Blitz S, Beasely R, et al. Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Database Syst Rev 2005,4:CD003898. [http://dx.doi.org/10.1002/14651858.CD003898.pub4] [ Links ]
43. Papiris SA, Manali ED, Kolilekas L, Triantafillidou C, Tsangaris I. Acute severe asthma. New approaches to assessment and treatment. Drugs 2009;69(17):2363-2391. [http://dx.doi.org/10.2165/11319930-000000000-00000] [ Links ]
44. Edmonds ML, Milan SJ, Brenner BE, Camargo CA, Rowe BH. Inhaled steroids for acute asthma following emergency department discharge. Cochrane Database Syst Rev 2012;12:CD002316. [http://dx.doi.org/10.1002/14651858.CD002316.pub2] [ Links ]
45. Edmonds ML, Camargo CA, Pollack CV, Rowe BH. Early use of inhaled corticosteroids in the emergency department treatment of acute asthma. Cochrane Database Syst Rev 2003;3:CD002308.[http://dx.doi.org/10.1002/14651858.CD002308.pub2] [ Links ]
46. McKean M, Ducharme F. Inhaled steroids for episodic viral wheeze of childhood. Cochrane Database Syst Rev 2000;1:CD001107. [http://dx.doi.org/10.1002/14651858.CD001107] [ Links ]
47. Schuh S, Reisman J, Alshehri M, et al. A comparison of inhaled fluticasone and oral prednisone for children with severe acute asthma. N Engl J Med 2000;343(10):689-694. [http://dx.doi.org/10.1056/NEJM200009073431003] [ Links ]
48. Volovitz B. Inhaled budesonide in the management of acute worsening and exacerbations of asthma: A review of the evidence. Respir Med 2007;101:685-695. [http://dx.doi.org/10.1016/j.rmed.2006.10.009] [ Links ]
49. Welsh EJ, Cates CJ. Formoterol versus short-acting beta-agonists as relief medication for adults and children with asthma. Cochrane Database Syst Rev 2010;9:CD008418. [http://dx.doi.org/10.1002/14651858.CD008418.pub2] [ Links ]
50. O'Byrne PM, Bisgaard H, Godard PP, et al. Budesonide/formoterol combination therapy as both maintenance and reliever medication in asthma. Am J Respir Crit Care Med 2005;171(2):129-136. [http://dx.doi.org/10.1164/rccm.200407-884OC] [ Links ]
51. Bisgaard H, Le Roux P, Bjámer D, Dymek A, Vermeulen JH, Hultquist C. Budesonide/formoterol maintenance plus reliever therapy: A new strategy in pediatric asthma. Chest 2006;130(6):1733-1743. [http://dx.doi.org/10.1378/chest.130.6.1733] [ Links ]
52. Watts K, Chavasse RJPG. Leukotriene receptor antagonists in addition to usual care for acute asthma in adults and children. Cochrane Database Syst Rev 2012;5:CD006100. [http://dx.doi.org/10.1002/14651858.CD006100.pub2] [ Links ]
53. Morris CR, Becker AB, Piñieiro A, et al. A randomized, placebo-controlled study of intravenous montelukast in children with acute asthma. Ann Allergy Asthma Immunol 2010;104(2):161-171. [http://dx.doi.org/10.1016/j.anai.2009.11.065] [ Links ]
54. Graham V, Lasserson TJ, Rowe BH. Antibiotics for acute asthma. Cochrane Database Syst Rev 2001;2:CD002741. [http://dx.doi.org/10.1002/14651858.CD002741] [ Links ]
55. Rodrigo GJ, Pollack CV, Rodrigo C, Rowe BH. Heliox for non-intubated acute asthma patients. Cochrane Database Syst Rev 2006;4:CD002884. [http://dx.doi.org/10.1002/14651858.CD002884.pub2] [ Links ]
56. Bigham MT, Jacobs BR, Monaco MA, et al. Helium/oxygen-driven albuterol nebulization in the management of children with status asthmaticus: A randomized, placebo-controlled trial. Pediatr Crit Care Med 2010;11(3):356-361. [http://dx.doi.org/10.1097/PCC.0b013e3181c5163f] [ Links ]
57. Bigham MT, Brilli RJ. Status asthmaticus. In: Nichols DG, ed. Rogers' Textbook of Pediatric Intensive Care. 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2008. [ Links ]
58. Rotta AT. Asthma. In: Fuhrman BP, Zimmerman J, eds. Pediatric Critical Care. 3rd ed. Philadelphia: Mosby, 2006. [ Links ]
59. Bohn D, Kissoon N. Acute asthma. Pediatr Crit Care Med 2001;2(2):151-163. [http://dx.doi.org/10.1097/00130478-200104000-00010] [ Links ]
60. Mannix R, Bachur R. Status asthmaticus in children. Curr Opin Pediatr 2007;19(3):281-287. [http://dx.doi.org/10.1097/MOP.0b013e3280f77531] [ Links ]
61. Thill PJ, Mguire JK, Baden HP, Green TP. Noninvasive positive-pressure ventilation in children with lower airway obstruction. Pediatr Crit Care Med 2004;5(4):337-342. [http://dx.doi.org/10.1097/01.PCC.0000128670.36435.83] [ Links ]
62. Carroll CL, Schramm CM. Noninvasive positive pressure ventilation for the treatment of status asthmaticus in children. Ann Allergy Asthma Immunol 2006;96(3):454-459. [http://dx.doi.org/10.1016/S1081-1206(10)60913-1] [ Links ]
63. Kissoon N. The child with asthma - emergency and critical care issues. Curr Allergy Clin Immunol 2007;20(3):116-122. [ Links ]
64. Sarnaik AP, Daphtery KM, Meert KL, Lieh-Lai MW, Heidemann SM. Pressure controlled ventilation in children with severe status asthmaticus. Pediatr Crit Care Med 2004;5(2):133-138. [http://dx.doi.org/10.1097/01.PCC.0000112374.68746.E8] [ Links ]
65. Closa RM, Ceballos JM, Gómez-Papí A, Galiana AS, Gutiérrez C, Martí-Henneber C. Efficacy of bronchodilators administered by nebulizers versus spacer devices in infants with acute wheezing. Pediatr Pulmonol 1998;26(5):344-348. [http://dx.doi.org/10.1002/(SICI)1099-0496(199811)26:5<344::AID-PPUL7>3.0.CO;2-F] [ Links ]
66. Wildhaber JH, Devadason SG, Hayden MJ, Eber E, Summers QA, LeSouéf PN. Aerosol delivery to wheezy infants: A comparison between a nebulizer and two small volume spacers. Pediatr Pulmonol 1997;23(3):212-216. [http://dx.doi.org/10.1002/(SICI)1099-0496(199703)23:3<212::AID-PPUL7>3.0.CO;2-P] [ Links ]
67. Rubilar L, Castro-Rodriguez JA, Girardi G. Randomized trial of salbutamol via metered-dose inhaler with spacer versus nebulizer for acute wheezing in children less than 2 years of age. Pediatr Pulmonol 2000;29(4):264-269. [http://dx.doi.org/10.1002/(SICI)1099-0496(200004)29:4<264::AID-PPUL5>3.0.CO;2-S] [ Links ]
68. Tal A, Levy N, Bearman JE. Methylprednisolone therapy for acute asthma in infants and toddlers: a controlled clinical trial. Pediatrics 1990;86(3):350-356. [ Links ]
69. Fox GF, Marsh MJ, Milner AD. Treatment of recurrent acute wheezing episodes in infancy with oral salbutamol and prednisolone. Eur J Pediatr 1996;155(6):512-516. [http://dx.doi.org/10.1007/BF01955192Links ] Arial, Helvetica, sans-serif" size="2">]
70. Daugbjerg P, Brenoe E, Forchhammer H, et al. A comparison between nebulized terbutaline, nebulized corticosteroid and systemic corticosteroid for acute wheezing in children up to 18 months of age. Acta Paediatrica 1993;82(6-7):547-551. [http://dx.doi.org/10.1111/j.1651-2227.1993.tb12750.x] [ Links ]
71. Everard ML, Bara A, Kurian M, Elliott TM, Ducharme F, Mayowe V. Anticholinergic drugs for wheeze in children under the age of two years. Cochrane Database Syst Rev 2005;3:CD001279. [http://dx.doi.org/10.1002/14651858.CD001279.pub2] [ Links ]
 Corresponding author:
Corresponding author:
S Kling (sk@sun.ac.za)



{kind=link}