










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309Print version ISSN 1681-150X
SA orthop. j. vol.21 n.2 Centurion 2022
https://doi.org/10.17159/2309-8309/2022/v21n2a7
KNEE
Mega-OATS of the knee without specialised instrumentation: a low-cost option for large cartilage defects in a resource-restrained environment
Johan le RouxI; Richard von BormannII; Sepp BraunIII; Andreas Β ImhoffIV; Michael HeldI, *
IDepartment of Surgery, Division of Orthopaedic Surgery, University of Cape Town, Groote Schuur Hospital, Cape Town, South Africa
IINetcare Christiaan Barnard Hospital, Cape Town, South Africa
IIIGelenkpunkt UMIT, Research Unit for Orthopedic Sports Medicine and Injury Prevention, Innsbruck, Austria
IVDepartment of Orthopaedic Sports Medicine, Technical University of Munich, Munich, Germany
ABSTRACT
BACKGROUND: A 26-year-old patient presented to a specialised knee clinic in a public hospital with ongoing pain after having sustained a soccer injury six years prior. A large osteochondral defect of the distal medial femoral condyle was diagnosed. Due to resource limitations, fresh allograft or a large osteochondral autograft transplantation system (Mega-OATS) workbench was unavailable.
CASE REPORT: A Mega-OATS cartilage transplantation was done, using the patient's posteromedial femoral condyle as donor tissue, and transplanted to the defect in the distal femoral condyle, a technique that has been well documented and followed up. At six weeks postoperatively, an MRI showed early incorporation of the graft tissue. Clinical outcomes were excellent at one year follow-up with the EQ-5D 5L score 11111, the Knee Injury and Osteoarthritis Outcome Score (KOOS-PS) 100%, and the Lysholm score also 100%. Radiographs at one year confirmed an unchanged graft position and showed no signs of osteoarthritis.
DISCUSSION: Large osteochondral lesions in the knee (> 4 cm2) are challenging to treat, and the most commonly used modalities are fresh osteochondral allograft (OCA) or autologous chondrocyte implantation (ACI). Mega-OATS of the knee has previously been described but is not commonly used due to the requirement of a specialised and expensive workbench, and fear of morbidity at the donor site.
CONCLUSION: Mega-OATS of the knee is possible without a specialised workbench or tools and had good clinical outcomes at two-year follow-up of the patient.
Level of evidence: Level 5
Keywords: Mega-OATS, osteochondral lesion knee, osteochondral autograft, resource restraint
Introduction
Osteochondral lesions present a challenge in young patients when arthroplasty is not considered a reasonable treatment option.1 Most joint-preserving treatment modalities for large cartilage defects are associated with considerable cost and often require intricate supply chains, subspecialist surgical skill sets, and an advanced theatre setup. Therefore, complex cartilage surgery is often not feasible with limited resources.2 The use of autologous chondrocyte implantation (ACI) is limited due to the high cost, and osteochondral allograft (OCA) depends on a reliable tissue bank that can guarantee good quality and infection-free fresh allograft.
These techniques are therefore unavailable in a limited-resource environment.3 An option that is available is a large osteochondral autograft transplantation system (Mega-OATS) where an ipsilateral posterior femoral condyle is harvested and transplanted. It must be highlighted that this is a salvage procedure and should not be used as a first-line option for all cases. This technique has been well described and excellent outcomes have been shown up to 5.5 years postoperatively.4-7 Mega-OATS relies on autograft, and therefore does not require access to chondrocyte culture or a tissue bank. However, in the described techniques, an expensive workstation to handle and shape the autograft is needed. The novelty and objective of our case report is the description of the Mega-OATS procedure with non-specialised instrumentation suitable for a limited-resource setup.
Case report
History and clinical findings
A 26-year-old healthy male presented to a subspecialist knee clinic of a large sub-Saharan academic hospital complaining of medial-sided left knee pain after a sports injury six years prior. The patient walked with an antalgic limp, had an effusion, and limited active range of motion of 0-90° and a passive range of motion (PROM) of 0-130°. No pathology was noted regarding menisci and ligaments.
Diagnostic studies and workup
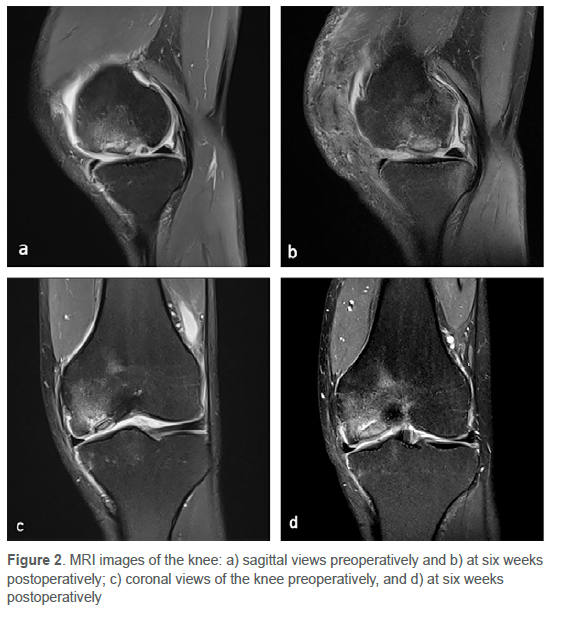
Radiographs revealed a large osteochondral lesion in the distal medial condyle (Figure 1). Magnetic resonance imaging (MRI) demonstrated a high-grade 1.4 χ 2.5 cm chondral lesion in the weight-bearing area, with loose intra-articular fragments (Figure 2). The posterior condyles were unaffected and no secondary osteoarthritis was noted with intact menisci and ligaments. The mechanical axis was neutral on long limb views.

Planning of procedure
Due to graft handling challenges, a specialised Mega-OATS workstation has been developed which can be purchased directly from Arthrex™ (Naples, FL) for R531 065 ($38 085). No loan sets are available in South Africa which therefore prevents local surgeons to follow the published techniques. After detailed discussion with international experts and the patient, it was decided to perform the Mega-OATS using only store-bought equipment to the value of R112 or $8. To allow for various defect sizes, a 20 mm, 25 mm and 30 mm flat drill bit with corresponding washers for templating were bought.
Surgical treatment
We followed the previously described Mega-OATS technique, but without using the workstation.6,7 A midline longitudinal incision with a medial parapatellar approach was used, and the defect confirmed clinically (Figure 3). The posteromedial femoral condyle was harvested with an osteotome in line with the posterior femoral cortex.

Hohman retractors were used to protect the medial collateral ligament and posterior cruciate ligament. The most dorsal cortex was carefully separated to avoid vascular damage. The osteochondral lesion measured 20 χ 30 mm in size, and a 25 mm flat stainless steel drill bit obtained from the local hardware shop was used to overdrill the osteochondral defect into a round shape and to a depth of 10 mm (Figure 4). A marker pen was used to draw a circle with a 25 mm diameter onto the graft. A Kirschner wire drilled through the graft from side to side and bent on both ends was used to handle the slippery graft without a specialised workstation. A rongeur was used to shape the autograft for press-fit grafting (Figure 4). No additional hardware was necessary. After infiltration with local anaesthetic, the wound was closed with multiple layers of absorbable sutures. The surgical time for the procedure was 1 hour 37 minutes.
The patient was discharged one day after the operation. Postoperative rehabilitation consisted of non-weight-bearing for six weeks, after which closed chain exercises were started. Weight-bearing was started after confirming early integration of the graft with MRI scan six weeks after the procedure (Figure 2).
Already at the six-month follow-up, the patient showed marked improvement of pain and function, reporting of only mild start-up pain after sitting for a prolonged time. At two-year follow-up the patient reported no pain in the left knee, and good stair climbing or squatting without pain. The range of motion in the left knee was 0-130°, with no laxity or instability in the coronal or sagittal plane (Figure 5). The EQ-5D 5L score was 11111, the Knee Injury and Osteoarthritis Outcome Score (KOOS-PS) 100%, and the Lysholm score also 100%. Radiographs at one year confirmed an unchanged graft position and showed no signs of osteoarthritis (Figure 1).

Discussion
Cartilage defects are a common cause of painful knees and are most frequent in the medial femoral condyle in the young male patient.8,9 Treatment options depend on the size of the defect. In lesions less than 2 cm2, microfracture and OATS are recommended. With microfracture, treatment failure can be expected after five years postoperatively, whereas OATS has shown better intermediate and long-term outcomes.10,11 In intermediate size lesions between 2 and 4 cm2 OATS, microfracture and ACI (autologous chondrocyte implantation) is commonly performed, and in large lesions > 4 cm2 treatment options are ACI and OCA (osteochondral allograft).1,3,12
Gudas et al. showed that the patient-reported outcome measures (PROMs) after treatment for larger sized cartilage lesions with a mean of 2.8 cm2 is similar when comparing microfracture to OATS at ten years postoperatively. However, 75% of patients returned to their pre-injury level of activity after OATS compared to only 37% after microfracture. Younger patients (< 25 years) showed significantly better PROMs with OATS than older patients and remained higher at ten years after the procedure.13 In a randomised control trial, Knutsen et al. noted that patients older than 30 years of age had worse outcomes than younger patients who were treated with microfracture and OATS. There was no difference between the two treatment modalities at five years postoperatively.14
Although OATS does achieve restoration of organised hyaline cartilage, the limited amount of expendable donor cartilage limits this option to smaller lesions. For large lesions, Imhoff et al. presented a Mega-OATS case series using the posterior femoral condyle as autograft.6 A concern with this technique may be that of morbidity at the donor site; however, the defect of the donor site had no clinical impact in follow-up and, in some cases, was found to be replaced by white fibrous tissue.6 Although we had excellent results in one case, this should not be generalised and a larger series is needed to evaluate the outcomes when using the low-cost tools. Promising results have been described in a 5.5-year follow-up of 33 patients using a Mega-OATS workstation which showed a highly significant median increase in the Lysholm score from 49.0 preoperatively to 86.0 points.6 Twenty-seven patients returned to recreational sports, and X-rays showed partial remodelling of the posterior condyle in 24 patients.
Like Imhoff et al., we also noted marked improvement and no major deficit in knee function of the patient due to the harvest of the posterior condyle. Imhoff used specialised equipment, such as a recipient and donor harvester, dilators, tamps and a workbench. However, the need for this instrumentation, and the complex surgical technique is known as a barrier to the use of Mega-OATS.2 Although OATS is frequently performed at our institution, the size of the defect in this patient required a Mega-OATS. As previously mentioned, the loan sets are not available in our country and a purchase price of $38 095 (R531 065) prevented its use. We, therefore, acquired a set of stainless-steel flat drill bits from 20 mm to 30 mm in 5 mm increments, priced at a total of $8 (R112) (Figure 6).

The most important limitation of this technique remains the possible morbidity at the donor site, despite previously, and in this case, being reported as minimal to none.6 We therefore do not advise this technique as a standard treatment option, but rather as one that should be approached with caution by an experienced knee surgeon in a very select patient combined with a resource-limited environment, as highlighted above.
The main advantage of using the described low-cost technique is that the instrumentation is freely available and very cost-effective. Yet, there are important problems and pitfalls to take into consideration when considering this option. The main technical disadvantage of this technique was the difficulty of handling the slippery osteochondral autograft and preventing it from falling on the floor. The Mega-OATS workbench has six holding screws that tighten around the graft, securing it in place. We solved the problem by drilling a K-wire through the graft from side to side, not damaging the chondral surface, and using it as handles. The precision of the graft shaping is also limited without a core reamer, but only a rongeur. This can be overcome by using circular templates (i.e., a 20 mm washer bought at the local hardware store). Also, no jig was available to ensure perpendicular orientation of the reamer to the cartilage level. We used a store-bought 25 mm flat drill bit for this. There was also no depth gauge available to confirm depth of the donor site. Here we used a ruler at 12, 3, 6, and 9 o'clock and correlated this with the graft thickness. Also, careful placement of the reamer and frequent checks while reaming are of paramount importance. Another technical consideration must be that a fixation system for the graft (i.e., headless screws) should be available in case press-fit fixation fails.
It is a potential medico-legal challenge to use equipment not designed for clinical use. This needs to be highlighted to the patient, hospital and theatre staff beforehand and written consent for it must be obtained.
A limitation of the study is the short radiological follow-up of six weeks (MRI) and one year (X-rays). Although we can report that the procedure is safe and carries no objective morbidity within two years postoperatively, longer follow-up will need to be done to screen for the development of osteoarthritis and other complications.
Conclusion
The Mega-OATS was successfully performed in this patient with a new low-cost technique, without complications and excellent outcome. It could therefore be used as a safe salvage procedure and may be a viable low-cost alternative for young patients with large osteochondral defects in the knee.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. Prior to commencement of the study, ethics approval was obtained from the University of Cape Town Human Research Ethics Committee No. 144/3030. Informed consent was obtained from the patient.
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
JlR: data analysis, first draft preparation, manuscript preparation, manuscript revision, submission, primary author
RvB: study conceptualisation, manuscript revision
SB: study conceptualisation, manuscript revision
ABI: study conceptualisation, manuscript revision
MH: study conceptualisation, data capture, first draft preparation, manuscript revision, study design
ORCID
Le Roux J https://orcld.org/0000-0002-5658-6827
Von Bormann R https://orcld.org/0000-0002-4546-3143
Braun S https://orcld.org/0000-0002-8865-2606
Imhoff AB https://orcld.org/0000-0001-5085-6446
Held Μ https://orcld.org/0000-0002-0671-0439
References
1. Karataglis D, Learmonth DJA. Management of big osteochondral defects of the knee using osteochondral allografts with the MEGA-OATS technique. Knee. 2005;12(5):389-93. https://doi.org/10.1016/j.knee.2004.12.008. [ Links ]
2. Bugbee WD, Pallante-Kichura AL, Görtz S, Amiel D, Sah R. Osteochondral allograft transplantation in cartilage repair: Graft storage paradigm, translational models, and clinical applications. J Orthop Res. 2016;34(1):31-38. https://doi.org/10.1002/jor.22998. [ Links ]
3. Richter DL, Schenck RC, Wascher DC, Treme G. Knee articular cartilage repair and restoration techniques: a review of the literature. Sports Health. 2016;8(2):153-60. https://doi.org/10.1177/1941738115611350. [ Links ]
4. Braun S, Minzlaff P, Hollweck R, Wörtler K, Imhoff AB. The 5.5-year results of Mega-OATS -autologous transfer of the posterior femoral condyle: A case-series study. Arthritis Res Ther. 2008;10(3):1-14. https://doi.org/10.1186/ar2439. [ Links ]
5. Minzlaff P, Braun S, Haller B, Wõrtler K, Imhoff AB. Der autologe Transfer der posterioren Femurkondyle bei ausgedehnten osteochondralen Schãden des Knies : 5-Jahres-Ergebnisse der Mega-OATS-Technik. Orthopade. 2010;39(6):631-36. https://doi.org/10.1007/s00132-010-1608-2. [ Links ]
6. Agneskirchner JD, Brucker P, Burkart A, Imhoff AB. Large osteochondral defects of the femoral condyle: Press-fit transplantation of the posterior femoral condyle (MEGA-OATS). Knee Surg Sport Traumatol Arthrosc. 2002;10(3):160-68. https://doi.org/10.1007/s00167-001-0259-6. [ Links ]
7. Brucker PU, Paul J, Imhoff AB. Mega-OATS technik und ergebnisse. Unfallchirurg. 2002;105(5):443-49. https://doi.org/10.1016/B978-1-4377-0878-3.10009-9. [ Links ]
8. Hjelle K, Solheim E, Strand T, Muri R, Brittberg M. Articular cartilage defects in 1,000 knee arthroscopies. Arthroscopy. 2002;18(7):730-34. https://doi.org/10.10534ars.2002.32839. [ Links ]
9. Pareek A, Sanders TL, Wu IT, Larson DR, Saris DBF, Krych AJ. Incidence of symptomatic osteochondritis dissecans lesions of the knee: a population-based study in Olmsted County. Osteoarthr Cartil. 2017;25(10):1663-71. https://doi.org/10.1016/jjoca.2017.07.005. [ Links ]
10. Hangody L, Füles P. Autologous osteochondral mosaicplasty for the treatment of full-thickness defects of weight-bearingjoints: Ten years of experimental and clinical experience. J Bone Joint Surg. 2003;85(SUPPL 2):25-32. https://doi.org/10.2106/00004623-200300002-00004. [ Links ]
11. Goyal D, Keyhani S, Lee EH, Hui JHP. Evidence-based status of microfracture technique: A systematic review of Level I and II studies. Arthroscopy. 2013;29(9):1579-88. https://doi.org/10.1016/j.arthro.2013.05.027. [ Links ]
12. Hohmann E, Tetsworth K. Large osteochondral lesions of the femoral condyles: Treatment with fresh frozen and irradiated allograft using the Mega OATS technique. Knee. 2016;23(3):436-41. https://doi.org/10.1016/j.knee.2016.01.020. [ Links ]
13. Gudas R, Gudaite A, Pocius A, et al. Ten-year follow-up of a prospective, randomized clinical study of mosaic osteochondral autologous transplantation versus microfracture for the treatment of osteochondral defects in the knee joint of athletes. Am J Sports Med. 2012;40(11):2499-508. https://doi.org/10.1177/0363546512458763. [ Links ]
14. Knutsen G, Drogset JO, Engebretsen L, et al. A randomized trial comparing autologous chondrocyte implantation with microfracture: Findings at five years. J Bone Joint Surg. 2007;89(10):2105-12. https://doi.org/10.2106/JBJS.G00003. [ Links ]
Received: August 2020
Accepted: July 2021
Published: May 2022
* Corresponding author: email.held@gmail.com
Editor: Dr Chris Snyckers, Eugene Marais Hospital, Pretoria, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.

{kind=link}