










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.77 n.2 Johannesburg Mar. 2022
https://doi.org/10.17159/2519-0105/2022/v77no2a10
RADIOLOGY CASE
Z YakoobI; C SmitII
IBChD, PDD (Maxillofacial and Oral Radiology), MSc (Maxillofacial and Oral Radiology). Department of Oral Pathology and Oral Biology, Faculty of Health Sciences, University of Pretoria. ORCID: 0000-0003-1966- 5574
IIBChD, MSc (Maxillofacial and Oral Radiology). Department of Oral Pathology and Oral Biology, Faculty of Health Sciences, University of Pretoria. ORCID: 0000-0003-4047-6356
CBCT INCIDENTAL FINDINGS
CASE
Below are two patients that presented to our facility for dental treatment. In both of these patients' calcifications were noted as incidental findings.
INTERPRETATION
Large field of view cone beam computed tomography (CBCT) images allows the visualisation of anatomical structures outside of the teeth and jaws. These areas include the cranial vault and paranasal sinuses. Occasionally pathology, anatomical variation and various other incidental findings can be seen.1 As the use of CBCT has become more common amongst general dentists and specialists, awareness and understanding of incidental findings are of great importance, for the patient as well as medico-legal reasons. Calcifications that are found as incidental findings on CBCT scans within the brain can be pathological or physiological in origin. Common areas within the brain where physiological calcifications can be found include the pineal gland, choroid plexus, habenular, tentorium cerebelli, sagittal sinus, and falx cerebri. The most reported form of physiological brain calcifications is in the pineal gland and is thought to be an age-related change.2 Pathological calcifications are less common than the physiological variants and are because of more serious diseases such as infectious diseases, endocrine disorders, metastatic lesions, and primary intracranial tumours, to name a few.3
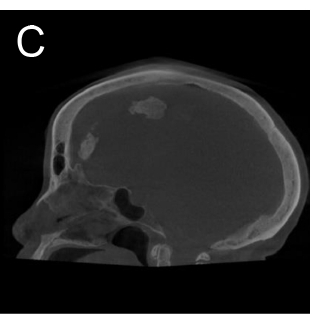
Above are images of two patients that presented to our facility for reasons unrelated to the calcifications. The first patient is a 72-year-old female (Images A-C) that presents with physiological calcifications of the falx cerebri. The second patient is an 82-year-old female that presents with physiological calcifications of the choroid plexus glomus (Image D), unilateral globus pallidus calcifications (Image E) and pineal gland calcifications (Image F).





Although neither of these patients required medical intervention, a thorough medical history should always be undertaken together with a detailed evaluation of the full CBCT volume, to eliminate possible pathological calcifications.
Dentists and dental specialists should be mindful of incidental findings that may be found on CBCT scans. In cases of uncertainty a dentist trained in maxillofacial radiology and pathology should be consulted as negligence of this nature can result in medico-legal implications.
AUTHORS DECLARATION
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Conflict of Interest: The authors declare that they have no conflict of interest.
Ethics approval: This study was approved by the University of Pretoria, Faculty of Health Sciences Research Ethics Committee (Reference no.: 478/2021). All procedures followed the ethical standards of the Helsinki Declaration of 1975, as revised in 2008.
REFERENCES
1. Ozdede M, Kayadugun A, Ucok O, Altunkaynak B, Peker I. The assessment of maxillofacial soft tissue and intracranial calcifications via cone-beam computed tomography. Current Medical Imaging. 2018 Oct 1;14 (5):798-806. [ Links ]
2. Khalifa HM, Felemban OM. Nature and clinical significance of incidental findings in maxillofacial cone-beam computed tomography: a systematic review. Oral Radiology. 2021 Jan 9:1-3. [ Links ]
3. Sedghizadeh PP, Nguyen M, Enciso R. Intracranial physiological calcifications evaluated with cone beam CT. Dentomaxillofacial Radiology. 2012 Dec; 41(8):675-8. [ Links ]
 Correspondence:
Correspondence:
Z Yakoob
Department of Oral Pathology and Oral Biology
Faculty of Health Sciences, University of Pretoria
E-mail: zarah.yakoob@up.ac.za
Authors contribution:
Dr Zarah Yakoob: 70%
Dr Chané Smit: 30%
