










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.79 n.9 Johannesburg 2024
CASE REPORT
Lymphangioma: A Rare Intraoral Cystic Lesion
A OdendaalI; A KassanII; A AfroghehIII
IBChD; Department of Oral Medicine and Perlodontology, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
IIBDS (WITS), MChD (MFOS), PDD (IMPLANTOLOGY), PDD (FORENSIC PATHOLOGY) (UWC); Chief Specialist and part time senior consultant, Livingstone Hospital, Department of Oral and Maxillofacial Surgery
IIIBChD, MSc, MChD, PhD; Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, University of the Western Cape, Extraordinary Senior Lecturer, Division of Anatomical Pathology, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
CASE PRESENTATION
A 34-year-old female presented to an Oral and Maxillofacial surgeon with a complaint of a large painful cystic mass of her right upper lip. The patient mentioned that the lesion has been gradually increasing in size over the past few years. She also reported that the cystic mass was previously aspirated by an Oral and Maxillofacial surgeon who advised her to closely monitor the lesion. The patient had no medical history of note. She was taking Mypaid Forte tablets for pain relief and was using Gum Paroex 300 ml oral rinse twice daily. Extraoral examination was unremarkable. Intraoral examination revealed a 3 x 2 cm bluish submucosal cystic lesion of the right upper lip (Figure 1).

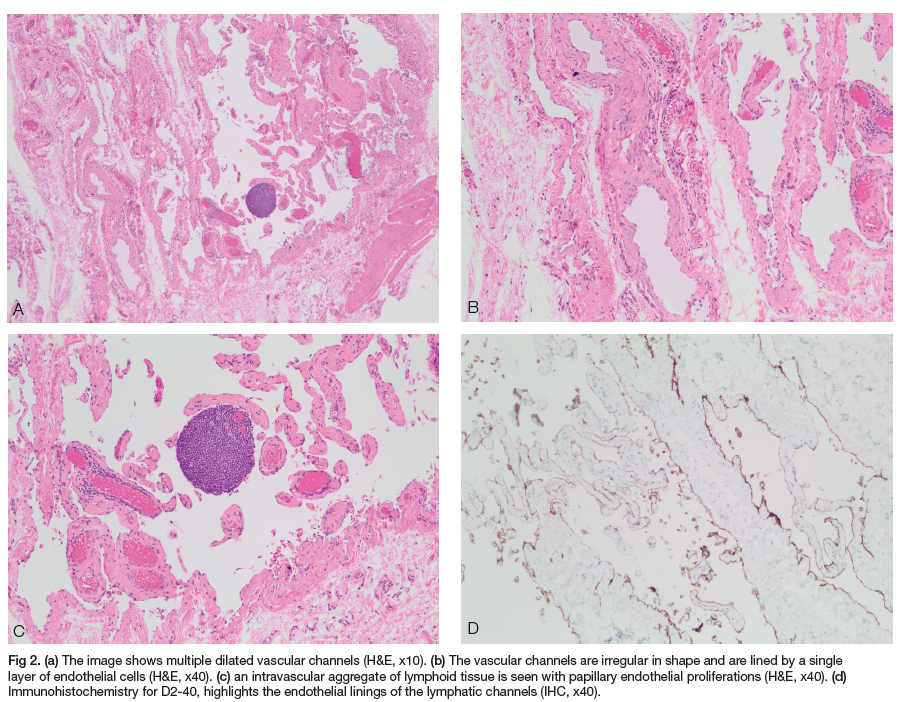
The clinical differential diagnosis included cystic benign and malignant salivary gland neoplasms that commonly involve the upper lip (pleomorphic adenoma, canalicular adenoma and mucoepidermoid carcinoma), arterio-venous malformations, namely hemangioma and lymphangioma, and mucocele (although a rare occurrence in the upper lip). An excisional biopsy was performed under local anaesthesia. The excised specimen was placed in formalin and sent to the pathology laboratory for histological evaluation. Microscopic examination revealed dilated irregular large vascular channels lined by a single layer of flattened endothelial cells (Figures 2 a,b). Focally the ectatic vascular spaces contained aggregates of lymphoid tissue and endothelial cell proliferations (Figure 2 c). The endothelial cells were positive for the immunomarker D2-40 (podoplanin) (Figure 2 d). Based on the histolgical features and the immunhistochemical positivity for podoplanin, a diagnosis of cavernous lymphangioma was established.
DISCUSSION
Lymphangiomas are characterized by abnormal proliferation of lymphatic vessels that have no communication with the normal lymphatic system. Recently, lymphangiomas have been linked to a somatic mutation in PIK3CA gene, suggesting a neoplastic aetiology.1 For the latter reason the World Health Organization (WHO) Classification of Tumours continues to use the term "lymphangioma" instead of vascular malformation.2 Lymphangiomas are very rare and preferentially affect the head and neck region. Most cases occur in children and young adults. In the oral cavity, the most frequently affected anatomical location is the tongue, followed by the lip. Clinically, lymphangiomas are slow-growing often translucent cystic lesions.3
Oral lymphangiomas can be classified microscopically into (a) capillary (microcystic) lymphangioma, composed of small lymphatic vessels and (b) cavernous (macrocystic) lymphangioma, exhibiting large, dilated lymphatic vessels.2 Histologically, lymphangiomas are characterized by the presence of several dilated vascular channels, that are lined by a single flattened layer of endothelial cells. The vascular spaces often contain a proteinaceous material (lymph). Intravascular and stromal lymphoid tissue is usually observed.2 Some capillary lymhangiomas dissect around normal tissue structures and can cross tissue planes. These capillary lymphangiomas pose a high risk for recurrence and may be irresectable. Immunohistochemical staining for podoplanin - an endothelial lymphatic marker -and/or PROX1 is often used to differentiate lymphangiomas from haemangiomas.4
Surgical excision is the preferred treatment of choice for most cases since spontaneous regression of these lesions is rare.3 Sclerotherapy is a minimally invasive, safe and highly effective procedure, ideal for recurrent/irresectable oral lymphangiomas.5 Various sclerosing agents have been employed in the treatment of oral lymphangiomas. OK-432 is the ideal sclerosing agent with no perilesional fibrosis evident following use. Ethanolamine oleate (Ethamolin®) is the most widely and least toxic agent used with good clinical response rates.6,7 Successful treatment of a case of a tongue lymphangioma with Everolimus (an mTOR inhibitor) targeting the PIK3A gene pathway has been reported.8
It is important for oral health care professionals to understand the clinicopathological presentation of this rare entity and include oral lymphangiomas in their differential diagnosis of cystic oral lesions. A better understanding of the etiopathogenesis of oral lymphangiomas may also help adopt appropriate and personalized therapeutic measures.
REFERENCES
1. Liu, X., Cheng, C., Chen, K., Wu, Y. and Wu, Z., 2021. Recent progress in lymphangioma. Frontiers in Pediatrics, 9, p.735832. [ Links ]
2. Jo VY Fletcher CDM. WHO classification of soft tissue tumours: an update based on the 2013 (4th) edition. Pathology. 2014;46(2):95-104. https://doi.org/10.1097/PAT.0000000000000050 [ Links ]
3. da Cruz Lima, J.G., Gonçalo, R.I.C., Pinheiro, J.C., da Silva, G.G., de Oliveira Costa, C.S., Queiroz, L.M.G. and de Oliveira, P.T., 2024. Oral lymphangioma: A clinicopathological analysis of 40 cases and review of the literature. Oral Surgery. [ Links ]
4. Kolay SK, Parwani R, Wanjari S, Singhal P. Oral lymphangiomas -clinical and histopathological relations: an immunohistochemically analyzed case series of varied clinical presentations. J Oral Maxillofac Pathol. 2018;22:108-11. https://doi.org/10.4103/jomfp.JOMFP_157_17 [ Links ]
5. Costa JRS, Torriani MA, Hosni ES, D'avila OP, Figueiredo PJ. Sclerotherapy for vascular malformations in the oral and maxillofacial region: treatment and follow-up of 66 lesions. J Oral Maxillofac Surg. 2011;69:88-92. https://doi.org/10.1016/j.joms.2010.06.204 [ Links ]
6. Kato CNAO, Ribeiro MC, Amaral MBF Grossmann SM, Aguiar MCF, Mesquita RA. Experience with 5% ethanolamine oleate for sclerotherapy of oral vascular anomalies: a cohort of 15 consecutive patients. J Craniomaxillofac Surg. 2019;47:106-11. https://doi.org/10.1016/j.jcms.2018.11.009 [ Links ]
7. Fernandes DT, Elias RA, Santos AR, Vargas PA, Lopes MA. Benign oral vascular lesions treated by sclerotherapy with ethanolamine oleate: a retrospective study of 43 patients. Med Oral Patol Oral Cir Bucal. 2018;23(2):180-7. https://doi.org/10.4317/medoral.22253 [ Links ]
8. Chang, Y.H., Wu, C.L., Yang, H.S., Huang, H.Y., Lin, Y.J., Hsiao, J.R., Hsu, C.K. and Li, Y.L., 2024. Successful treatment with everolimus for microcystic lymphangioma of the tongue caused by a somatic PIK3CA mutation. Dermatologica Sinica, 42(1), pp.54-55. [ Links ]
Reprint requests:
Amir Afrogheh, BChD, MSc, MChD, PhD
Department of Oral and Maxillofacial Pathology
Tygerberg Hospital, Cape Town, South Africa
Email: amir.afrogheh@nhls.ac.za

{kind=link}