










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.79 n.10 Johannesburg Nov. 2024
https://doi.org/10.17159/sadj.v79i10.19172
REVIEW
Perspectives on the Minamata Convention and dental amalgam waste management in South Africa
SM SudiI; S NaidooII
IDDS, MSc, Faculty of Dentistry, University of Western Cape, Cape Town, South Africa ORCID: 0009-0003-2223-7244
IIBDS, LDS.RCS, MDPH, DDPH.RCS, MChD, PhD, Dip IRE, DSc, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa ORCID: 0000-0001-7424-8082
ABSTRACT
The Minamata Convention on Mercury (MCM), a pivotal multilateral agreement, is dedicated to controlling human sources of mercury environmental release. Due to their unique properties, mercury and its compounds were extensively used in products and industrial processes. Human activities have escalated atmospheric mercury levels by 450%, causing severe environmental and life-threatening consequences. The MCM focuses on restricting mercury mining, phasing out and phasing down mercury use in products and processes, controlling environmental emissions and regulating small-scale gold mining. Dental amalgam restorative material is the only product subject to a phase-down approach through the prevention of dental caries, research for alternative restorative materials, and waste management practices. The increasing understanding of mercury's health and environmental impacts has led to restricting dental amalgam use in pregnant women and children, phase-out in several countries, and cessation of the marketing of dental amalgam by some manufacturers. This perspective delves into the current approaches to managing dental amalgam waste and proposes improvements to dental amalgam waste management practices in South Africa.
Keywords: Minamata Convention, mercury, dental amalgam, dental amalgam waste
Introduction
The 2013 Minamata Convention on Mercury (MCM), the 2001 Stockholm Convention on Persistent Organic Pollutants, the 1998 Rotterdam Convention on Prior Informed Consent Procedure for certain Hazardous Chemicals and Pesticides in International Trade and the 1989 Basel Convention on the Control are all global multilateral and legally binding environmental agreements that aim to protect human health and the environment from hazardous chemicals and waste.1 The MCM came into force on August 16 2017 and sought to control the anthropogenic release of mercury throughout its life cycle.2 The MCM focuses on banning new mercury mines, phasing out existing mines, phasing out and phasing down mercury use in products and processes, controlling environmental emissions, and regulating the informal sector of artisanal and small-scale gold mining.3 The MCM is of interest to oral health practitioners because of the potential environmental release of mercury waste from dental amalgam restorative material. The dental amalgam restorative material comprises 43-50% liquid mercury, which forms an intermetallic alloy with varying amounts of silver, tin, copper, zinc and palladium.4 In the MCM, dental amalgam is subject to a phase-down approach based on prevention, research for alternative materials, and waste management practices. The debate on the use of dental amalgam in South Africa has been reignited by the recent publication of the Department of Forestry, Fisheries and the Environment's amended draft national regulations for the management of mercury in South Africa to stakeholders.5 2024 is the fifth year since South Africa acceded as a party to the MCM.6
Brief background of mercury in the environment
Mercury is a naturally occurring element, the only liquid metal at room temperature. It exists in multiple oxidative states, inorganic salts and organic complexes,7 all of which present with varied chemical affinities, biological activity and toxicity.8 Mercury's chemical and physical properties have led to its widespread use in various products and manufacturing processes, leading to detrimental environmental release and human exposure.9 Other sources of environmental mercury release are geologic processes such as volcanic activities.10 Human activities have increased total atmospheric mercury concentration by about 450% above natural levels.9 In a 2010 report by Masekoameng et al South Africa was ranked as the sixth largest emitter of mercury, releasing 29.47t, with 80% of the emissions originating from coal-fired power generation.11
Mercury is a recognised global pollutant that persists in the environment, bioaccumulates and biomagnifies in the food chain and has adverse health effects on human health, animal life and the environment.3 Human exposure occurs mainly through the ingestion of fish and other marine species contaminated with organic mercury or through contact with mercury used in products and processes, such as artisanal and small-scale gold mining.12 The World Health Organization (WHO) has described mercury as one of the 10 chemicals of public health concern.13
The most significant and catastrophic mercury poisoning occurred in Minamata, Japan. In 1932, the Chisso factory started producing acetaldehyde using inorganic mercury as a catalyst and released effluent into the Minamata Bay and the Shiranui Sea. Minamata Bay residents reported dwindling fish catches, deranged flight in crows, and cats exhibiting
strange movements, convulsions and deaths.14 In April 1956, two sisters, aged five and two, presented with unexplained neurological symptoms at Chisso Hospital and, by August 1956, 30 cases and 11 deaths were attributed to "Minamata Disease".15
Methylmercury, a by-product in synthesising acetaldehyde, was recognised as the cause of neurological symptoms in October 1959.16 The released methylmercury bioaccumulated in marine life, a staple diet of the Minamata population, leading to acute and chronic methylmercury poisoning.17 More than 2,000 individuals were officially recognised as Minamata Disease patients, with several tens of thousands exhibiting neurological symptoms characteristic of methylmercury poisoning.18 The Minamata convention is named after the Minamata Bay disaster, a remembrance of the lives lost and a commitment to addressing the anthropogenic release of mercury.
It is well known that the consumption of marine life contaminated with methylmercury is associated with long-term neurocognitive deficits in exposed children and increased cardiovascular risks in adults.19 The health risks of consuming marine life contaminated with methylmercury are similarly pertinent to South Africa. In 2015, mercury levels higher than the recommended levels by the WHO in some fish samples from Cape Town and Durban were reported, leading to the release of a dietary advisory for allowable fish consumption in South Africa.20
South Africa has witnessed the ravages of mercury poisoning and environmental contamination through industrial exposure and artisanal and small-scale gold mining (ASGM). Occupational exposure of 30 workers (two of them fatally) at a mercury processing plant owned by Thor Chemicals and environmental contamination of the Mngceweni River in KwaZulu-Natal were reported in the 1990s.21 In a study conducted in 1999, fish collected from the local water streams downstream of the Thor plant exhibited elevated mercury levels.22 Ten years later, Papu-Zamxaka et al described elevated mercury levels in fish and soil samples from the uMgeni River and in hair samples from individuals who consumed fish from the uMgeni River and the Inanda Dam.23
The Thor Chemicals saga further offers a glimpse at the challenges of long-term storage of mercury waste in a developing country. Mercury waste originating from the Thor Chemicals site has been subject to fires at a processing plant and the A-Thermal processing plant in Gauteng and pilfering at the plant site in Cato Manor, potentially leading to further environmental releases and contamination.24
Artisanal and small-scale gold miners' informal and unregulated mining is prevalent in disused and functioning gold mines in South Africa and the Southern African region.25 Artisanal and small-scale gold mining (ASGM) utilises elemental mercury to extract gold from ore. The mercury vapour released can potentially cause neurological, cognitive and several other health problems for miners and communities.26,27ASGM is currently the largest source of mercury pollution in the world, contributing 38%, or 838 tonnes, of mercury released into the environment. In Sub-Saharan Africa, emissions from ASGM account for 70%-85%.9 South Africa is a major mercury trade hub in Sub-Saharan Africa. A regional report on the mercury trade and use for ASGM in Sub-Saharan Africa indicated that mercury destined for ASGM activities might be imported as dental amalgam and liquid mercury imported for dental use is used for ASGM.28 As more controls are introduced in the mercury trade, it is essential to apply standards and custom codes that ensure dental amalgam is unavailable in mercury and alloy bulk forms that facilitate diversion to ASGM in the region.
Dental amalgam in the Minamata Convention
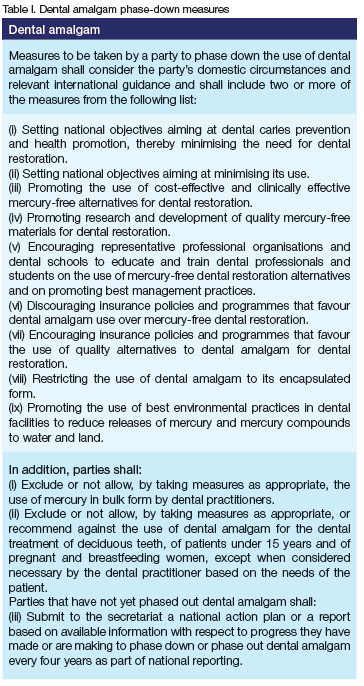
In the MCM, dental amalgam is the only mercury-added product subject to a phase-down approach based on prevention, research for alternative materials and waste management practices.3 Annex A Part II of the Convention addresses provisions aimed at a phase-down of dental amalgam, of which a party shall implement two or more of the nine measures (Table I). In 2022, the fourth conference of parties of the MCM added three more provisions on restricting the use of bulk dental amalgam, restricting the use of dental amalgam in children under 15 years of age, pregnant and breastfeeding mothers, and on reporting mechanisms for national action plans for countries that are yet to phase out dental amalgam.29
Additionally, the MCM mandates that mercury waste be managed in an environmentally sound manner by considering the guidelines developed under the Basel Convention on the Control of Transboundary Movements of Hazardous Wastes and Their Disposal. The environmentally sound management of mercury framework guides handling, interim storage, transportation, treatment, recovery, stabilisation, solidification and long-term storage. The United Nations Environment Programme (UNEP) developed a practical sourcebook,30 updated the guidelines31 and produced a catalogue of technologies and services for mercury waste management32 to facilitate the environmentally sound management of mercury waste. Oral health practitioners need to be aware of the current management protocols for mercury waste, as they are likely to affect the cost of dental amalgam and waste management services.
Dental amalgam use and waste management in South Africa
The global mercury consumption in dental applications in 2015 was estimated at an average of 274 tonnes, with sub-Saharan Africa consuming between 5 and 9 tonnes of mercury.9 Dental amalgam is an essential restorative material in primary oral health care provision in South Africa.33 The estimates of dental amalgam usage in South Africa obtained by use from the 2011 inventory of mercury releases suggest that 70-100kg of dental amalgam was sold annually between 2009 and 2011, with a further 50kg of non-amalgamated mercury sold to dental practitioners.34
The use of dental amalgam produces waste, which poses a risk of mercury contamination in the environment,35 through direct wastewater discharge, incineration of healthcare waste, landfilling, sewage sludge incineration, cremation and burials.36 Dental amalgam waste is categorised as noncontact and contact amalgam waste. Used capsules and amalgam scraps form non-contact amalgam waste, while contact amalgam waste is composed of carved amalgam, amalgam captured in chairside traps, vacuum pump filters and extracted teeth.36 Drummond et al estimated that without proper waste management, about 50% of dental amalgam used in restorations could end up in the waste stream.37 Dental amalgam particles settle in wastewater lines, leading to continuous leaching of mercury, exacerbated by the use of oxidising wastewater cleaning agents.38 The production of organic methyl mercury in dental wastewater lines by sulphate-reducing bacteria has been previously reported.39
Managing dental amalgam waste in developing countries is challenging, and containment systems are neither affordable nor readily available. In the East Arica Dental Amalgam Phase-down Project (EADAP), the high cost of mercury waste containment systems and lack of processing facilities were described as significant challenges.40 The informal global WHO consultation with policymakers in dental public health on implementing the Minamata Convention on Mercury reported that only nine percent of countries in the African region have phased out the use of dental amalgam, 30% have no plan to phase out dental amalgam and only 17%-23% of the countries still using dental amalgam have regulations on dental amalgam waste and disposal.41 The risks of environmental contamination with mercury from dental amalgam and the increasing knowledge of the dangers posed by mercury releases have created new dynamics and considerations for dental amalgam use in developing countries.
In South Africa, the regulatory framework for healthcare risk waste is provided by a set of acts, regulations, norms and standards, mainly from the Department of Environmental Affairs through the National Environmental Management: Waste Act (Act 59 of 2008), the National Department of Health, National Health Act (Act No. 61 of 2003) and various provincial legislation and regulations.42 Healthcare waste in South Africa is categorised into two main groups: healthcare risk waste (HCRW), which is infectious or hazardous, and healthcare general waste (HCGW), similar to domestic waste.43 An estimated 48,749 tonnes of healthcare risk waste were generated in South Africa in 2017, with waste management services provided by 15 operational HCRW facilities.44 The South African Bureau of Standards developed the available guidelines for managing healthcare waste in South Africa. The South African National Standard SANS 10248-3 provides guidelines on managing healthcare risk waste from minor generators, with oral healthcare centres listed among the intended. The guideline adequately outlines requirements for oral health care professionals in the general responsibilities documentation, contractual commitments with waste management firms, training, workplace hygiene and health and safety, guidelines in identification, classification, segregation, collection and packaging of health care waste, characteristics of storage areas, and modalities of transportation, treatment and disposal of healthcare waste.45 The guideline falls short of the current dental amalgam waste management standards known as the Best Management Practices for Dental Amalgam Waste (BMPs).46 The American Dental Association developed the BMPs and introduced an accompanying guide for incorporating BMPs into dental practice.47 The BMPs and accompanying guide for incorporating BMPs into dental practices were later adopted by the World Health Organization.48 Developing a new healthcare waste guideline for oral health services in line with internationally recognised standards will facilitate the proper management of amalgam waste and meet a measure stipulated in the Minamata Convention. Furthermore, local development and manufacture of technologies such as containment systems and separators will facilitate adaptation of the new guidelines and provide for the growth of circular economy opportunities in the country and the region.
The Department of Environmental Affairs (DEA) promoted appropriate traps in dental wastewater to prevent potential mercury contamination from using dental amalgam49 and, furthermore, the South African Dental Association (SADA) advocated the introduction of BMPs for dental amalgam use to prevent environmental mercury contamination.50 Recently, the Department of Forestry, Fisheries and the Environment released the amended draft of national regulations for the management of mercury in South Africa to stakeholders. In the draft regulations, dental amalgam phase-down approaches include limiting the use in pre-dosed encapsulated form, ensuring the installation of amalgam separators in dental facilities from 1 April 2025, curbing the release of dental amalgam into the environment and providing guidelines for phase-down plans. The contravention of regulations related to dental amalgam is an offence liable to a fine and/or imprisonment.5
The standard for dental amalgam used in South Africa is an identical implementation of the international standard ISO 24234:2004. In the standard, the amalgam alloy can be packaged as powder in bulk or tablets, with the mercury supplied in bulk or sachets, or both mercury and alloy supplied in a pre-dosed capsuie.51 In response to measures stipulated in the Minamata Convention, a new dental amalgam standard, ISO 20749:2023, was developed to enable countries that do not allow the use of products other than pre-capsulated amalgam to use the ISO Standard.52
Adapting this new standard will help enforce dental amalgam availability in South Africa in pre-capsulated form and enable the country to meet the requirements of the additional measures stipulated in the Minamata Convention.
SADA entered into a collaboration with Dental Recycling International, which facilitated the availability of amalgam separators in South Africa.53 This commendable initiative should be coupled with introducing BMPs, containment systems for noncontact amalgam waste, amalgam waste treatment and disposal vendors, and infrastructure to support the disposal and long-term storage of mercury waste.
CONCLUSION
The Southern African region faces challenges in providing oral health services due to limited financial and human resources, limited access and affordability, poverty and a higher burden of diseases.54 The provision of restorative treatment has been problematic due to the lack of basic oral health care packages in the Western Cape, where less than 31.5% of dental clinics offer a basic treatment package.55 Dental amalgam has long been known to be an affordable restorative material compared to other restorative materials.56 However, the affordability of amalgam is historical: when amalgam was introduced, the alternative restorative material was gold, which was beyond the reach of many.57 It is noteworthy to recognise that most studies that compare the affordability of dental amalgam do not consider the environmental, health and social management costs of continual usage of dental amalgam.58 The increasing knowledge of the effect of mercury on health and the environment has led to the banning of amalgam use in pregnant women and children, advanced phase-out processes in several countries and the cessation of the marketing of dental amalgam by some manufacturers.59
South Africa, the continent's second-largest economy, is in the process of introducing a national health insurance scheme to promote quality, affordable and universal health coverage.60 Dental amalgam is an essential restorative material in primary oral health care provision in South Africa33 and the use of dental amalgam is still taught in South Africa's dental schools.61 An in-depth analysis of the benefits of the continued use of dental amalgam is urgent, considering the complexities related to dental amalgam waste management, the impending phase-out in most developed countries that are a source of amalgam and the cost of waste management technologies.
Conflict of interest
The authors declare the manuscript was developed without commercial or financial relationships that could create a conflict of interest.
Funding
The authors funded the development of the manuscript.
REFERENCES
1. Koloutsou-Vakakis S, Chinta I. Multilateral Environmental Agreements for Wastes and Chemicals: 40 Years of Global Negotiations. Environ Sci Technol. 2011 Jan 1;45(1):10-5. Available from: https://doi.org/10.1021/es101373n [ Links ]
2. UNEP. New convention calls time on mercury poisoning. UN Environment. 2017. Available from: http://www.unep.org/news-and-stories/press-release/new-convention-calls-time-mercury-poisoning [ Links ]
3. UNEP. Minamata Convention on Mercury: Text and Annexes. 2023. Available from: https://minamataconvention.org/sites/default/files/documents/2023-10/Minamata-Convention-booklet-Oct2023-EN.pdf [ Links ]
4. Sakaguchi R, Ferracane J, Powers J, editors. Chapter 10 - Restorative Materials: Metals. In: Craig's Restorative Dental Materials (14th Edition). Philadelphia: Elsevier; 2019. p. 171-208 [ Links ]
5. Department of Forestry, Fisheries and the Environment, South Africa. National Environment Act, 1998, (Act No 107 of 1998), Consultation on the Draft National Regulations for the Management of Mercury in South Africa. 2023 [ Links ]
6. UNEP. South Africa brings to 108 the number of Parties to the Minamata Convention | Minamata Convention on Mercury. 2019. Available from: https://minamataconvention.org/en/news/south-africa-brings-108-number-parties-minamata-convention [ Links ]
7. Broussard LA, Hammett-Stabler CA, Winecker RE, Ropero-Miller JD. The Toxicology of Mercury. Lab Med. 2002;33(8):614-25 [ Links ]
8. Gworek B, Dmuchowski W, Baczewska-Dabrowska AH. Mercury in the terrestrial environment: a review. Environ Sci Eur . 2020 Oct 2;32(1):128. Available from: https://doi.org/10.1186/s12302-020-00401-x [ Links ]
9. AMAP/UNEP. Technical Background Report for the Global Mercury Assessment 2018/Global Mercury Partnership. Arctic Monitoring and Assessment Programme, Oslo, Norway/UN Environment Programme, Chemicals and Health Branch, Geneva Switzerland. 2019. Available from: https://www.unep.org/globalmercurypartnership/resources/report/technical-background-report-global-mercury-assessment-2018 [ Links ]
10. Geyman BM, Thackray CP, Jacob DJ, Sunderland EM. Impacts of Volcanic Emissions on the Global Biogeochemical Mercury Cycle: Insights from Satellite Observations and Chemical Transport Modeling. Geophys Res Lett. 2023;50(21): e2023GL104667. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1029/2023GL104667 [ Links ]
11. Masekoameng KE, Leaner J, Dabrowski J. Trends in anthropogenic mercury emissions estimated for South Africa during 2000-2006. Atmos Environ. 2010 Aug;44(25):3007-14. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1352231010003791 [ Links ]
12. Beckers F, Rinklebe J. Cycling of mercury in the environment: Sources, fate, and human health implications: A review. Crit Rev Environ Sci Technol. 2017 May 3;47(9):693-794. Available from: https://www.tandfonline.com/doi/full/10.1080/10643389.2017.1326277 [ Links ]
13. WHO. 10 chemicals of public health concern. 2020. Available from: https://www.who.int/news-room/photo-story/photo-story-detail/10-chemicals-of-public-health-concern [ Links ]
14. Jenks AL. Chapter 1: The Minamata Disaster and the True Cost of Japanese Modernization.pdf. In: Perils of Progress: environmental disasters in the twentieth century. 1st ed. Prentice Hall; 2011. p. 159. Available from: https://searchworks.stanford.edu/view/8658738 [ Links ]
15. Mcalpine D, Araki S. MINAMATA DISEASE AN UNUSUAL NEUROLOGICAL DISORDER CAUSED BY CONTAMINATED FISH. The Lancet. 1958 Sep;272(7047):629-31. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673658903489 [ Links ]
16. Yorifuji T, Tsuda T, Harada M. Chapter 5 Minamata disease: a challenge for democracy and justice. In: Late lessons from early warnings: science, precaution, innovation. Luxembourg: European Environment Agency; 2013. p. 764. Available from: https://data.europa.eu/doi/10.2800/73322 [ Links ]
17. Ekino S, Susa M, Ninomiya T, Imamura K, Kitamura T. Minamata disease revisited: An update on the acute and chronic manifestations of methyl mercury poisoning. J Neurol Sci. 2007 Nov 15;262(1):131-44. Available from: https://www.sciencedirect.com/science/article/pii/S0022510X07004558 [ Links ]
18. Hachiya N. Epidemiological Update of Methylmercury and Minamata Disease. In: Ceccatelli S, Aschner M, editors. Methylmercury and Neurotoxicity. Boston, MA: Springer US; 2012. p. 1-11. Available from: https://doi.org/10.1007/978-1-4614-2383-6_1 [ Links ]
19. Karagas MR, Choi AL, Oken E, Horvat M, Schoeny R, Kamai E, et al. Evidence on the Human Health Effects of Low-Level Methylmercury Exposure. Environ Health Perspect. 2012 Jun;120(6):799-806. Available from: https://ehp.niehs.nih.gov/doi/10.1289/ehp.1104494 [ Links ]
20. Carstens J. SEE: Potentially dangerous mercury levels in SA retail fish. Life. 2016. Available from: https://www.news24.com/life/archive/see-potentially-dangerous-mercury-levels-in-sa-retail-fish-20161101 [ Links ]
21. Dixon N. South Africa: bosses who kill | Green Left. 1993. Available from: https://www.greenleft.org.au/content/south-africa-bosses-who-kill [ Links ]
22. Oosthuizen J, Ehrlich R. The impact of pollution from a mercury processing plant in KwaZulu-Natal, South Africa, on the health of fish-eating communities in the area: An environmental health risk assessment. Int J Environ Health Res. 2001 Apr 1;11:41-50 [ Links ]
23. Papu-Zamxaka V, Mathee A, Harpham T, Barnes B, Röllin H, Lyons M, et al. Elevated mercury exposure in communities living alongside the Inanda Dam, South Africa. J Env Monit. 2010;12(2):472-7 [ Links ]
24. Carnie T. At long last, Thor's poisonous mercury is getting cleaned up. Daily Maverick. 2021. Available from: https://www.dailymaverick.co.za/article/2021-04-17-at-long-last-thors-poisonous-mercury-is-getting-cleaned-up/ [ Links ]
25. Madimu T. 'Illegal' gold mining and the everyday in post-apartheid South Africa. Rev Afr Polit Econ. 2022 Jul 3;49:436. Available from: https://www.scienceopen.com/doi/10.1080/03056244.2022.2027750 [ Links ]
26. Esdaile LJ, Chalker JM. The Mercury Problem in Artisanal and Small-Scale Gold Mining. Chem - Eur J. 2018;24(27):6905-16. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/chem.201704840 [ Links ]
27. George J, Sadiq E, Moola I, Maharaj S, Mochan A. Informal gold miners with mercury toxicity: Novel asymmetrical neurological presentations. S Afr Med J. 2023 Dec 4;113(12):20. Available from: https://samajournals.co.za/index.php/samj/article/view/1127 [ Links ]
28. World Bank. Mercury Trade and use for Artisanal and Small-scale Gold Mining in Sub-Saharan Africa. World Bank/COWI; 2016 [ Links ]
29. UNEP. Annex A to the Minamata Convention on Mercury, as amended by the Conference of Parties at its fourth meeting. Mercury-added products. Minamata Convention on Mercury; 2022. Report No.: UNEP/MC/COP.4/Dec.3/Add.1. Available from: https://minamataconvention.org/sites/default/files/documents/decision/4_Dec3_Add1_Amendment.English.pdf [ Links ]
30. UNEP. Practical Sourcebook on Mercury Waste Storage and Disposal. 2015. Available from: https://wedocs.unep.org/bitstream/handle/20.500.11822/9839/-Practical_Sourcebook_on_Mercury_Waste_Storage_and_Disposal-2015Sourcebook_Mercruy_FINAL_web.pdf [ Links ]
31. UNEP. Technical guidelines on the environmentally sound management of waste consisting of, containing or contaminated with mercury or mercury compounds. 2023 [ Links ]
32. UNEP. Catalogue of Technologies and Services on Mercury Waste Management. UNEP Global Mercury Partnership Waste Management Area; 2024. Available from: https://wedocs.unep.org/bitstream/handle/20.500.11822/27819/WMA_catalog.pdf [ Links ]
33. Department of Health, South Africa. Norms, Standards and Practice Guidelines for Primary Oral Health Care. 2005 [ Links ]
34. Departments of Environmental Affairs, South Africa. Inventory of Mercury releases in South Africa. Pretoria: Department of Environmental Affairs; 2011 [ Links ]
35. Jones DW. Putting dental mercury pollution into perspective. Br Dent J. 2004 Aug 28;197(4):175-7 [ Links ]
36. Jokstad A, Fan P. Amalgam waste management. Int Dent J. 2006 Jun 1;56(3):147-53. Available from: https://www.sciencedirect.com/science/article/pii/S0020653920343392 [ Links ]
37. Drummond JL, Cailas MD, Croke K. Mercury generation potential from dental waste amalgam. J Dent. 2003 Sep;31(7)493-501 [ Links ]
38. Stone M, Kuehne J, Cohen M, Talbott J, Scott J. Effect of iodine on mercury concentrations in dental-unit wastewater. Dent Mater. 2006 Feb;22(2):119-24. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0109564105001387 [ Links ]
39. Zhao X, Rockne KJ, Drummond JL, Hurley RK, Shade CW, Hudson RJM. Characterization of methyl mercury in dental wastewater and correlation with sulfatereducing bacterial DNA. Environ Sci Technol. 2008 Apr 15;42(8):2780-6 [ Links ]
40. MUHAS. Promoting the 'phase down' Approach of Dental Amalgam in Developing Countries - Tanzania. Dar es Salaam, Tanzania: Muhimbili University of Health and Allied Sciences (MUHAS); 2014. Available from: https://wedocs.unep.org/bitstream/handle/20.500.11822/31412/EADA_Tanzania.pdf [ Links ]
41. WHO. Report of the informal global WHO consultation with policymakers in dental public health, 2021: monitoring country progress in phasing down the use of dental amalgam. Geneva; 2021. Available from: https://iris.who.int/bitstream/handle/10665/348985/9789240038424-eng.pdf [ Links ]
42. Jansen KE, Kocks DJ, Roberts H. Healthcare risk waste and waste legislation in South Africa. Occup Health South Afr. 2017 Nov;23(6):15-7 [ Links ]
43. Department of Health, South Africa. The National Health Act, 2003 (Act No. 61 of 2003) Regulations relating to Health Care Waste Management in Health Establishments. Government Gazette No 37654; 2014. Available from: https://www.gov.za/sites/default/files/gcis_document/201409/37654rg10195gon375.pdf [ Links ]
44. Departments of Environmental Affairs, South Africa. 2017 Health Care Risk Waste Treatment Figures. 2019. Report No.: Draft SAEO2019 [ Links ]
45. SABS Standards Division. SOUTH AFRICAN NATIONAL STANDARD 10248.3.2011. Management of healthcare risk waste from minor generators - Registered healthcare professionals and non-healthcare professionals.pdf. 2011 [ Links ]
46. Author
47. ADA. Best Management Practices for Amalgam Waste. 2007. Available from: https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/research/oral-health-topics/topics_amalgamwaste_brochure.pdf [ Links ]
48. WHO. Future use of materials for dental restoration. 2010. 65 p. Available from: https://www.who.int/publications/i/item/9789241500647 [ Links ]
49. Department of Environmental Affairs, South Africa. Analysis of Mercury in the Health Care Sector. Department of Environmental Affairs; 2011. Available from: https://noharm-europe.org/sites/default/files/documents-files/2679/SA_Mercury_Report.pdf [ Links ]
50. SADA. Dental Amalgam - Position Statement [Internet]. 2014. Available from: https://www.sada.co.za/Dental_Amalgam [ Links ]
51. SABS Standards Division. SOUTH AFRICAN NATIONAL STANDARD 24234,2008, Dentistry, Mercury and alloys for dental amalgam.pdf. 2008 [ Links ]
52. ISO. ISO 20749:2023, Dentistry; Pre-capsulated Amalgam. 2023. Available from: https://www.iso.org/standard/82859.html [ Links ]
53. Makhubele KC. Starting in 2023, SADA members can purchase amalgam separators at discounted prices. South Afr Dent J. 2023 Mar 9;78(01):2-2. Available from: https://journals.assaf.org.za/index.php/sadj/article/view/15708 [ Links ]
54. World Health Organization. Global oral health status report: towards universal health coverage for oral health by 2030: regional summary of the African Region. 2023 p. viii, 24 p. Available from: https://iris.who.int/bitstream/handle/10665/366662/9789240070769-eng.pdf [ Links ]
55. Smit D, Osman Y. The availability of the basic oral health care package in the Western Cape. South Afr Dent J. 2017;72(6). Available from: http://ref.scielo.org/b955gm [ Links ]
56. Mark A. Amalgam fillings: safe, strong, and affordable. J Am Dent Assoc 1939. 2019 Oct 1;150:894 [ Links ]
57. Forrai J. HISTORY OF AMALGAM IN DENTISTRY. Rev Clin Pesq Odontol Vol 3 No 1 2007. 2007;3(1):65-71 [ Links ]
58. Schwendicke F, Göstemeyer G, Stolpe M, Krois J. Amalgam Alternatives: Cost-Effectiveness and Value of Information Analysis. J Dent Res. 2018 Nov;97(12):1317-23. Available from: http://journals.sagepub.com/doi/10.1177/0022034518782671 [ Links ]
59. Tibau AV, Grube BD. Dental Amalgam and the Minamata Convention on Mercury Treaty: Make Mercury History for All. J Oral Dent Health. 2023 Sep;7(3). Available from: https://www.opastpublishers.com/open-access-articles/dental-amalgam-and-the-minamata-convention-on-mercury-treaty-make-mercury-history-for-all.pdf [ Links ]
60. Malele-Kolisa Y. Unpacking the NHI Bill recently passed by parliament in May 2023: Implications for oral health. South Afr Dent J. 2023 Dec 23;78(09):467-8. Available from: https://journals.assaf.org.za/index.php/sadj/article/view/17496 [ Links ]
61. Essa AY, Ahmed S, Dyason A, Karjiker F, Adam RZ. Teaching and placement of dental amalgam restorations at South African dental schools. Front Oral Health. 2023 Jul 19;4. Available from: https://www.frontiersin.org/journals/oral-health/articles/10.3389/froh.2023.1118361/full [ Links ]
 Correspondence:
Correspondence:
Stephen M Sudi
Email: ssudi@uwc.ac.za
Author's contribution
1. Stephen M Sudi: conceptualisation, draft preparation (60%)
2. Sudeshni Naidoo: draft preparation, review and editing (40%)
