










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.80 n.1 Johannesburg Feb. 2025
https://doi.org/10.17159/sadj.v80i01.19967
REVIEW
Sialolithiasis and urolithiasis - coincidence or correlation? A systematic review
S MaharajI; A AdamII
IMBBCh, MMed, FCORL, Shivesh.maharaj@wits.ac.za; +27 76 120 4066. Postal: 7th York Road, Medical School, 9th Floor, Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, Parktown, 2193, South Africa. Charlotte Maxeke Johannesburg Academic Hospital, School of Clinical Medicine, Department of Otolaryngology, University of the Witwatersrand, Johannesburg, South Africa. Orcid Number: 0000-0002-2118-2400
IIMBBCh, DpPEC(SA), MMed, FCS(SA) Urol aadam81@gmail.com Postal: 7th York Road, Medical School, 9th Floor, Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, Parktown, 2193, South Africa. Division of Urology, School of Clinical Medicine, Faculty of Health Sciences, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa. Orcid Number: 0000-0001-9069-3282
ABSTRACT
INTRODUCTION: Lithiasis is the formation of stones within an organ, which can occur in multiple organs. Several studies have reported the possible concurrent occurrence of uroliths and sialoliths, possibly associated with shared comorbidities.
AIMS AND OBJECTIVES: This systematic review was conducted to review published research and identify the concurrent presence of uroliths and sialoliths. The review will describe diagnostic modalities, management, and prevention and suggest future research and clinical recommendations.
DESIGN AND METHODS: The following electronic databases were searched: PubMed, Scopus, Embase, Web of Science, and Google Scholar, using the Medical Subject Headings (Mesh terms), related to the primary disease processes relevant to the review.
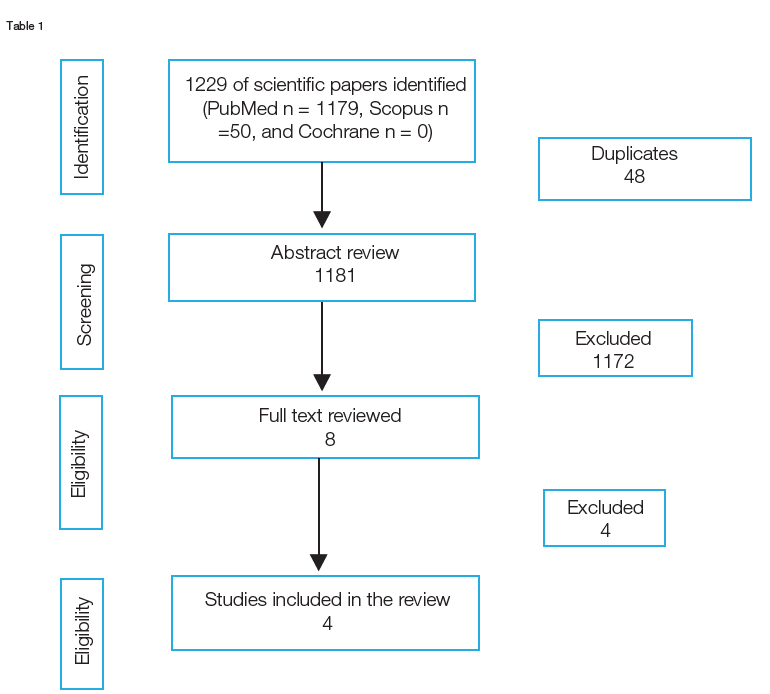
RESULTS: The database search yielded 1229 research papers. The articles were screened for duplicates, and unrelated studies were removed. The remaining four articles were reviewed by independent researchers and included in this review. Two of the four studies included in the review were case-control studies, and two were retrospective studies.
CONCLUSIONS: We found no evidence of a link between sialoliths and uroliths. However, the published literature's inconsistency posed a limitation.
Keywords: Salivary gland calculus; urolithiases; lithiasis; sialolithiasis; submandibular gland
INTRODUCTION
Lithiasis is the formation of stones composed of organic and inorganic material within an organ and can occur in multiple organs. Stones predominantly manifest in organs such as the kidney (nephrolith), bladder (cystolith), gallbladder (cholelith), bile duct (choledocholith), and salivary glands (sialolith) and typically result in obstructive or inflammatory effects within these organs if not surgically removed.1 According to conservative estimates, the incidence of lithiasis has been reported to reach 23 750 cases per 100,000 individuals in the United States alone, accounting for a burden of approximately $270 billion on their healthcare system.1
Sialoliths refer specifically to calculi formed within the salivary glands, with most cases (approximately 80 - 85%) affecting the submandibular gland.2 Recent studies have estimated the incidence of sialoliths to be between 1:15 000 to 1:30 000 persons or 2.9-5.5 cases per 100 000, with most cases seen in people between the ages of 30 to 50.2,3 Patients suffering from sialoliths may present with pain and swelling of the affected gland and, without surgical intervention, may experience complications such as sialadenitis.3
Deemed as one of the most common urologic diseases, urolithiasis is reported to affect up to 15% of people globally, with incidence increasing annually.4 In 2019, the Global Burden of Disease study reported a record of 115 million incident cases over 204 countries and 21 regions across the globe, with Southern Sub-Saharan Africa recording 546 100 cases. Of these global cases, 13 2 789 mortalities occurred, these figures demonstrate a 7% increase in just under two decades.5 Worldwide, the incidence is higher in males than females and higher between the age groups of 50 and 60 years.5
Several studies have reported the possible concurrent occurrence of uroliths and sialoliths,6 possibly because of shared comorbidities.4 In a study done by Hemminki et al.4 a link between sialolithiasis, urolithiasis and cholelithiasis was assessed. An assessment of familial and spouse risks between the three and comparing familial risks for concordant stone diseases were done. The familial risks between stone diseases were low but higher than those between spouses. Familial risks between stone diseases were also modest and they were not significant between sialolithiasis and urolithiasis, for which the stone composition is similar.
The data showed that familial clustering is unique to each stone disease, which implied distinct disease mechanisms. The data also showed higher familial risks for concordant stone formation than between spouses. These results questioned the reported excessive comorbidities between the three stone formations..4
The composition of sialoliths has been extensively researched in an attempt to identify aetiological factors and correlations with other diseases related to stone formation.7 However, correlation with other diseases related to stone formation was hard to establish.8 Most of the studies also emphasised the biochemical composition of sialoliths instead of the disease processes that may predispose to stone formation. Nonetheless, salivary stones are often found in the submandibular duct (72-95%), and of these, 57% and 34% are found in the hilum and distal duct, respectively.6 Sialoliths are seen less frequently in the parotid duct (4-28%), and of these, 23% are found in the parenchyma, while 13% and 64% are found in the hilum and distal duct, respectively.9 Contrasting from yellow to a yellow-brown colour, sialoliths consist of an amorphous mineralised core that is surrounded by concentric, laminated layers of organic or inorganic material identified through a scanning electron microscope.10 A study by Kraaij11 et al. showed that carbonate apatite was identified in 99% of sialoliths, while phosphate in 88%, calcium in 87%, magnesium in 68%, struvite in 44%, oxalate in 38% and carbonate in 35% as identified by wet chemical analysis. Other studies show an ultrastructural composition of mainly hydroxyapatite (Ca5(PO4)3OH), along with other trace minerals such as magnesium, sodium and chloride.7 Furthermore, sialoliths have an average weight of 300 mg, with the larger stones found more within the submandibular gland.12 More than half of the stones have a diameter between 2.1 mm and 10 mm, 88% being less than 10mm, whereas 7.6% of the stones are larger than 15 mm, with stones less than 5 mm being impalpable.13,14 Giant sialoliths are considered to be more than 15 mm in any dimension or weigh more than 1 gram, which is rare.13 The weights of the stones correlate significantly with age, demonstrating a direct proportion with increasing age.11
Uroliths is the most common form of stony concretions in the body; and is considered a chronic systemic condition which may recur within 5 to 10 years from the initial diagnosis within more than 50% of patients.15 Therefore, it is necessary to understand the etiopathogenesis that results in the formation of these stones. Various factors such as lifestyle, obesity, dietary habits, and dehydration have been implicated in the development of renal calculi and hormonal changes, genetic conditions, and anatomical variations may influence their pathogenesis.16 Nephroliths consist primarily of calcium oxalate, calcium phosphate and struvite, with calcium and phosphorus elements predominating.
Because of the possible correlation between urolithiasis and sialolithiasis, this systematic review was conducted to critically appraise published research and identify the concurrent presence of uroliths and sialoliths.
MATERIALS AND METHODS SEARCH STRATEGY
After PROSPERO registration was completed, the following electronic databases were searched: PubMed, Scopus, Embase, Web of Science and Google Scholar, utilising a search strategy developed with the Medical Subject Headings (Mesh terms) from PubMed related to the main disease processes relevant to the review. With regards to urolithiasis, the terms used included "Urolithiasis", "Nephrolithiasis", "Kidney Calculi", "Ureterolithiasis", "Ureteral Calculi", "Urinary Calculi". With regards to sialolithiasis, the terms used included "Sialolithiasis", "Salivary Gland Calculi", "Salivary Calculi", and "Salivary Duct Calculi". A term/s related to urolithiasis and a term/s related to sialolithiasis were combined using and/or to refine the search.
The inclusion criteria for the reviewed studies required full text publications in English, related only to the human species, and provided exposure to health conditions of both uroliths and sialoliths. Studies were pooled and screened, eventually narrowing the number of eligible studies to four papers that reached full-text review.
The Critical Appraisal Skills Programme (2018) Oxford Checklist was used to determine the quality of the studies appraised.
RESULTS
The database search yielded 1229 research papers. The articles were screened, and 48 duplicates and 1172 unrelated studies were removed. The remaining four articles were reviewed by independent researchers and included in this review. (Table 1) Two of the four studies included in the review were case-control studies, and the remaining two were retrospective studies.4,8,17,18 All the included studies were published in English within the last 10 years.
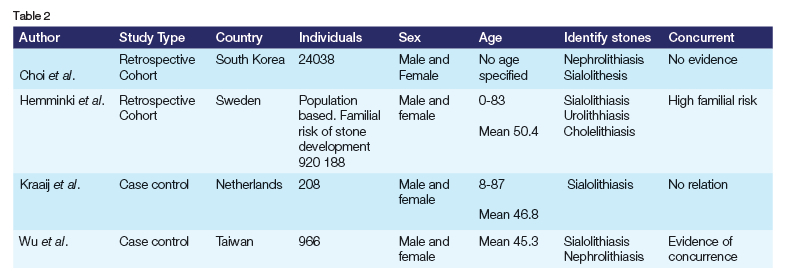
A total of 195 969 participants were included in the systematic review. The number of participants in the reviewed articles varied in size, the smallest being 208 and the largest 920 188 participants.4,17 Relevant studies were conducted in Sweden (920 188), Taiwan (966), South Korea (24038) and the Netherlands (208). Three studies recorded the sex of the patients, with Hemminki4 et al. being the only study without the definitive number of each sex. Participants of all ages were included, with the average age being 45 to 50 years old. However, Choi18 et al. excluded participants under the age of 18. (Table 2)
DISCUSSION
Urolithiasis has been extensively researched, and several correlations have been drawn between stone formation, systemic disease and genetic predisposition. In comparison, there is little to no research on the contributing factors to sialolithiasis. Sialoliths and uroliths have a similar composition. By investigating a possible correlation between uroliths and sialoliths, our better understanding of uroliths may be extrapolated to sialolith development and associated risk factors. Our systematic review aimed to identify the concurrent presence of uroliths and sialoliths to describe diagnostic modalities, management, and prevention and to make subsequent research and future clinical recommendations. Analysis of the available literature found no correlation between sialolithiasis and urolithiasis.
A study conducted by Choi18 et al. stated that the cause of nephroliths determines the composition of the stone. Calcium-containing stones are caused by hyperuricosuria,19 while uric acid and cystinuria are the most prevalent causes of non-calcium containing stones. Whereas causes of sialoliths range from lifestyle factors such as tobacco smoking to salivary duct trauma and chronic infection of the oral cavity.20 Another critical difference is that sialoliths are more likely to be caused by local factors such as the salivary gland ductal system or the content of saliva, in comparison to nephrolithiasis, which is said to be more likely as a result of systemic disease or medication.
Koch21 et al. provided a theory that decreased salivary flow and chronic obstructive sialadenitis are the leading causes of sialolith formation; however, unlike in nephrolithiasis, no study has found a direct correlation between systemic factors such as calcium metabolism contributing to salivary gland calculi.22
Kraaij17 et al. (2015) found no relationship between salivary stone formation and most systemic diseases. The study showed that the prevalence of nephrolithiasis in the patient group did not differ from that in the control group, suggesting that the risk factors for developing a sialolith and urolith were unrelated. The data also indicated that systemic diseases and the use of medication did not play a prominent role in the development of sialoliths, which suggests that local factors, such as anatomic variations of the salivary ducts, altered biochemical composition of saliva, or both are probably more critical factors in the development of salivary stones.17
Three of the four papers included in this review showed no association between urolithiasis and sialolithiasis. However, Wu8. et al. found a significant association between sialolithiasis and urolithiasis in the Taiwanese population. Reasons for this association may include ethnic differences and surveillance bias. There is well known variation among ethnic groups regarding the prevalence of urolithiasis, with diet and lifestyle, as well as genetic factors playing a role in predisposition to calculi formation.23 In addition, there is a risk of surveillance bias. The patient is already closely monitored within the healthcare system due to their primary disease; consequently, detecting other conditions is more likely. In this case, sialolithiasis is commonly an asymptomatic condition; most people may go undetected if not for regular visits to healthcare facilities and routine checks. Consequently, detecting sialolithiasis in these patients may have been incidental rather than an association. This is supported by the findings of Choi18 et al. (2018), in which the number of participants diagnosed with sialolithiasis in the control group (0.1%, 92/96,152, P = 0.447) was larger than the experimental group who had a history of urolithiasis (0.08% (19/ 24 038).
The sparse amount of literature pertaining to the link between sialolithiasis and nephrolithiasis contributes to the study's strengths. Though few studies support a lack of correlation, the large sample sizes can be seen as reliable. There is a great amount of literature on sialolithiasis and nephrolithiasis as individual entities. However, limited research is found when looking at the two in a combined matter. Therefore, the biggest limitation is that there were only an estimated four papers that could be analysed for the study.
Additionally, inconsistency in the studies analysed posed an additional limitation. These limitations show the importance of this study being conducted, as it will serve a bridge between the lack of literature available. Thus, to confidently determine a correlation and not a coincidence between sialolithiasis and nephrolithiasis, more literature should focus on the link between the two and not only on the individual aspects.
CONCLUSION
We found there to be no evidence between sialoliths and uroliths. Stones most commonly manifest in organs such as the kidney (urolithiasis) and salivary glands (sialolithiasis), thus supporting evidence of coincidence rather than correlation. The aetiology of sialoliths is found to be multifactorial. However, similarities with the hyperoxaluria that forms kidney stones have been suggested, but research remains sparse. It is for this reason that further investigations into the common aetiology could change the way in which lithiasis is identified, treated and prevented.
REFERENCES
1. Busso CS, Guidry JJ, Gonzalez JJ, Zorba V, Son LS, Winsauer PJ, et al. A comprehensive analysis of sialolith proteins and the clinical implications. Clin Proteom [Internet]. 2020 Mar 31;17(1). Available from: http://dx.doi.org/10.1186/s12014-020-09275-w [ Links ]
2. Tretiakow D, Skorek A, Ryl J, Wysocka J, Darowicki K. Ultrastructural analysis of the submandibular sialoliths: Raman spectroscopy and electron back-scatter studies. Ultrastructural Pathology [Internet]. 2020 Mar 3;44(2):219-26. Available from: http://dx.doi.org/10.1080/01913123.2020.1744784 [ Links ]
3. Kao WK, Chole RA, Ogden MA. Evidence of a microbial etiology for sialoliths. Laryngoscope [Internet]. 2019 Mar 12;130(1):69-74. Available from: http://dx.doi.org/10.1002/lary.27860 [ Links ]
4. Hemminki K, Hemminki O, Koskinen AIM, Försti A, Sundquist K, Sundquist J, et al. Familial risks in and between stone diseases: sialolithiasis, urolithiasis and cholelithiasis in the population of Sweden. BMC Nephrol [Internet]. 2018 Jul 3;19(1). Available from: http://dx.doi.org/10.1186/s12882-018-0945-y [ Links ]
5. Lang J, Narendrula A, El-Zawahry A, Sindhwani P, Ekwenna O. Global Trends in Incidence and Burden of Urolithiasis from 1990 to 2019: An Analysis of Global Burden of Disease Study Data. Eur Urol Open Sci [Internet]. 2022 Jan;35:37-46. Available from: http://dx.doi.org/10.1016/j.euros.2021.10.008 [ Links ]
6. Kraaij S, Karagozoglu KH, Forouzanfar T, Veerman ECI, Brand HS. Salivary stones: symptoms, aetiology, biochemical composition and treatment. Br Dent J [Internet]. 2014 Dec;217(11):E23-E23. Available from: http://dx.doi.org/10.1038/sj.bdj.2014.1054 [ Links ]
7. Rakesh N, Bhoomareddy Kantharaj YD, Agarwal M, Agarwal K. Ultrastructural and elemental analysis of sialoliths and their comparison with nephroliths. J Investig Clin Dent [Internet]. 2014 Feb;5(1):32-7. Available from: http://dx.doi.org/10.1111/j.2041-1626.2012.00157.x [ Links ]
8. Wu CC, Hung SH, Lin HC, Lee CZ, Lee HC, Chung SD. Sialolithiasis is associated with nephrolithiasis: a case-control study. Acta Otolaryngol [Internet]. 2016 Jan 25;136(5):497-500. Available from: http://dx.doi.org/10.3109/00016489.2015.1129068 [ Links ]
9. Zenk J, Constantinidis J, Kydles S, Hornung J, Iro H. Klinische und diagnostische Befunde bei der Sialolithiasis. HNO [Internet]. 1999 Nov 23;47(11):963-9. Available from: http://dx.doi.org/10.1007/s001060050476 [ Links ]
10. Kodaka T, Debari K, Sano T, Yamada M. Scanning electron microscopy and energy-dispersive X-ray microanalysis studies of several human calculi containing calcium phosphate crystals. Scanning Microsc. 1994;8(2):241-257. [ Links ]
11. Kraaij S, Brand H, van der Meij E, de Visscher J. Biochemical composition of salivary stones in relation to stone- and patient-related factors. Med Oral Patol Oral Cir Bucal [Internet]. 2018;0-0. Available from: http://dx.doi.org/10.4317/medoral.22533 [ Links ]
12. Harrill JA, King JS, Boyce WH. Structure and composition of salivary calculi. Laryngoscope [Internet]. 1959 May;69(5):481-92. Available from: http://dx.doi.org/10.1288/00005537-195905000-00001 [ Links ]
13. Bodner L. Giant salivary gland calculi: Diagnostic imaging and surgical management. Oral Surg Oral Med Oral Pathol Oral Radiol [Internet]. 2002 Sep;94(3):320-3. Available from: http://dx.doi.org/10.1067/moe.2002.123863 [ Links ]
14. Zenk J, Koch M, Klintworth N, König B, Konz K, Gillespie MB, et al. Sialendoscopy in the Diagnosis and Treatment of Sialolithiasis. Otolaryngol Head Neck Surg [Internet]. 2012 Jun 29;147(5):858-63. Available from: http://dx.doi.org/10.1177/0194599812452837 [ Links ]
15. Morgan MSC, Pearle MS. Medical management of renal stones. BMJ [Internet]. 2016 Mar 14;i52. Available from: http://dx.doi.org/10.1136/bmj.i52 [ Links ]
16. Yasui T, Okada A, Hamamoto S, Ando R, Taguchi K, Tozawa K, et al. Pathophysiology? based treatment of urolithiasis. Int J Urol [Internet]. 2016 Aug 18;24(1):32-8. Available from: http://dx.doi.org/10.1111/iju.13187 [ Links ]
17. Kraaij S, Karagozoglu KH, Kenter YAG, Pijpe J, Gilijamse M, Brand HS. Systemic diseases and the risk of developing salivary stones: a case control study. Oral Surg Oral Med Oral Pathol Oral Radiol [Internet]. 2015 May;119(5):539-43. Available from: http://dx.doi.org/10.1016/j.oooo.2015.01.010 [ Links ]
18. Choi HG, Bang W, Park B, Sim S, Tae K, Song CM. Lack of evidence that nephrolithiasis increases the risk of sialolithiasis: A longitudinal follow-up study using a national sample cohort. Gupta V, editor. PLOS ONE [Internet]. 2018 Apr 26;13(4):e0196659. Available from: http://dx.doi.org/10.1371/journal.pone.0196659 [ Links ]
19. Pak CYC. Etiology and Treatment of Urolithiasis. Am J Kidney Dis [Internet]. 1991 Dec;18(6):624-37. Available from: http://dx.doi.org/10.1016/s0272-6386(12)80602-0 [ Links ]
20. Hung S, Huang H, Lee H, Ching Lin H, Kao L, Wu C. A populationEbased study on the association between chronic periodontitis and sialolithiasis. Laryngoscope [Internet]. 2016 Jan 25;126(4):847-50. Available from: http://dx.doi.org/10.1002/lary.25360 [ Links ]
21. Koch M, Zenk J, Bozzato A, Bumm K, Iro H. Sialoscopy in Cases of Unclear Swelling of the Major Salivary Glands. Otolaryngol Head Neck Surg [Internet]. 2005 Dec;133(6):863-8. Available from: http://dx.doi.org/10.1016/j.otohns.2005.08.005 [ Links ]
22. Waseem BAZ, Forte V. An unusual case of bilateral submandibular sialolithiasis in a young female patient. Int J Pediatr Otorhinolaryngol [Internet]. 2005 May;69(5):691-4. Available from: http://dx.doi.org/10.1016/j.ijporl.2004.11.015 [ Links ]
23. Cook J, Lamb BW, Lettin JE, Graham SJ. The Epidemiology of Urolithiasis in an Ethnically Diverse Population Living in The Same Area. Urol J [Internet]. 2016 Aug. 25 [cited 2024 Aug. 27];13(4):2754-8. Available from: https://ojs3.sbmu.ac.ir/urolj/index.php/uj/article/view/3336 [ Links ]
 Correspondence:
Correspondence:
Name: Prof. S. Maharaj
Email: shivesh.maharaj@wits.ac.za
Tel: +27 1714299
Contributions
Prof. S. Maharaj: Principal Researcher and editing - 50% Prof. Ahmed Adam: Writing Article 50%
Acknowledgements
Glory Amadi-Ihunwo, Gabriela Bartolo, Khatijah Bayat, Olivia Currie, Pallo Madisha, Kumaran
Disclosure
The authors declare no conflicts of interest and have no funding to disclose.

{kind=link}
{kind=link}