










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.80 n.2 Johannesburg Mar. 2025
https://doi.org/10.17159/sadj.v80i02.20196
SYSTEMATIC REVIEW
Comparability of the single-item Visual Analog Scale (VAS-A) to the multi-item Modified Dental Anxiety Scale (MDAS) - A systematic review and meta-analysis
ML MacheteI; TK MadibaII; PD MotlobaIII
IBDS (UL), MDS (SMU), Registrar (MDent), Department of Community Dentistry, School of Dentistry, Sefako Makgatho Health Sciences University (SMU), Ga-Rankuwa, South Africa.ORCID: 0000-0002-0218-8428
IIB.Dent Ther, BDS, DHSM, MChD (Community Dentistry), Department of Community Dentistry, School of Dentistry, University of Pretoria, Pretoria, South Africa. ORCID: 0000-0002-0171-0595
IIIMDent (Comm Dent) (Medunsa), MBL (Unisa), Head, Department of Community Dentistry, School of Dentistry, Sefako Makgatho Health Sciences University (SMU), Ga-Rankuwa, South Africa. ORCID: 0000-0003-1379-7576
ABSTRACT
BACKGROUND: Anxiety is associated with delayed dental attendance and treatment, leading to worsened intra-operative experiences for patients and clinicians. Ultimately, clinicians must reliably evaluate and manage dental anxiety to improve patient compliance and overall oral health status.
AIM: The purpose of this study was to estimate the reliability of the visual analog scale for anxiety (VAS-A) compared to the modified dental anxiety scale (MDAS).
METHODOLOGY: This systematic review and meta-analysis was conducted according to PRISMA guidelines. Comprehensive Meta-Analysis (CMA) 4.0 software was used to analyse data from 17 included studies.
RESULTS: The random effects model was selected due to high heterogeneity, yielding a correlation of 0.730 (95% CI: 0.615-0.815) between VAS-A and MDAS.
CONCLUSION: A high correlation between VAS-A and MDAS confirms the reliability of the tool. Given its simplicity and ease of use, the VAS-A should be incorporated in routine assessment of dental anxiety in dental settings.
Keywords: Dental anxiety, reliability, VAS, MDAS
INTRODUCTION
Understanding the vicious cycle of dental anxiety and phobia is critical for clinicians in ensuring better outcomes for their patients. Fearful patients often delay or avoid dental visits, which seriously impacts their oral health.1-3 This cycle of missed appointments, poor oral health, intense pain and invasive dental care only deepens dental anxiety and phobia.4-5 Dental anxiety is most prevalent among adults, ranging between 10.0% and 29.3% depending on the outcome measured.6-8 The primary step towards an adequate and effective management of dental anxiety, fear or phobia should include an accurate evaluation of the problem using proper screening tools. It is therefore important for clinicians to accurately assess patient's anxiety and its triggers, using a reliable and validated instrument. The visual analog scale for anxiety (VAS-A), Corah's Dental Anxiety Scale (DAS) and recently the Modified Dental Anxiety Scale (MDAS) and State-Trait Anxiety Inventory (STAI) are among the widely used tools to assess dental anxiety in the dental setting.9-12 Despite its well-established validity, the use of VAS-A has reduced significantly since its introduction in 1988.13-4 The decline in the use of VAS-A is attributed to its perceived low reliability compared to MDAS. The unfavourable comparative reliability of the VAS-A can be ascribed to methodological inadequacies such as the study characteristics and, specifically, the low sample size. While the VAS-A is easy to use and understand, its sensitivity and reliability have not been quantified. Therefore, the consistency of VAS-A in assessing dental anxiety remains questionable.15 Hence this meta-analysis aims to assess the reliability of the VAS-A by aggregating the findings from similar studies.
MATERIAL AND METHODS
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.16
Review question
The following review question formed the basis of this systematic review and meta-analysis. How does the single-item Visual Analog Scale-Anxiety (VAS-A) compare with the multi-item Modified Dental Anxiety Scale (MDAS) in assessing dental anxiety? In other words, how reliable is the VAS-A as a measure of anxiety in the dental setting compared with the MDAS?
Eligibility criteria
All observational studies reporting the correlation of VAS-A and MDAS or data that could permit the computation of the correlation of VAS-A and MDAS were considered for inclusion. Other criteria included the following: (i) Patients in a dental clinic setting, irrespective of the procedure undertaken. (ii) Participants aged 18 years or older. (iii) Studies with incomplete data were excluded.
Search strategy
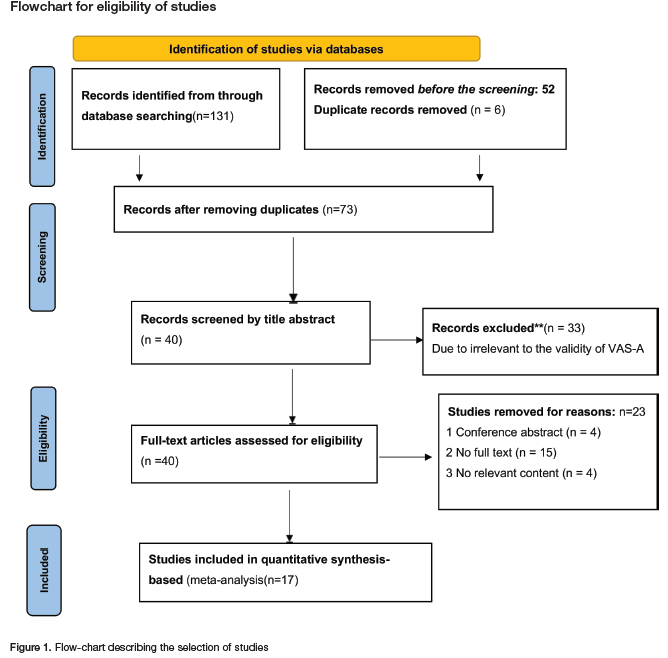
A comprehensive electronic search for literature was conducted in PubMed, Scopus Google Scholar and MEDLINE Ultimate, using the relevant MeSH terms. The search was restricted to English language articles and publications from 1988 to June 2024. The specific search strategies for each database are presented in Figure 1.
Inclusion and exclusion of studies
Two reviewers (LMM and DPM) independently screened titles and abstracts; in case of disagreement the third reviewer (TM) was engaged to resolve the dispute through discussion. LMM and DPM also read the full-text articles for inclusion or exclusion based on the established eligibility criteria. Details of the excluded and reasons are depicted in Figure 1. Additional hand search and review of references was done to broaden the pool of included studies.
Data collection
LMM and DPM independently abstracted data from eligible studies using a predefined form. The tool recorded the following variables: author details, study design, sample characteristics (mean age), country, sample size and correlation coefficients (VAS-A and MDAS). Disagreements in data collection were resolved by the third reviewer. In case of missing or incomplete data, authors would be contacted to provide clarity.
Quality assessment of included studies
The methodological quality assessment of the included studies was performed using the adapted Newcastle-Ottawa Quality Assessment Scale for correlational studies.17 This instrument assessed eight (8) study design factors using the options "yes", "no" or "unclear". The study characteristics included representativeness of the sample, study setting, sample size, data collection and measurements, and statistical analysis. Studies were rated as high or low risk of bias with scores <4 and >4 respectively. LMM and DPM independently assessed the quality of the included study, and disagreements were resolved through discussion.
Statistical analysis
Comprehensive Meta-Analysis (CMA) 4.0. was used in data analysis for this study. The Pearson correlation coefficient for each study was used to estimate the overall correlation. This software permits Fisher's r-to-z transformation in the computation of the standardised effect sizes for each correlation coefficient. This transformation normalises the distribution of the correlation which increases the accuracy of the estimate of correlation. The pooled estimates of correlation were calculated using both the fixed-effect and random-effect models. However, the reported model was the random-effects model, due to observed differences in study characteristics, as well as the computed statistical heterogeneity (I2>50%). Subgroup analysis was conducted to investigate the effects of the study and methodological characteristics on summary estimates. Additional sensitivity analysis was conducted to assess the effects of each study on correlation estimates. The assessment of publication bias was evaluated visually from the funnel plot and confirmed from the statistical tests (Egger's test).
RESULTS
Study selection
The search generated 131 articles from which 58 duplicates were removed. The abstracts of 73 articles were screened, resulting in the exclusion of 40 papers. Seventeen studies met the inclusion criteria for this meta-analysis. Figure 1 depicts the PRISMA flowchart for this study. The screening accuracy between the two reviewers resulted in a 95% agreement rate initially and increased to 100% after discussion with a third reviewer.
Characteristics of included studies
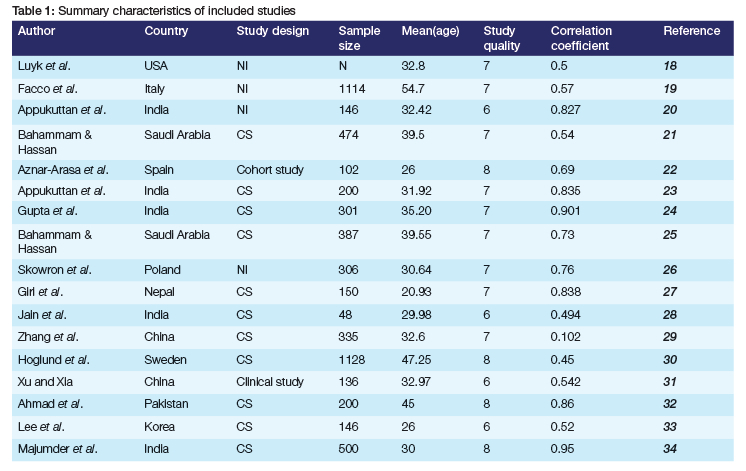
This meta-analysis included 17 studies (k=17, n=5787) from 11 countries, published between 1988 and 2023. The average sample size for the included studies was 336.12, ranging from 43 to 1128. The majority of studies, 12 (70.58%), were from Asia, represented by India and China. Table 1 shows detailed characteristics of the included studies,18-34 including quality assessment scores.
The correlation between VAS-A and MDAS
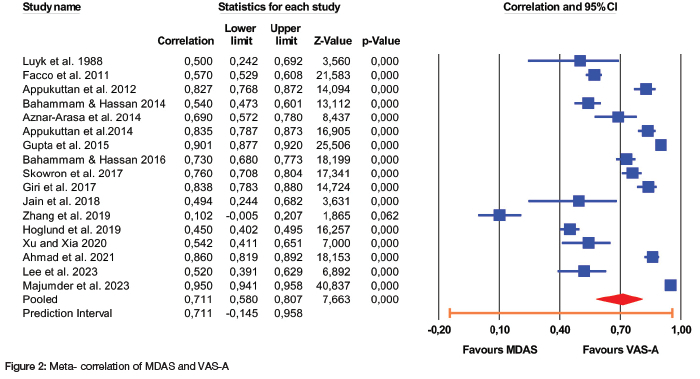
The correlation coefficient between VAS-A and MDAS was 0.711 (95% CI: 0.580-0.807), based on the random effects model, as shown in Figure 2. The Q test revealed the presence of heterogeneity in the included studies [Q (16) =1138.50; p<0.000; tau2=2.23; I2=98.595]. Based on the prediction interval (PI), the true effect size in 95% of all comparable populations lies between -0.145 and 0.958.
Subgroup analysis and meta-regression
The subgroup analysis included the following moderating variables: (i) country, which was dichotomised as Asian countries and others, and (ii) sample size, divided into two groups (<300 and >300). The correlation coefficient between VAS-A and MDAS was 0.678 (95%CI: 0.523, 0.834) among the Asian studies and 0.664 (95%CI: 0.507, 0.821) in others, p=0.905. Similar, insignificant correlation was found for smaller versus large studies 0.678 (95%CI: 0.553, 0.804) vs 0.669 (95%CI: 0.443, 0.895), p=0.932. Meta-regression was not done due to insignificant predictors.
Publication bias
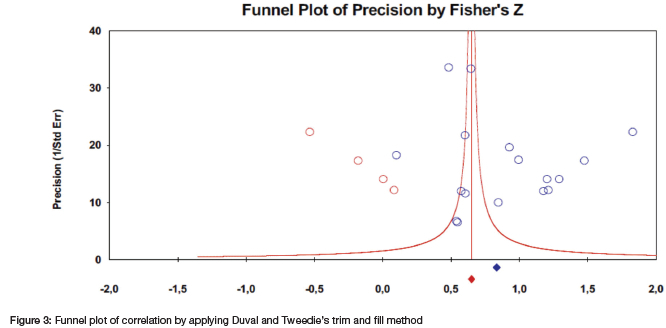
Publication bias was assessed visually using funnel plots and Duval and Tweedie's trim and fill method. Egger's test provided the statistical measure to confirm the presence of publication bias. The funnel plot indicated a preponderance of small studies to the left of the point estimate. This asymmetry could suggest publication bias (Figure 3). Similarly, the trim and fill procedure showed evidence of imbalance (evidence of missing studies) as indicated by differences in effect size estimates between the observed and adjusted values (Figure 3). However, Egger's test (t=0.876, p = 0.394) indicated that there was no obvious publication bias in this study.
Sensitivity and meta-regression analysis
Sensitivity analyses are used to evaluate the robustness of the meta-analysis in the estimation of the effect size. In this study the following analyses were undertaken: (i) one study removed, which is the sequential exclusion of a single study from the analysis; (ii) determining the effects of study weights in the computation of mean correlation (relative weights) and (iii) conducting cumulative meta-analysis. After excluding one study at a time, the correlation coefficients ranged between 0.681 and 0.736, which is materially and significantly similar to the mean effect size of 0.711. Similarly, the relative weights of included studies ranged between 5.47% and 6.03%. The cumulative meta-analysis showed an increase in correlation coefficients, from r=0.500 in 1998 to 0.711 in 2023, which indicates the increasing robustness of correlation estimates over time. Meta-regression analysis was not done due to statistically insignificant predictors.
Ethical consideration
No ethics clearance is required for this study, which does not involve human participants. This systematic review uses secondary data sourced from published literature.
DISCUSSION
Interpretation of the effect size estimate
This systematic review and meta-analysis found a substantial positive correlation between the visual analog scale for anxiety (VAS-A) and the modified dental anxiety scale (MDAS). The robustness of this pooled estimate is predicated by the rigorous methodologies employed in addressing the following questions: First, is it proper to compare the numeric VAS-A to the ordinal (5 Likert scale) MDAS? In other words, is the estimated correlation between these variables appropriate? Stated differently, can ordinal variables be treated as numeric variables in the computation of correlation? Literature indicates that it is defensible to treat ordinal data as continuous variables, especially when the variable has more categories.35 In this case, the MDAS is measured on a 5-point Lickert scale, which is sufficient. Additionally, Majumder et al34 and Hoglund et al30 found the computation of correlation between VAS-A and MDAS to be appropriate despite the differences in the measurement scales. These results establish the basis for comparing these scales as "apples and apples".
The second question sought to determine whether the estimation of the effect size was reliable and valid. In other words, can we show that the effects of bias and heterogeneity on the pooled estimate are not large enough to render the findings invalid? Robust statistical analyses were employed to assess the effects of these threats on the effect size. The visual tests, subgroup analyses and meta-regression demonstrated the absence of publication bias and lack of evidence of heterogeneity. Despite the observed high heterogeneity (I2=99.00), we can conclude that the pooled estimate in this meta-analysis is robust and justifiable.
Implications of the findings
Patients with higher levels of dental anxiety demonstrate a lower pain tolerance compared to those with lower levels of anxiety.36 The increased levels of anxiety correlate with increased attentiveness to environmental threats and perceived pain. Consequently, anxious patients are difficult to manage and treat in dental practices. Therefore, detecting and measuring the levels of anxiety is critical in its management, which, in turn, will be beneficial to ensuring a pleasant dental experience for the patient and clinician. Currently, the reliable and validated tool to measure dental anxiety is self-questionnaires. Although VAS-A is widely used in medicine to measure levels of pain, anxiety and other psychological states, the routine use of VAS-A has stalled. Instead, the use of MDAS has increased exponentially, especially in clinical research. The VAS-A is quick, easy and convenient to administer, especially for busy practitioners.
This study sought to establish the reliability of VAS-A as a tool to assess dental anxiety. Several publications have questioned the reliability of VAS-A due to underpowered studies, hence its infrequent use in clinical practice or research.22-3,27-8 There is currently no systematic review or meta-analysis evaluating the reliability of VAS-A. This meta-analysis is probably the first to synthesise existing data, thereby demonstrating the comparative reliability of the VAS-A as a tool to evaluate dental anxiety. Additionally, the VAS-A is flexible in assessing overall levels of patient's anxiety, without being confined to the predefined categories or clinical scenarios. Like classic VAS, the validity and usefulness of this tool is well established, and this study has provided evidence of its reliability.
Study limitations
Most of the included studies did not measure item-to-item correlations.30-3 Consequently, the findings of this study are applicable as estimates of the overall reliability measure and not the specific item-to-item correlation. The other limitation is the overrepresentation of Asian studies, which could bias the results. The impact of factors such as age, gender and history of dental visits on dental anxiety was not assessed in these studies. These predictors may affect the estimation of anxiety levels and correlation.
CONCLUSION
The VAS-A is a reliable and practical instrument for assessing overall anxiety in the dental setting. Based on the study findings, we recommend the routine use of VAS-A to measure the changing levels of dental anxiety.
REFERENCES
1. Berggren U, Meynert G. Dental fear and avoidance: Causes, symptoms, and consequences. JADA. 1984; 109:247-251. doi: 10.14219/jada.archive.1984.0328 [ Links ]
2. Winkler CH, Bjelopavlovic M, Lehmann KM, et al. Impact of Dental Anxiety on Dental Care Routine and Oral-Health-Related Quality of Life in a German Adult Population-A Cross-Sectional Study. J Clin Med.2023;12(16):5291. doi: 10.3390/jcm12165291 [ Links ]
3. Pohjola V, Rekola A, Kunttu K, Virtanen JI. Association between dental fear and oral health habits and treatment need among University students in Finland: A national study. BMC Oral Health.2016;16:26. doi: 10.1186/s12903-016-0179-y [ Links ]
4. Heidari E, Newton J, Banerjee A. Minimum intervention oral healthcare for people with dental phobia: a patient management pathway. BDJ.2020; 229:417-424. https://doi.org/10.1038/s41415-020-2178-2 [ Links ]
5. Yildirim TT. Evaluating the Relationship of Dental Fear with Dental Health Status and Awareness. J Clin Diagn Res. 2016 Jul;10(7):ZC105-9. doi 10.7860/JCDR/2016/19303.8214 [ Links ]
6. Cianetti S, Lombardo G, Lupatelli E, Pagano S, Abraha I, Montedori A, Salvato R. (2017). Dental fear/anxiety among children and adolescents. A systematic review. Eur J Paediatr Dent, 18(2), 121-30 [ Links ]
7. Silveira ER, Cademartori MG, Schuch HS, Armfield JA, Demarco FF. (2021). Estimated prevalence of dental fear in adults: A systematic review and meta-analysis. Journal of Dentistry, 108, 103632. https://doi.org/10.1016/j.jdent.2021.103632 [ Links ]
8. Murad MH, Ingle NA, Assery MK. Evaluating factors associated with fear and anxiety to dental treatment-A systematic review. J Family Med Prim Care. 2020 Sep 30;9(9):4530-4535. doi: 10.4103/jfrnpc.jfrnpc_607_20 [ Links ]
9. Facco E, Zanette G, Favero L, Bacci C, Sivolella S, Cavallin F, Manani G. Toward the validation of visual analog scale for anxiety. Anesth Prog. 2011 Spring;58(1):8-13. doi: 10.2344/0003-3006-58.1.8 [ Links ]
10. Newton JT, Buck DJ. Anxiety and pain measures in dentistry: a guide to their quality and application. JADA. 2000 Oct;131(10):1449-57. doi: 10.14219/jada.archive.2000.0056. PMID: 11042984 [ Links ]
11. Schuurs AH, Hoogstraten J. Appraisal of dental anxiety and fear questionnaires: a review. Community Dent Oral Epidemiol. 1993 Dec;21(6):329-39. doi: 10.1111/j.1600-0528. 1993.tb01095. x [ Links ]
12. Chi SI. What is the gold standard of the dental anxiety scale? J Dent Anesth Pain Med. 2023 Aug;23(4):193-212. doi: 10.17245/jdapm.2023.23.4.193 [ Links ]
13. Kindler CH, Harms C, Amsler F, et al. The visual analog scale allows effective measurement of preoperative anxiety and detection of patient's anesthetic concerns. Anesth Analg.2000; 90: 706-712 [ Links ]
14. Hosey MT, Blinkhorn AS. An evaluation of four methods of assessing the behaviour of anxious child dental patients. Int J Paediatr Dent. 1995;5(2):87-95. doi: 10.1111/j.1365-263x.1995.tb00170. x [ Links ]
15. Maxwell C. (1978). Sensitivity and accuracy of the visual analog scale: a psycho-physical classroom experiment. British journal of clinical pharmacology, 6(1), 15-24 [ Links ]
16. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of Internal Medicine.2009; 151(4): 264-269 [ Links ]
17. Moskalewicz A, Oremus M. No clear choice between Newcastle-Ottawa Scale and Appraisal Tool for Cross-Sectional Studies to assess methodological quality in cross-sectional studies of health-related quality of life and breast cancer. Journal of Clinical Epidemiology.2020; 120: 94-103 [ Links ]
18. Luyk NH, Beck FM, Weaver JM. A visual analogue scale in the assessment of dental anxiety. Anesthesia progress. 1988;35(3):121 [ Links ]
19. Facco E, Zanette G, Favero L, Bacci C, Sivolella S, Cavallin F, et al. Toward the validation of visual analogue scale for anxiety. Anesthesia progress. 2011;58(1):8-13. https://doi:10.2344/0003-3006-58.1.8 [ Links ]
20. Appukuttan D, Datchnamurthy M, Deborah SP, Hirudayaraj GJ, Tadepalli A, Victor DJ. Reliability and validity of the Tamil version of Modified Dental Anxiety Scale. Journal of Oral Science. 2012;54(4):313-20. https://doi.org/10.2334/josnusd.54.313 [ Links ]
21. Bahammam MA, Hassan MH. Validity and reliability of an Arabic version of the modified dental anxiety scale in Saudi adults. Saudi Med J. 2014;35(11):1384-9 [ Links ]
22. Aznar-Arasa L, Figueiredo R, Valmaseda-Castellón E, Gay-Escoda C. Patient anxiety and surgical difficulty in impacted lower third molar extractions: a prospective cohort study. Int J Oral Maxillofac Surg. 2014;43(9):1131-6. http://dx.doi.org/10.1016/j.ijom.2014.04.005 [ Links ]
23. Appukuttan D, Vinayagavel M, Tadepalli A. Utility and validity of a single-item visual analog scale for measuring dental anxiety in clinical practice. Journal of oral science. 2014;56(2):151-6. https://doi.org/10.2334/josnusd.56.151 [ Links ]
24. Gupta G, Shanbhag N, Puranik MP. Cross-Cultural Adaptation of Kannada Version of Modified Dental Anxiety Scale Among an Adult Indian Population. J Clin Diagn Res. 2015;9(9):Zc34-8. https://doi:10.7860/JCDR/2015/12675.6469 [ Links ]
25. Bahammam MA. Validity and reliability of an Arabic version of the state-trait anxiety inventory in a Saudi dental setting. Saudi Med J. 2016;37(6):668-74. https://doi:10.15537/smj.2016.6.13935 [ Links ]
26. Skowron MU, Nowak PG, Wisckiewicz W, Waliczek M. Utility of the visual analog scale for the assessment of dental anxiety. Dental and Medical Problems. 2017;54(4):389-95.https://doi:10.17219/dmp/78544 [ Links ]
27. Giri J, Pokharel PR, Gyawali R, Bhatttarai B. Translation and validation of modified dental anxiety scale: the Nepali version. International scholarly research notices. 2017;2017(1):5495643. https://doi.org/10.1155/2017/5495643 [ Links ]
28. Jain M, Tandon S, Sharma A, Jain V, Yadav NR. Cross-Cultural adaption, validity and reliability of a Hindi version of the Corah's Dental Anxiety Scale. Health promotion perspectives. 2018;8(2):120. https://doi:10.15171/hpp.2018.15 [ Links ]
29. Zhang X, Wang B, Qiao SC, Gu YX, Shi JY, Lai HC. A study on the prevalence of dental anxiety, pain perception, and their interrelationship in Chinese patients with oral implant surgery. Clinical implant dentistry and related research. 2019;21(3):428-35. https://doi.org/10.1111/cid.12779 [ Links ]
30. Höglund M, Bágesund M, Shahnavaz S, Wárdh I. Evaluation of the ability of dental clinicians to rate dental anxiety. European journal of oral sciences. 2019;127(5):455-61. https://doi.org/10.1111/eos.12648 [ Links ]
31. Xu JL, Xia R. Influence factors of dental anxiety in patients with impacted third molar extractions and its correlation with postoperative pain: a prospective study. Med Oral Patol Oral Cir Bucal. 2020;25(6):e714-e9. https://doi:10.4317/medoral.23293 [ Links ]
32. Ahmad S, Sana U, Haseeb M, Niazi I, Khan Z, Yousaf O. Relationship of dental anxiety and pain during inferior alveolar nerve block. Pakistan Journal of Medical and Health Sciences. 2021;15(7):1626-8. https://doi.org/10.53350/pjmhs211571626 [ Links ]
33. Lee E, Jee Y-J, Jung J, Lee MH, ok Hong S. Extraction of mandibular third molars: relationship of preoperative anxiety with body mass index, serum high-sensitivity C-reactive protein levels, and visual analog scale scores and predictors of postoperative complications. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2023;49(5):252. https://doi.org/10.5125/jkaoms.2023.49.5.252 [ Links ]
34. Majumder G, Das S, Bhattacharyya A, Mitra A, Maity AB. Evaluating the Reliability of the Visual Analogue Scale (VAS) in assessing dental anxiety in Bengali Population - A Cross-sectional Study [ Links ]
35. Robitzsch A. Why Ordinal Variables Can (Almost) Always Be Treated as Continuous Variables: Clarifying Assumptions of Robust Continuous and Ordinal Factor Analysis Estimation Methods. Frontiers in Education. 2020; 5:589965.doi:10.3389/feduc.2020.589965 [ Links ]
36. Michaelides A, Zis P. Depression, anxiety and acute pain: links and management challenges. Postgrad Med. 2019;131(7):438-444. doi: 10.1080/00325481.2019.1663705 [ Links ]
 Correspondence:
Correspondence:
Name: Motimedi L Machete
Email: lesley.machete@smu.ac.za
Author's contribution
Motimedi L Machete - principal author (45%)
Thomas K Madiba (15%)
Pagollang D Motloba (40%)

{kind=link}
{kind=link}
{kind=link}
{kind=link}