










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.80 n.3 Johannesburg Apr. 2025
ETHICS
Listening: The most valuable service you won't charge for!
LM SykesI; HT van den BerghII; P NethonondaIII; H BernitzIV
IBSc, BDS, MDent, Dip Research Ethics (IRENSA), Dip Forensic Odont, Dip ESMEA, FCD (Pros) Head of Department of Prosthodontics, University of Pretoria. Leanne.sykes@up.ac.za; Orcid: https://orcid.org/0000-0002-2002-6238
IIBChD, MSc. (Dent) Registrar
IIIBSc, BDS, PGDip (Clinical), MChD (Pros) Senior Lecturer Prosthodontics Department, University of Pretoria. Herman van den Bergh. Orcid: https://orcid.org/0000-0002-8571-818X; Portia Nethononda. Orcid: https://orcid.org/0009-0004-1978-0702
IVBChD, MSc, Dip Odont, PhD Extraordinary Professor, Department of Maxillo-facial Pathology, University of Pretoria
ABSTRACT
Dental practitioners cannot charge additional fees for the time spent "listening" to their patients, however, the non-financial cost benefits of this time spent may be of a far greater value than is generally realised. Consciously paying attention to a patient and engaging in meaningful communication with them play a valuable part in providing patient-centred care and fostering a positive healthcare experience. Time constraints and billing pressures are a reality in today's clinical practice. The art of listening to patients aligns with both ethical care and sustainable practice management. It's about balancing financial viability with compassionate patient care.
"Knowledge Speaks, but Wisdom Listens"
Jimi Hendricks
Introduction
Dental practitioners are not allowed to charge additional fees for the time spent "listening" to their patients. The fees they charge are for the services they provide, such as the consultation, examination and treatment planning, and the subsequent performance of clinical procedures. Time spent listening or talking to a patient falls under the general scope of the consultation visit, and is included in the overall fee for that appointment (*see Code 8101 and 8104 description).1 This brings up the question of whether we, as individuals, health care providers, or society, truly listen to one another, rather than merely observing at a surface level and forming opinions based on a superficial, and often subjective impression refered to as cognitive bias. While a practitioner cannot charge for added listening-time, the non-financial cost benefits may be of a far greater value. Listening and communicating well helps build trust, ensures accurate diagnoses, and leads to better outcomes.2 When patients feel heard, they are more likely to share important details about their symptoms, concerns, and medical history, which can lead to a more complete and accurate diagnosis.3
It also promotes a sense of respect and empathy, making patients feel valued and more likely to follow treatment plans. Overall, listening is key to providing patient-centred care and fostering a positive healthcare experience.4 The following case highlights the need for clinicians to spend time listening to their patients and sets the scene for the subsequent ethical discussion.
Case scenario
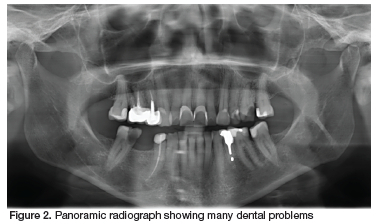
A patient presented to a new dentist seeking treatment. Before even taking the time to listen to her main complaint, establish her desires, or examine her mouth, the clinician began to discuss her "ugly front teeth", and the need to have all six anterior maxillary teeth crowned to give her a "beautiful smile" (Figure 1). The patient was rather disconcerted, as she had never been too worried about her smile, and was seeking relief from the severe pain she had been experiencing in the 4th quadrant. The dentist then decided it might be prudent to take a radiograph and investigate further. An orthopantomogram (Figure 2) revealed several dental problems, the most obvious being the large carious lesion on the 46. The patient was told that this tooth could be restored if she was willing to undergo a root canal therapy and pay for a seventh crown. If not it could be extracted immediately while the follow-up visits were being scheduled.

At this stage, the patient became anxious and psychoiogicaiiy distressed. Firstly, because she feit the clinician had not taken the time to talk to her, or listen to her presenting problem. She had sought treatment because she was in pain, yet this had not even been acknowledged. Furthermore, she had never considered her smile unattractive and was now feeling self-conscious and embarrassed at the thought that other people may have been commenting on her looks without her knowledge for many years. She felt so unnerved and upset, that she cut the visit short and left the rooms without having her main complaint, the pain, addressed.
Hearing versus Listening
Hearing can be defined as a passive physiological process of perceiving sound through the ears by a physical process of detecting sound waves and recognizing that noise is present. No active or conscious effort is required, as it happens automatically if the auditory system is functioning. Merely hearing something does not necessarily lead to understanding or retaining information without active input and engagement.
Listening is that active process of paying attention to, understanding, and interpreting the sounds or words that have been heard. It involves conscious effort to decode the unspoken messages, and construct meaning from what is being communicated. This requires mental focus, attention, interest, comprehension, engagement, and an emotional connection in order to understand and respond with empathy or action based on the information.2,4
The key distinction between the two is that hearing is passive and physiological, while listening is active, intentional, and cognitive. Effective communication requires listening, not just hearing, and involves attention, empathy, patience, openness, and comprehension, making it a critical skill in personal and professional communication.5
Key Elements of Listening and Communicating
Receiving: The physical act of hearing the sound or observing the nonverbal cues of the speaker.
Understanding: Making sense of the words, tone, and context of what is being communicated.
Evaluating: Judging the content, intent, and relevance of the message.
Responding: Providing verbal or nonverbal feedback to show comprehension and engagement.
Remembering: Retaining the information shared for future reference or action.
The phrase "I see you, but do I hear you?" is a powerful reflection on the distinction between acknowledgment and understanding in communication. It highlights the idea that truly hearing someone goes beyond the spoken word. It includes acknowledging their presence, noticing or observing their behaviour, engaging with them to try form a connection, and responding in a manner that shows you genuinely value what they have said. The seeing is about recognition, while the hearing relates to the connection and comprehension. This question also challenges whether we, as individuals or society, truly listen to one another, rather than merely observing at a surface level.
The Importance of Listening in a Healthcare setting A. Patient related factors
During the initial consultation, a practitioner must spend time engaging with their patients and listening attentively to their presenting complaints. This involves actively listening and hearing not just the words, but also the emotions and context behind what the patient is saying. It's not just about checking off symptoms, but about picking up on the nuances, concerns, and any underlying fears that might affect their well-being or their willingness to follow through with treatment. This in turn will help the healthcare provider understand the full picture of the patient's physical, emotional, and social state of health. Being genuinely present and attentive also builds trust, which can be especially important if patients are feeling vulnerable or scared about their condition, as-yet-unknown diagnosis and possible treatment options. At the same time listening to patients can be seen as an ethical and legal requirement as it shows the following:4,6,7
1. Respect for Autonomy:
Listening shows respect for a patient's right to make decisions about their own health and treatment. It ensures they can express their values, concerns, and preferences, which are crucial in shared decision-making.
2. Building Trust and Loyalty:
Active listening builds a foundation of trust between patients and caregivers. It is also crucial that they are honest when communicating with their patients, and this will encourage honesty, adherence to treatment, and better overall outcomes in return. They will also be more likely to return for all their future treatment needs, and recommend the practice to others
3. Empathy and Compassion:
Listening is an act of compassion that acknowledges the patient's feelings and experiences. It helps create a space where patients feel seen and understood, reducing feelings of isolation or fear. Furthermore, many patients feel anxious or vulnerable in dental consulting rooms. When you take the time to listen, it helps reduce those feelings and creates a safe environment for them.
4. Improved Quality of Care:
Patients often provide key details about their symptoms, history, or lifestyle that can guide better diagnosis and treatment. Ignoring them risks missing crucial information.
5. Advocacy and Equity:
Listening ensures that marginalized or vulnerable populations have their voices heard, preventing disparities in care and promoting ethical principles of justice and fairness.
6. Non-Maleficence:
Ignoring or dismissing a patient's concerns can lead to harm, whether through misdiagnosis, inappropriate treatment, or emotional distress. Listening actively minimizes such risks.
7. Informed Consent:
Engaging with patients ensures they understand their options, risks, and benefits, empowering them to make informed choices about their care.
In essence, listening is not only a cornerstone of ethical practice but also a critical tool for effective, patient-centred care.
B. Practitioner related factors
While it is not permissibie to charge fees for extra time spent listening to a patient, it is still absolutely worth the time in the long run. It can lead to:2,4,8
1. Improved Patient Outcomes
Listening can lead to a better understanding of symptoms, concerns, and underlying issues. Accurate diagnosis and treatment decisions are more likely, reducing follow-ups or complications that could take more time later.
2. Relationship Building
A strong patient-provider relationship fosters loyalty and satisfaction. Patients who feel heard are more likely to return, and to adhere to treatment plans, benefiting long-term success. They are also more likely to recommend you to family and friends, which is valuable for growing a practice and reputation.
3. Personal Professional Fulfilment
Listening is part of the human connection that makes healthcare meaningful. Taking the time to listen can provide personal satisfaction and remind a clinician why they chose this field.
4. Legal and Ethical Safeguards
Patients who feel unheard are more likely to pursue legal action if something goes wrong. Many reported cases of litigation relate to poor communication and overcharging as opposed to bad treatment. Listening carefully reduces misunderstandings and helps ensure clarity in care.
5. Patient Satisfaction
A patient who feels heard is far more likely to leave with positive feelings and return for future visits when necessary. Even if the actual time spent with a patient is short, quality listening can make them feel like they received personalized, focused attention.
6. Efficient Communication
While listening may take more time initially, it can help prevent confusion and repeated questions, and reduce the number of unnecessary follow-up calls or visits. Thus investing time early can save time later.
Strategies to aid effective listening
It is clear that effective listening plays an important role in any dental consultation, and can impact on the treatment outcome. Patients who feel heard become more open to suggestions, more compliant with treatment, and more satisfied with the healthcare practitioner. At the same time, healthcare practitioners who were considered good listeners and communicators also tended to experience less malpractice litigation.9
Listening as a skill set is not well understood. Merely hearing sound does not guarantee that an individual is actively focusing on what is being said or processing the meaning from it. While dental training may teach communication skills, the aspect of developing good listening skills is often overlooked as it is seen as common sense or falls under the banner of empathy and as such, does not get the attention it deserves.9
Authors, Barker and Watson (2000) suggested that before any meaningful listening can occur, practitioners need to identify what type of listener they are, and then be taught skills that tap into their individual profiles. They proposed that there are four main listener types: (1) people-oriented listeners;
(2) action-oriented listeners; (3) content-oriented listeners, and (4) time-oriented listeners. They noted that healthcare practitioners can have a combination of these profiles, which impacts how they should be taught the various listening skills.10 They then proposed different listening skill sets that can be taught to healthcare practitioners, which include: (1) discriminative listening, that focuses on interpreting the message based on how the words are articulated and not on the words themselves, (2) critical listening, where one not only hears what is being said but also comprehends, analyses and evaluates what is being said to form an opinion,
(3) empathic listening also known as reflective listening wherein the listener tries to understand the patient's point of view, (4) therapeutic listening also referred to as diagnostic listening undertaken by qualified health personnel, and (5) comprehensive listening which is a deeper level of active listening characterized by internalizing the spoken words and engaging the speaker to fully understand what they mean.10
Many listening exercises can be taught and learned to help practitioners develop effective listening skills, but these often require trained personnel to teach them. However, as a starting point clinicians can consciously try to eliminate distraction, be more focused on the person who is speaking (their patients), avoid thinking of an immediate answer, show respect to patients' opinions and desires, and pay attention to voice changes as well as their more subtle body language during the conversation.11
CONCLUSION
Ultimately, while billing pressures are a reality, listening to patients aligns with both ethical care and sustainable practice management. It's about balancing financial viability with compassionate patient care.
REFERENCES
1. Government gazette - Dental Codes. Accessed at: flle:///C:/Users/u28681942/ Documents/ethics%20and%20human%20rights/dental%20codes%20and%20 description.pdf; Accessed on:28-01-2025 [ Links ]
2. Jagosh J, Donald Boudreau J, Steinert Y, MacDonald ME, Ingram L. The importance of physician listening from the patients' perspective: Enhancing diagnosis, healing, and the doctor-patient relationship. Patient Educ. Couns. 2011; 85(3):369-74. doi:https://doi.org/10.1016/j.pec.2011.01.028 [ Links ]
3. Lang F, Floyd MR, Beine KL. Clues to patients' explanations and concerns about their illnesses: A call for active listening. Arch. Fam. Med. 2000; 9(3):222. [ Links ]
4. Epstein RM, Beach MC. "I don't need your pills, I need your attention:" Steps toward deep listening in medical encounters. Current Opinion in Psychology. 2023; 53:101685. doi:https://doi.org/10.1016/j.copsyc.2023.101685 [ Links ]
5. Worthington DL. Modelling and measuring cognitive components of listening. The sourcebook of listening research: Methodology and measures. 2017:70-96. [ Links ]
6. Pietrzykowski T, Smilowska K. The reality of informed consent: empirical studies on patient comprehension-systematic review. Trials. 2021; 22(1):57. doi:10.1186/ s13063-020-04969-w [ Links ]
7. Heston TF, Pahang JA. Moral injury and the four pillars of bioethics. F1000Res. 2019; 8:1193. doi:10.12688/f1000research.19754.4 [ Links ]
8. Robertson K. Active listening: more than just paying attention. Aust. Fam. Physician. 2005; 34(12):1053-5. [ Links ]
9. Shand-Mclntosh et al. (2011). Listening Education. Issue 2, (Vol. 3): pp 5- 15. [ Links ]
10. Johnston MK, Weaver JB, Watson KB, at al Listening Styles: Biological or Psychological Differences? January 2000. International Journal of Listening 14(1):32-46; DOI: 10.1080/10904018.2000.10499034 [ Links ]
11. Brittin, M. (2005). Keys to improving your listening skills. Family Practice Management, 12, 68 [ Links ]
 Correspondence:
Correspondence:
Leanne Sykes
Email: Leanne.sykes@up.ac.za
Author Contribution
1. Leanne Sykes - Primary author - 70%
2. Herman van den Bergh - 10%
3. Portia Nethononda - 10%
4. Herman Bernitz - 10%
*Code 8101 refers to a Full Mouth Examination, charting, and treatment planning. It states that no further examination fees shall be chargeable until the treatment plan resulting from this consultation is completed with the exception of code 8102. This includes the issuing of a prescription where only medication is prescribed. Code 8104 refers to a consultation for a specific problem and not to a full mouth examination, charting, and treatment planning. Except in those cases where the fee is determined "by arrangement", the fee for the rendering of a service that is not listed in this schedule shall be based on the fee in respect of a comparable service that is listed therein and Rule 002 must be indicated together with the tariff code.
