










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.80 n.4 Johannesburg May. 2025
https://doi.org/10.17159/sadj.v80i04.20799
RESEARCH
Radiation protection and compliance with radiation safety standards by dental professionals and radiographers in rural Limpopo Province, South Africa: a cross-sectional study
RM ModibaI; I NtatamalaII; T NetshisauluIII
IDepartment of Health Sciences, University of Limpopo, School of Public Health, Turfloop Campus, P/ Bag X1106, Sovenga, 0727, South Africa. ORCID: 0009-0004-3281-5156
IIDivision of Occupational Medicine and Centre for Environmental and Occupational Health Research, School of Public Health, University of Cape Town, Cape Town, South Africa. ORCID: 0000-0001-9799-0132
IIIDepartment of Physics, University of Limpopo, Turfloop Campus, P/Bag X1106, Sovenga, 0727, South Africa. ORCID: 0000-0002-7792-8494
ABSTRACT
INTRODUCTION: Poor radiation protection practices in South African healthcare facilities have been reported on account of several factors including staff shortages, poor training on radiation protection, and inconsistent dosimeter use.
AIMS AND OBJECTIVES: To investigate radiation protection practices of dental professionals and radiographers in Limpopo Province following the closure of two radiography units due to non-compliance.
METHODS: A quantitative cross-sectional study was conducted among the eight rural hospitals in the Waterberg District of the Limpopo Province, South Africa, using a self-administered questionnaire comprised of Ave components exploring the knowledge and practices of dentists (36%), oral hygienists (18%) and dental therapists (18%) and radiographers (38%). Forty-five participants (n=45) completed the study questionnaire, representing a 75% response rate (45/60).
RESULTS: Dentists (63.0%) felt slightly at risk of radiation exposure compared to radiographers who felt at risk (59.0%). Only 58.8% of radiographers, and even fewer dental professionals (37.5% of dentists and 16.7% of oral hygienists & dental therapists) admitted to always wearing their personal radiation dosimeters in the workplace (p=0.03). Equally concerning is that only a third of radiographers (29.4%) reported always protecting patients before radiological examinations compared to most dentists (93.8%) and oral hygienists & dental therapists (83.3%) (p<0.001).
CONCLUSION: Dental professionals and radiographers in this study underestimated the long-term health impacts of radiation exposure on themselves and patients, and should be better supported to comply with radiation safety protocols.
Introduction
The discovery and use of ionizing radiation (hereafter referred to as radiation) has been both beneficial and detrimental to human health. The beneficial effects of radiation include the use of x-rays in diagnostic medicine and health sciences research, but also detrimental due to potential adverse health effects arising from acute and chronic exposure. Occupational exposure to radiation is mostly associated with low dose, chronic exposure which can result in adverse health outcomes such as cataracts and thyroid cancer.1, 2, 3 As a treatment modality, ionizing radiation is intangible, neither seen or heard, which may contribute to inconsistent radiation protection and safety practices.1 Healthcare workers such as dental professionals, who are exposed to ionizing radiation of over 20mSv per annum because of their occupation are defined as radiation workers. The recent COVID-19 pandemic has further highlighted that while there was a significant focus on using personal protective equipment and improving access to occupational health services to prevent radiation workers being infected with SARS-CoV-2, there was an equal need to promote continued compliance with radiation protection practices.4,5
Several international bodies including the International Commission of Radiation Protection (ICRP), and International Atomic Energy Agency (IAEA) have highlighted the importance of adequate radiation protection and safety practice in radiation workers by making recommendations regarding radiography equipment quality, setting occupational radiation exposure limits, and detailing imaging standard operating procedures/ protocols.6, 7 The International Labour Organisation (ILO) has also adopted the Radiation Protection Convention, 1960 (No. 115), and its accompanying Recommendation (No. 114) advocating for the reduction of ionizing radiation to the lowest practicable level and avoidance of any unnecessary exposure through collaboration between employers, workers, and governments.8
Various legislation in South Africa have been promulgated as early as 1973 to regulate the amount of ionizing radiation emitted by electronic products, including the Hazardous Substances Act, 1973 (Act 15 of 1973) and Regulations (No R1332 of 3 August 1973) that govern the safe use of electronic products, including medical x-ray equipment found in dental practices and radiography units.9 The establishment of the Radiation Control Directorate in the National Department of Health (NDOH) and Code of Practice of Electronic Products have emphasized the importance of radiation protection and safety practice in all health facilities in the country based on the three main radiation protection principles of justification of the practice/investigation, optimization of protection (ALARA, keeping occupational and workplace exposures as low as reasonably achievable), and dose limitation.10
Dental professionals and diagnostic radiographers in South Africa must be registered with the Health Professions Council of South Africa (HPCSA) which has a Medical and Dental Professions Board and a Radiography and Clinical Technology Board that regulates the professional training and conduct of dental professionals and radiographers. Diagnostic radiographers perform radiation work such as general x-ray examinations, mobile radiography, fluoroscopy, angiography, computed tomography, magnetic resonance imaging, and mammography.11. The HPCSA notes for example that one of the key tasks radiographer's have include "understanding and observing health and safety at work as well as welfare issues, including infection control policies and ionising radiation regulations in order to protect themselves and others".11 Radiation safety training for radiation workers such as dental professionals and radiographers takes place during undergraduate studies and in the workplace, commonly in the first year of professional work (compulsory community/ national service year) and thereafter in the public or private sector. The quality of the training received is however variable. Van der Merwe et al12 has noted that undergraduate radiography students are often placed in clinical practice without proof of sufficient radiation safety knowledge, while Lewis et al13 has also reported insufficient training even in qualified radiographers in practice. More recently, the South African Health Products Regulatory Authority's Radiation Control Unit has hosted several radiation safety training webinars online with a focus on improving radiation safety training for radiation workers, including those in rural and remote areas who are able to livestream.14
Despite these regulations, guidance documents and training, evidence of poor radiation protection practices in South African healthcare facilities have been consistently reported in largely urban and more economically advanced areas of South Africa.15, 16, 17 There is an inequitable distribution of radiographers in South Africa, with more human and financial resources concentrated in the private health sector and larger central public sector hospitals compared to the often-under-resourced rural district and primary healthcare facilities.16, 18 As of 2020, South Africa has a national average of 5.94 radiographers per 100 000 population, which constitutes 1.2% of the public health workforce, 19 While most radiographers in South Africa's nine provinces may be employed in either the public or private sector (or both concurrently), most are employed in more developed provinces such as the Western Cape (ratio: 9.36 per 100,000 public sector population) compared to more rural provinces such as Mpumalanga (ratio: 3.42 per 100,000). 19 Other systemic challenges faced in the health sector include not wearing registered dosimeters, poor quality control on x-ray machines, the lack of specialized radiologists, customized radiation guidelines and failing infrastructure in South African health facilities. 18, 20
Significant challenges with compliance to set radiation protection standards have been experienced in largely rural and remote provinces which resulted in the closure of two x-ray/radiography units in Limpopo Province (Waterberg District) by the Radiation Control Directorate of the South African National Department of Health due to non-compliance. The factors contributing to these closures of radiation units and extent to which healthcare workers in rural healthcare facilities have adopted radiation safety practices are to be determined. The common work practices of the radiographers in the province consist of performing general and special radiological procedures that include an average of 45 x-rays per radiographer each day with a total of 1,700 x-ray examinations performed per month in the biggest hospital in the rural Waterberg District. The specialized examinations include assisting in/performing mammography, ultrasound, and computed tomography scans (CT scans) procedures. The oral hygienists, dental therapists and dentists do also assist in/perform 18 to 25 intra and extra oral radiography procedures each day including periapical, occlusal, bitewings x-rays (oral radiography) and panoramic and cephalometric x-rays (extra oral radiography). The dental professionals are not in the room during the patient exposure.
The study aims to investigate radiation protection practice and compliance with radiation safety standards by dental professionals and radiographers in rural health facilities of Waterberg District in Limpopo Province, South Africa.
Materials and methods
2.1. Study design and sampling
A quantitative cross-sectional study was conducted among the eight rural hospitals in the Waterberg District of Limpopo Province, South Africa. The study population included all radiographers and dental professionals in these institutions (one regional hospital and seven district level hospitals) to ensure a statistically significant sample size with adequate power. The total population therefore consisted of 60 radiation workers (namely 21 dentists, 6 oral hygienists and 8 dental therapists, and 25 radiographers) employed in the eight institutions. These health professionals work with both intra-oral and extra-oral x-ray machines serving a mostly rural population.
2.2. Study methods
An author generated questionnaire was developed from the available evidence-based literature. The questionnaire was comprised of a combination of closed and open-ended questions divided into Ave components. The first component consisted of socio-demographic questions regarding participant's gender, age, level of education, designation/ occupation, and length of service. The second component evaluated participant's sources of exposure and knowledge about ionizing radiation, while the third component enquired about the ill effects of radiation exposure. The fourth component was organized as a series of statements, and participants were asked to express their opinion on a 4-point scale about compliance to radiation safety protocols. The last component consisted of was open-ended questions that probed further about radiation safety protocols and the risks associated with radiation exposure. The researchers hand-delivered the questionnaires to all participants at the eight rural hospitals after obtaining access into the health facility from the management.
2.3. Data analysis
The data were analyzed using SPSS (Statistical Product Service Solutions) Version 28. The responses to open-ended questions in the last component of the questionnaire were read, and re-read by the researchers, followed by coding, and forming of categories from similar responses that addressed radiation protection practice and compliance with radiation safety standards. Descriptive statistics for continuous variables was presented as frequencies and percentages. In addition, a Pearson's chi-square test was used to determine whether there was an association between categorical variables (at a p-value < 0.05).
2.4 Consent and ethical approval
Ethical approval for the study was obtained from the University of Limpopo (MREC/H/12/2010:PG) and the Limpopo Department of Health's Research Ethics Committee (Ref 4/2/2). The ethics approval letters were shared with the Chief Executive Officers/Clinical Managers of the eight participating rural health facilities. Participation in the study was voluntary and confidentiality assured.
Results
3.1. Socio-demographic variables
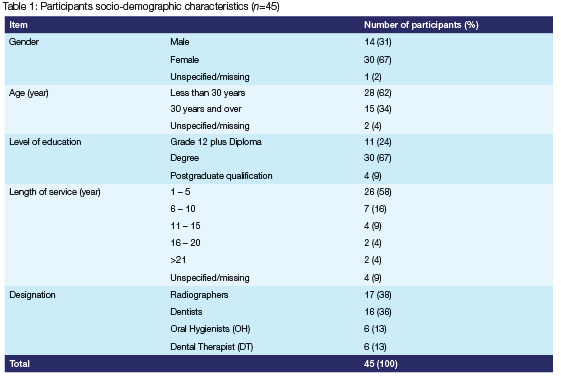
Forty-five (45) participants (Table 1) from the various rural hospitals in the Waterberg District completed the study questionnaire, representing a 75.0% response rate (45/60). The participants were largely female (67.0%) and below the age of 30 years (62.0%). The majority had received a bachelor/degree qualification (67.0%) and most had been employed for under 5 years (58.0%). Over a third (37.0%) of the participants were radiographers while remaining 63.0% were dental professionals (including oral hygienists [OH], dental therapists [DT] and dentists).
3.2 Knowledge, awareness, and perceived risk of ionizing radiation exposure
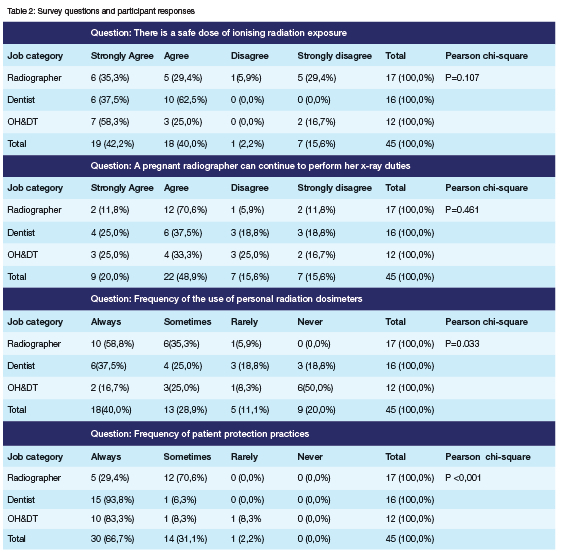
Understanding of safe dose of medical x-ray radiation Most participants were able to identify x-rays as source of ionizing radiation (100% for both radiographers, OH & DT and 95% of dentists). The participant's understanding on whether there is a safe dose of x-ray radiation from medical imaging in a day was further explored (Table 2). The majority (64.7%) of all radiographers agreed (35.3% strongly agree and 29.4% agree) that there is a safe dose of radiation from x-rays that one can take in a day. Similarly, 83.3% of OH & DT (58.3% strongly agree and 25.0% agree) and 100% dentists (37.5% strongly agree and 62.5% agree) also shared a similar view. While differences in understanding of safe dose of x-ray radiation were observed amongst the professionals, these were not statistically significant (p=0.11).
Perceived risk of radiation exposure
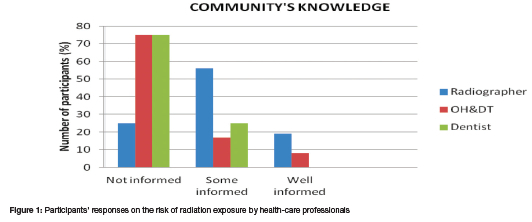
When asked about their perceived level of exposure to ionizing radiation, radiographers felt more (35.0%) or highly at risk (24.0%) of radiation exposure than other healthcare professionals while most dentists (63.0%) feeling only slightly at risk (Figure 1). Most radiographers attributed this perception to their daily continuous exposure to x-ray duties compared to other health-care professionals and the general population which would generally experience exposure only when medically warranted. Response to open ended questions identified possible factors that placed them at increased risk including the lack of access to personal dosimeters, uncertainty as to who should provide protective lead shields, poor maintenance of x-ray machines, use of mobile/portable x-ray units in theatre and when screening.
Performance of x-ray duties by a pregnant radiographer
The participant's knowledge of occupational health requirements for radiation workers, particularly vulnerable pregnant workers, was investigated (Table 2). Participants were asked whether a pregnant radiographer could continue performing her x-ray duties. Most radiographers (82.4%) agreed that a pregnant radiographer can continue to perform her x-ray duties, while dental professionals also agreed, though to a lesser extent (58.3% OH & DT and 62.5% dentists). The differences observed were however not statistically significant (p=0.46).
3.3. Radiation safety practice and compliance with radiation protection protocols
Compliance with wearing personal radiation monitoring badges/dosimeters
Participants were asked about the extent to which they complied with wearing a dosimeter (when supplied with this at the workplace). Only 58.8% of radiographers, 37.5% of dentists and 16.7% of oral hygienists & dental therapists indicated that they always wore their dosimeters (Table 2). Even more concerning is that half of the oral hygienists & dental therapists (50.0%) and 18.8% of dentists indicated that they never wore a dosimeter. The differences observed in the use of dosimeters were statistically significant (p=0.03).
Compliance with radiation protection of patients Compliance with protection of patients by covering them with lead apron and/or wearing a collar before procedures was enquired about (Table 2). Only a third (29.4%) of radiographers reported always protected patients before radiological examinations. This contrasted with responses from dental professionals (Dentists, OH & DT), majority of whom indicated that they always protect the patients before procedures (93.8% and 83.3%, respectively). The differences observed in the use of dosimeters were statistically significant (p<0.001).
The frequency with which participants repeat x-ray procedures on patients was also explored. A quarter (24%) of radiographers, 8% of OH&DT and 31% of dentists always repeat x-ray procedures because the radiograph images were not clear. Enquiry regarding compliance with radiation safety protocols to limit patient exposure including the safe filing or keeping of x-ray records revealed that 38% of dentists indicated to only sometimes keeping patients' records and 19% never keep the patients' records. Radiographers fared better in ensuring patients' records are kept, with 100% of all participants indicating that they comply with the requirement.
3.4. Perception of community's knowledge of radiation exposure risks
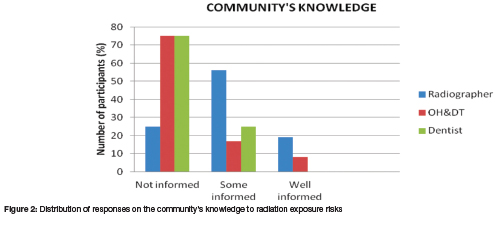
Finally, the study participants were asked about their perception of the patients/general public's knowledge of radiation exposure risks (Figure 2). A quarter (25.0%) of radiographers and the majority (75.0%) of dental professionals held a view that the public/patient community was not well informed about radiation exposure risks. Responses to an open ended question in the questionnaire indicated that possible reasons may include the low levels of literacy/education in the communities where the health facilities are located, patients not being familiar with the concept of x-rays, lack of appreciation of the health risk associated with ionizing radiation, and patients feeling disempowered to ask questions when procedures are being performed, and inconsistent/poor explanation of associated health risks by health professionals. Some participants however noted that health information, instructions and warnings are regularly provided to patients verbally and that the posters/signs on walls do explain risk associated with radiation exposure therefore patients should be better informed.
DISCUSSION
This study found that rural health facility-based dental professionals and radiographers in Limpopo Province (South Africa) were able to correctly recognize ionizing radiation as an important health hazard. More radiographers than dental professionals felt at increased risk of exposure to ionizing radiation due to their continuous occupational exposure while performing x-rays. Most radiographers agreed that a pregnant radiographer can continue to perform her x-ray duties. Most radiographers and even fewer dental professionals admitted to always wearing their personal radiation dosimeters while only a third of radiographers reported always protecting patients before radiological examinations. It was also common to repeat x-rays on patients and not keep adequate records of investigations completed. The participants perceived the public/patient community as not well-informed regarding radiation exposure risks.
The linear no-threshold (LNT) model stipulates that there is no safe level of exposure to ionizing radiation 6, and it was therefore concerning that most participants (64.7% radiographers, 83.3% of OH & DT, and 100% dentists) believed that there was a safe dose of x-ray radiation from medical imaging. This belief may be due to several factors including the perception that ionizing radiation is unseen, insufficient training on the job and a lack of focused teaching on radiation protection during undergraduate university studies. 1 13, 21, 22 The frequently stated occupational exposure dose of 20mSv per annum may have also led participants to believe that there is a safe radiation dose level. 10 These findings do however highlight the importance of ongoing education and training regarding the principles of radiation protection including justification, optimalisation of protection and limitation of all x-ray exposures (dose limits) that should be adhered to. Radiation worker's contact with the occupational health service, such as during entry medical examinations also provide an opportunity for this reinforcement to take place, particularly for new employees and those vulnerable such as those who are pregnant. 23
The fetus in pregnant women who are radiation workers is particularly vulnerable to the effects of ionizing radiation.10, 24 The participant's knowledge regarding occupational exposure to ionizing radiation for pregnant women was sufficient which is important observation in the context of this study as most of the respondents were young and female (67%) of childbearing age. Hussein et al.25 in Sudan made similar observations in their cross-sectional study of dentists, where the majority (74.3%) recognized that dental radiography was not an absolute contra-indication in pregnant women. According to the Code of Practice for Radiation Workers 10, a pregnant radiographer can continue working but the maximum equivalent dose limit of 2 mSv to the abdomen should not be exceeded. They should be monitored and issued with a direct reading pocket alarm dosimeter. Women of childbearing age are further identified as a particularly vulnerable occupational group that should receive the requisite training and be well-versed with the use of ionizing radiation.10, 24 In evaluating equivalent dose of ionizing radiation to the fetus in occupationally exposed pregnant workers, Osei and Kotre 24 confirmed that while radiation doses are generally low, it is important for pregnant staff to be encouraged to report the pregnancy early and to follow good radiation protection operational procedures for the protection of the fetus, co-workers, and patients.
Personal radiation monitoring dosimeters/badges are used for monitoring cumulative exposure to ionizing radiation that radiation workers receive. The finding that only 58.8% of radiographers in this study always wore dosimeters when performing radiation work is concerning. Though not exposed to the same extent as radiographers on a daily/ continuous basis, it is also concerning that only 37.5% of dentists and 16.7% of OH&DT always comply with the wearing of a dosimeter. Globally, radiation protection compliance levels have also been found to be as low as 59.26% among radiographers and healthcare professionals in a meta-analysis conducted in four countries.26 Other South African nationwide studies have also reported that only 16.3% of radiographers continuously used the radiation protection made available by the employer in the past21, while in specific provinces (South Africa's Gauteng Province), only 41.67% of radiographers indicating that they always wore their radiation monitoring devices.16 Other countries within the sub-Saharan region have noted concerning radiation protection practices amongst radiation workers with only 58.62% of medical imaging technologists in Rwanda having radiation-measuring devices, and 29% receiving dose readings inconsistently.27 They further found that while lead rubber aprons were available in 99% of these government hospitals, over half (59%) of the medical imaging technologists had never checked the integrity of the aprons.27 Fiagbedzi et al.28 in Ghana similarly reported that while over 90% of radiographers in their study had personal radiation dosimeters, only 25% admitted to wearing them always. The low levels of compliance in our study could be attributed to a lack of/confusing messaging on when dosimeters should be worn, lack of recognition of radiographers in the healthcare team, having to perform x-rays on difficult patients, lack of resources, inadequate training, and a lack of management support.16, 21, 27, 28
Several national guidelines and reports10, 20, 23 have detailed the importance of operators and patients wearing protective clothing however only a third (29%) of radiographers reported always protecting patients before radiological examinations. This practice could be due to several factors including having a poor understanding of the ill-effects of radiation exposure to patients or negligence/complacency in those who fully understand the risk of ionizing radiation. Previous studies in Gauteng, South Africa have reported that only 33% of radiographers knew the function of exposure indicators.17 Shiralkar et al.29 similarly reported that most doctors do not know the dose levels of radiation that their patients get exposed to during radiological investigations and that they routinely requested x-rays without weighing the necessity, thereby subjecting patients to more radiation exposure risk. The lack of providing patients with protective clothing may however also represent the recent paradigm shift away from the routine use of patient protection shielding during medical x-ray imaging as the contact shielding may interfere with the imaging process (resulting in a repeat test) or dose reduction technology, increased risk of radiation exposure should the shielding move during the examination (resulting in increased exposure), and reduced infection control practices.30, 31
This study provided evidence that patients are likely to receive more radiation exposure than necessary as a quarter (24%) of radiographers, 8% of OH&DT and 31% of dentists reported that they always repeated x-ray procedures. This routine repetition of x-ray imaging could result from poor record keeping, unnecessary requisition of x-rays and not paying attention and considerable care to ill-effects of chronic exposure to radiation. Our findings are in keeping with those by Arslanoglu et al.32, who noted that 93% of the 177 doctors underestimated the actual patient radiation dose of various radiological examinations. Thirty eight percent (38%) of dentists indicated to only sometimes keeping patients' records and 19% never keep the patients' records which could lead to patients being subjected to further radiation. Requirements for dental radiography stipulate that a record/ register of all patients undergoing x-ray examinations must be stored for a period of at least 5 years and that the repetition of x-rays is discouraged.33
Our study found a quarter (25%) of radiographers and the majority (75%) of dental professionals held a view that the public/patient community was not well informed about radiation exposure risks likely due to low levels of literacy/education, lack of familiarity with x-rays, and poor risk communication by healthcare providers. Lewis et al.34 observed that patient radiation protection knowledge influenced radiation protection practices. A study in a rural public sector hospital in Kwa-Zulu Natal, South Africa also revealed that very few patients (10.9%) had a fair knowledge about x-rays35 while less than 50% of patients attending four Jordanian local hospitals had received information on radiation awareness before medical imaging examinations. 36 With improvements in access to modern technology and greater use of artificial intelligence tools such as ChatGPT and Meta AI, patients can search for information on radiation protection and treatment plans prescribed by themselves, becoming much more self-reliant and knowledgeable about the effects of ionizing radiation.37 It is the responsibility of the health-care professionals to provide first-hand information to patients undergoing all radiological procedures and clearly articulate the risks and benefits.10, 35 36 Consent should also be sought from the patients before they undergo any radiological procedure to confirm that the patients understand the risks involved.
The study has some limitations. The study included rural health facilities in only one health district (Waterberg) out of five in Limpopo Province (Capricorn, Mopani, Sekhukhune, Vhembe) which reduced population sample size and limited generalizability of the study findings. While the focus of this study was the Waterberg District, future research should include all rural districts in the province to enable greater generalizability. The self-reported nature of the study does not make it possible to confirm the accuracy of responses regarding actual practices in health facilities, use of personal protective equipment, including the availability of equipment and resources. Social desirability bias may have reflected more positive radiation safety practices than are done in the workplace. The strength of the study is its focus on a remote and rural workforce in South Africa, in a province that has experienced closures of radiation units due to non-compliance. The study also focused on all exposed radiation workers including radiographers, and dental professionals.
This study highlights the need for several stakeholders at national, provincial and facility level to collaborate in addressing radiation protection concerns and avoiding further closures of radiation units in already resource constrained rural settings. Evidence-based radiation protection policies from the national department of health and related agencies are needed, with the requisite support provided to health facility managers and healthcare workers on their implementation.
The employer at each health facility must conduct a workplace health risk assessment as required by the Occupational Health and Safety Act 85 of 1993 to evaluate the risk to workers, and the public. The findings of the health risk assessment should inform risk mitigation strategies including building x-ray rooms compliant with set standards, procurement of required dosimeters and protective clothing in compliance with occupational health and safety legislation. Artificial Intelligence (AI) has also played an increasing role in radiation protection including dose optimization and reduction of radiation doses in select anatomical regions. 38 Patient education to improve radiation awareness should be an integral part of the health facilities daily practice to reduce unnecessary exposure from medical imaging examinations. 35, 36
To improve compliance at a healthcare worker level, it is suggested that training at undergraduate training level and once fully qualified be provided to influence attitudes and practice. 16, 21, 22 Health-care professionals should be encouraged to present for their radiation worker medical examination/surveillance, ensure that personal dosimeters are worn daily/as prescribed, and that they submit these for analysis on a regular basis. 10, 20, 23 They should also take a keen interest in reading the reports sent from their dosimeter readings. Refresher courses, continuous educational programmes to occupationally exposed health-care professionals should be reinforced and should not only focus on radiation protection, but other important occupational hazards associated with radiation work including infections and chemicals in the workplace. 4, 5, 39
CONCLUSION
This study demonstrated that though dental professionals and radiographers had identified ionizing radiation as an occupational hazard, their compliance with radiation protection and safety protocols highlights that they underestimate the long-term health impacts of radiation exposure on themselves and patients. More work is needed in drafting and implementing policies at national, provincial and health facility level to support radiation workers in better complying with radiation safety protocols. The patient population's low levels of knowledge on radiation safety should be addressed by all healthcare professionals involved in prescribing and performing x-rays and other radiological procedures.
Acknowledgements
The authors would like to thank the University of Limpopo for ethical approval, Limpopo Department of Health and hospital managers for granting access to collect data on hospitals in the Waterberg District. We thank all radiographers, oral hygienists, dental therapists, and dentists for participation in the study.
Declaration of competing interests:
The authors have declared that no competing interests exists.
Author's contributions
RM and TN were responsible for the overall study design, data collection and analysis, write-up and review of the manuscript. IN was responsible for the write up, and preparation of the manuscript. All authors were involved in commenting on the paper and have approved the final version.
Funding statement
This research received no specific funding grant from any finding agency in the public, commercial, or not-for-profit sectors.
Data availability
The data that support the findings of this study are not openly available because of reasons of confidentiality. Anonymised data are available from the corresponding author, RM., upon request.
Disclaimer
The views and opinions expressed in this manuscript are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
REFERENCES
1. Rose A, Uebel KE, Rae WI. Interventionists' perceptions on a culture of radiation protection. S Afr J Rad. 2018;22(1):1-0. S DOI: https://doi.org/10.4102/sajrv22i1.1285 [ Links ]
2. Chodick G, Bekiroglu N, Hauptmann M, et al. Risk of cataract after exposure to low doses of ionizing radiation: a 20-year prospective cohort study among US radiologic technologists. Am J Epidemiology. 2008 15;168(6):620-631. DOI: https://doi.org/10.1093/aje/kwn171 [ Links ]
3. Zielinski JM, Garner MJ, Band PR, et al. Health outcomes of low-dose ionizing radiation exposure among medical workers: a cohort study of the Canadian national dose registry of radiation workers. International journal of occupational medicine and environmental health. 2009 Apr 1;22(2):149. DOI: https://doi.org/10.2478/v10001-009-0010-y [ Links ]
4. Hazell LJ, Stork LA. Radiographer experiences of personal protective equipment during COVID-19 in Gauteng, South Africa. Journal of Medical Imaging and Radiation Sciences. 2024 Jan 3. DOI: https://doi.org/10.1016/j.jmir.2023.12.002 [ Links ]
5. Abuzaid M, Elshami W, Tekin HO. Compliance with infection control and radiation protection measures during COVID-19 in the UAE's radiology department. Journal of Medical Imaging and Radiation Sciences. 2022 Dec 1;53(4):S4. [ Links ]
6. International Commission on Radiological Protection. The 2007 recommendations of the International Commission on Radiological Protection. Oxford: Pergamon Press, 2007 [ Links ]
7. I nternational Atomic Energy Agency. Basic safety standards for radiation protection. GSR part 3. Vienna-IAEA-2014. [ Links ]
8. Niu S. Radiation protection of workers. International Labour Office; 2011 April. Available at: https://www.ilo.org/wcmsp5/groups/public/@ed_protect/@protrav/@safework/documents/publication/wcms_154238.pdf. Accessed 2024-04-02 [ Links ]
9. Herbst CP, Fick GH. Radiation protection and the safe use of x-ray equipment: laws, regulations and responsibilities: opinion. S Afr J Rad. 2012 Jan 1;16(2):50-4. DOI: https://doi.org/10.10520/EJC122041 [ Links ]
10. National Department of Health (South Africa). Code of practice for users of medical x-ray equipment. Radiation Control Directorate. 2016. Available at: https://www.sahpra.org.za/wp-content/uploads/2020/01/Code-of-practice-for-users-of-medical-x-ray-equipment-01-2015-2.pdf. Accessed: 2024-04-01 [ Links ]
11. Health Professions Council of South Africa (HPCSA). Scope of practice: diagnostic radiography (22 May 2020). 2020. Available at: https://www.hpcsa.co.za/Uploads/professional_boards/rct/guidelines/RCT_Scope_of_Practice_Diagnostic_Rad_22_May_2020_for%20Current_Scope.pdf. Accessed 14 July 2024. [ Links ]
12. Van der Merwe B, Kruger SB, Nel MM. Developing training and assessment of radiation safety regulations. Journal for New Generation Sciences. 2017 Dec 1;15(2):108-18. DOI: https://doi.org/10.10520/EJC-f09b0a768 [ Links ]
13. Lewis MS, Downing C, Hayre CM. South African radiography leadership co-constructing radiation protection change ideas. Journal of medical imaging and radiation sciences. 2022 Jun 1;53(2):248-55. DOI: https://doi.org/10.1016/j.jmir.2022.03.007 [ Links ]
14. South African Health Products Regulatory Authority. Radiation Control. 2024. Available at: https://www.sahpra.org.za/radiation-control-news-updates/. Accessed [2024-07-14]. [ Links ]
15. Nyathi T, Chirwa TF, van der Merwe DG. A survey of digital radiography practice in four South African teaching hospitals: an illuminative study. Biomedical imaging and intervention journal. 2010 Jul 1;6(1):e5. : https://doi.org/10.2349/biij.6.1.e5 [ Links ]
15. Sethole KM, Ahrens E, Kruger U. The level of compliance with the use of personal radiation monitoring devices by qualified radiographers at provincial hospitals in the Tshwane District area. Health Physics. 2019 Oct 1;117(4):426-33. DOI: https://doi.org/10.1097/HP.0000000000001064 [ Links ]
17. Moolman N, Mulla F, Mdletshe S. Radiographer knowledge and practice of paediatric radiation dose protocols in digital radiography in Gauteng. Radiography. 2020 May 1;26(2):117-21. DOI: https://doi.org/10.1016/j.radi.2019.09.006 [ Links ]
18. Kabongo JM, Nel S, Pitcher RD. Analysis of licensed South African diagnostic imaging equipment. Pan African Medical Journal. 2015;22(1). DOI: https://doi.org/10.11604/pamj.2015.22.57.7016 [ Links ]
19. National Department of Health, South Africa. 2030 Human resources for health strategy: investing in the health workforce for universal health coverage [online]. 2020. Available at https://www.spotlightnsp.co.za/wp-content/uploads/2020/08/2030-HRH-strategy-19-3-2020.pdf. Accessed 01 April 2024. [ Links ]
20. Office of Health Standards Compliance (South Africa). Improving the quality of healthcare in South Africa Annual Inspection Report 2016/17. Available at: https://knowledgehub.health.gov.za/system/files/elibdownloads/2023-04/OHSC-2016-17-ANNUAL-INSPECTION-REPORT-FINAL.pdf. Accessed: 01 April 2024 [ Links ]
21. Lewis S, Downing C, Hayre CM. Radiation protection among South African diagnostic radiographers-a mixed method study. Health Physics. 2023 Mar 1;124(3):208-16. DOI: https://doi.org/10.1097/HP.0000000000001655 [ Links ]
22. Van der Merwe B, Kruger SB, Nel MM. Radiation safety requirements for training of users of diagnostic x-ray equipment in South Africa. African Journal of Health Professions Education. 2017;9(3):123-7. [ Links ]
23. National Department of Health (South Africa). Guidelines - medical examinations for radiation workers. Radiation Control Directorate. 2012. Available at: https://www.sahpra.org.za/document/guideline-for-code-of-practice-for-users-of-medical-xray-equipment/ Accessed: 01 April 2024 [ Links ]
24. Osei EK, Kotre CJ. Equivalent dose to the fetus from occupational exposure of pregnant staff in diagnostic radiology. The British journal of radiology. 2001 Jul 1;74(883):629-37. DOI: https://doi.org/10.1259/bjr.74.883.740629 [ Links ]
25. Hussein RE, Hashim NT, Awooda EM. Knowledge, awareness and practice of Sudanese dentists towards oral radiology and protective guidelines. J. Dent. Med. Sci.. 2016;15:79-83. DOI: https://doi.org/10.9790/0853-1510047983 [ Links ]
26. Sarman I, Hassan DH. Factors affecting radiographers' compliance with radiation protection on all areas of hospital settings worldwide-a meta-analysis. International Journal for Innovative Research in Science & Technology. 2016 Sep;3(4):433-8. [ Links ]
27. Maina PM, Motto JA, Hazell LJ. Investigation of radiation protection and safety measures in Rwandan public hospitals: Readiness for the implementation of the new regulations. Journal of Medical Imaging and Radiation Sciences. 2020 Dec 1;51(4):629-38. DOI: https://doi.org/10.1016/j.jmir.2020.07.056 [ Links ]
28. Fiagbedzi E, Gorleku PN, Nyarko S, et al. Assessment of radiation protection knowledge and practices among radiographers in the central region of Ghana. Radiation Medicine and Protection. 2022 Sep 30;3(03):146-51. DOI: https://doi.org/10.1016/j.radmp.2022.06.001 [ Links ]
29. Shiralkar S, Rennie A, Snow M, et al. Doctors' knowledge of radiation exposure: questionnaire study. Bmj. 2003 Aug 14;327(7411):371-2. DOI: https://doi.org/10.1136/bmj.327.7411.371 [ Links ]
30. Samara ET, Saltybaeva N, Merce MS, et al. Systematic literature review on the benefit of patient protection shielding during medical X-ray imaging: towards a discontinuation of the current practice. Physica Medica. 2022 Feb 1;94:102-9. DOI: https://doi.org/10.1016/j.ejmp.2021.12.016 [ Links ]
31. British Institute of Radiology. Guidance on using shielding on patients for diagnostic radiology applications. Available at: https://www.bir.org.uk/media/414334/final_patient_shielding_guidance.pdf . Accessed 15 July 2024 [ Links ]
32. Arslanoglu A, Bilgin S, Kubali Z,et al. Doctors' and intern doctors' knowledge about patients' ionizing radiation exposure doses during common radiological examinations. Diagn Interv Radiol. 2007 Jun 1;13(2):53. [ Links ]
33. National Department of Health (South Africa). Guidelines - dental radiography. Radiation Control Directorate. 2017. Available at: https://www.sahpra.org.za/wp-content/uploads/2020/01/Dental-Radiography-Guidelines-2.pdf. Accessed: 01 April 2024 [ Links ]
34. Lewis S, Downing C, Hayre CM. South African radiographers' radiation protection practices, a qualitative study. Radiography. 2022 May 1;28(2):387-93. DOI: https://doi.org/10.1016/j.radi.2021.12.008 [ Links ]
35. Mung'omba B, Botha AD. Core competencies of radiographers working in rural hospitals of KwaZulu-Natal, South Africa. Afr J Prm Health Care Fam Med. 2017 Feb 22;9(1):1-8. DOI: https://doi.org/10.4102/phcfm.v9i1.1389 [ Links ]
36. Alhasan M, Abdelrahman M, Alewaidat H, et al. Medical radiation knowledge among patients in local hospitals. Journal of Medical Imaging and Radiation Sciences. 2015 Mar 1;46(1):45-9. DOI: https://doi.org/10.1016/j.jmir.2014.09.002 [ Links ]
37. Temple S, Rowbottom C, Simpson J. Patient views on the implementation of artificial intelligence in radiotherapy. Radiography. 2023 May 1;29:S112-6. DOI: https://doi.org/10.1016/j.radi.2023.03.006 [ Links ]
38. Fiagbedzi, E.W., Gorleku, P.N., Nyarko, S., et al, 2022. The role of artificial intelligence (AI) in radiation protection of computed tomography and fluoroscopy: A review. Open Journal of Medical Imaging. 2022 12(1), 25-36. DOI: https://doi.org/10.4236/ojmi.2022.121004 [ Links ]
39. Motiang KP Chelule PK. Occupational health and safety in radiographic film processing in Limpopo province. Occupational Health Southern Africa. 2017 Jan 1;23(1):21-5. DOI: https://doi.org/10.10520/EJC-5843de548 [ Links ]
 Correspondence:
Correspondence:
Name: Itumeleng Ntatamala
Email address: Itumeleng.ntatamala@uct.ac.za (I. Ntatamala)
Contributors
RM and TN contributed to the conception or design of the work, the acquisition, analysis, and interpretation of the data. All authors were involved in drafting and commenting on the paper and have approved the final version.
Funding: This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author declaration and competing interests
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical approval
Participation in the study was voluntary. Informed written consent was obtained from all participants and confidentiality assured. Ethical approval for the study was obtained from the University of Limpopo (MREC/H/12/2010:PG) and the Limpopo Department of Health's Research Ethics Committee (Ref 4/2/2).
