










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.80 n.7 Johannesburg Aug. 2025
https://doi.org/10.17159/sadj.v80i07.19969
RESEARCH
Impact of different types of smoking on the discolouration of teeth and nanocomposites
Y IbrahimI; SB KhanII; F KarjikerIII
I(BChD, MSc)
IIDepartment of Prosthodontics. University of the Western Cape (UWC). Private Bag X01, Tygerberg, 7505. Tel : +27 21 937 3006. E-mail: skhan@uwc.ac.za. ORCID No: 0000-0001-6017-959X
IIIDepartment of Prosthodontics. University of the Western Cape (UWC). Private Bag X01, Tygerberg, 7505. Tel : +27 21 9373096. E-mail: fkarjiker@uwc.ac.za ORCID No: 0009-00079515-8589
ABSTRACT
BACKGROUND: Tobacco is a commonly used and misused psychoactive substance
OBJECTIVE: Comparing the impact of different methods of smoking tobacco on tooth discolouration and colour stability of 3MTM FiltekTM Universal Nanohybrid composite
MATERIALS AND METHODS: For this in vitro study, 40 sound premolars and 40 composite discs were randomly divided into 4 groups (N=10 teeth and N=10 composite discs per group). A machine mimicking smoking was utilised, exposing the study groups to tobacco smoke as follows: Group A to cigarette smoke, Group B to e-cigarette smoke, Group C to waterpipe smoke, and Group D was the control group. The study period was over 5 days, completing 10 cycles/day. Two readings were recorded, at baseline and on day 5 for each group. Colour changes for both teeth and composite discs were determined using a stereomicroscope. Statistical analysis included using the two-way mixed measures ANOVA with Bonferroni corrections
RESULTS: The darkest colour was shown with cigarette smoke exposure in group A for the teeth and composite discs. A statistically significant difference in change of tooth and composite colours were observed (p-value < 0.001
CONCLUSION: All different tobacco consumption methods contributed some degree to tooth discolouration and composite colour change
Keywords: Cigarette smoking, E-cigarette smoking, Waterpipe smoking, Tooth Staining, Colour Stability, nanocomposite.
INTRODUCTION
Tobacco has been reported to be a very misused psychoactive substance among the world's rural and urban populations.1 The World Health Organisation (WHO) reported that more than 8 million individuals die every year from tobacco use.2 This number is predicted to rise to 10 million deaths by 2031.3 Smoking tobacco has increased, and new consumption methods have become a trend, especially amongst the younger generations.4
Tobacco is generated from two plant species: Nicotiana tabacum and Nicotiana rustica.5 Tobacco products are manufactured from raw tobacco leaves which all contain highly addictive psychoactive ingredients.6 Some of the active ingredients of tobacco include solid submicron-sized particles like nicotine, polyaromatic hydrocarbons, phenols and nitrosamines, and the gas constituents are carbon monoxide, hydrogen cyanide and nitrogen oxides.6 Damage caused by tobacco is from one of 3 ways: (i) Its addictive ability from nicotine 5; (ii) the physical and /or heat irritation from the devices wherein it is used7, and (iii) development of pathology from chemical and molecular interactions between oral cavity tissues and tobacco products.7
Generally, tobacco products are divided into two types, smoked tobacco and smokeless tobacco.8 The smoked tobacco products include normal cigarettes (menthol cigarettes, light, hand-rolled, natural, or herbal cigarettes), clove cigarettes (kreteks), bidis (flavoured cigarettes), electronic or e-cigarettes (ECIGs), waterpipes, cigars, little cigars and sticks are included under this category.8 Smoked tobacco comes in different types and methods of consumption and the method of tobacco use determines the site at which tissues are most impacted.7
Cigarettes represent the core of all tobacco products.9 In vitro and clinical studies indicate that the toxicity and the smoke produced from conventional cigarettes is more than any other type of tobacco product.10 These researchers also found that smoke from ECIGs and other tobacco heating products was much simpler and contained fewer elements.10 Moreover, their research indicated that human cells and composite material responded less to ECIGs and tobacco heating products.10
EClGs or electronic nicotine delivery systems (ENDS) or vaping, was first introduced to the market in 2004 as an approach to help smokers quit smoking by delivering nicotine in a vapour form (nicotine-containing aerosol) without calcination.7, 11-12 Their popularity has significantly increased worldwide in recent years. Vaping is becoming a popular trend among both traditional cigarette smokers and non-smokers, including adults and teenagers.13 Since its introduction, significant advancements have resulted in multiple generations of ECIGs, thus 460 different types and 7000 different E-liquid flavours, which is its greatest appeal, are currently available.12-13 However, the long-term effects of ECIGs use remain unclear, notwithstanding the risk of nicotine addiction, which is higher among its users.14-16
Tobacco in all its forms has deleterious effects on the population and their health, including oral health, and are the cause of several systemic diseases and oral conditions. The oral effects of smoking tobacco range from simple tooth staining to more serious and fatal diseases like oral cancer.17-18 According to researchers, smokers not only had poor oral and dental hygiene (such as poor tooth brushing practices), but also unacceptable views of health (consuming more sugars and alcohol). Dentists, due to the nature of their patient interactions, will likely have easy access to 'healthy' smokers, even if there are no tobacco-related illnesses observed in the mouth. Dentists can determine, as part of routine history taking, and quickly detect the patient's smoking status. This places them in a unique position to guide smokers to prevent developing tobacco-related illnesses.17, 19
Tooth staining or tooth discolouration is one of the major aesthetic concerns experienced by the population. Extrinsic discolouration, which is caused by external factors, adheres to the outer surface of the tooth, for example, tea, coffee, tobacco stains and medications.20 Smokers develop tobacco stains on their teeth due to exposure to inhaled cigarette smoke. Pigmented compounds in the tar may be deposited on the surface or even penetrate dental enamel, thus causing discolouration.20-21 In an in vitro study aimed to evaluate the effect of ECIGs on enamel colour, bovine enamel blocks were exposed to 20 cycles of ECIG smoke with different e-liquid flavours and nicotine concentrations. The results indicated that ECIGs do change the colour of enamel as well as the micro-hardness of enamel.14, 22 A recent survey aimed to look at the effect of waterpipe smoking on oral health and here 60% of the participants noticed stains on their teeth after its use.23
Similarly, composite restorative material colour changes, developing from either extrinsic or intrinsic factors, have been identified by practitioners impacting on aesthetics.24 Other studies conducted to determine the effect of cigarette smoking on composites indicated a substantial decrease in the colour stability and exacerbated the staining of materials with smooth or texturised surfaces.25-26 Although repolishing helps to reduce surface stains, the composite may not return to its original colour.26
Rationale
The different methods of smoking tobacco have increased and become a trend amongst young adults. Moreover, smoking that causes staining of teeth and restorations impacts patients' aesthetics and thus social relations, especially of those teeth in the aesthetic zone. Nanohybrid composite shows superior properties compared to the other available composite resins, thus it is the material of choice for clinicians.
This study therefore aimed to detect the effect of the different types of tobacco smoking methods on teeth and 3MTM FiltekTM Universal Nanohybrid composite to give value and a reference for future clinical use.
Null Hypothesis
There is no significant difference regarding the impact of the different types of smoking tobacco on teeth and nanohybrid composites such as 3MTM FiltekTM Universal Nanohybrid.
Methodology
This in vitro experimental laboratory study explored the effects of different smoking methods viz: cigarettes, e-cigarettes and a waterpipe on tooth colour and nanohybrid composite colour, and compared these between the different exposure groups. The samples included sound extracted premolar teeth obtained from the service rendering department at the Tygerberg Oral Health Centre and 3MTM FiltekTM Universal Nanohybrid composite discs. Following previous studies, it was determined that a definitive sample size of 40 teeth and 40 composite discs would be sufficient to yield results which would be statistically significant.27-28
1. Preparatory stage:
Machine preparation:
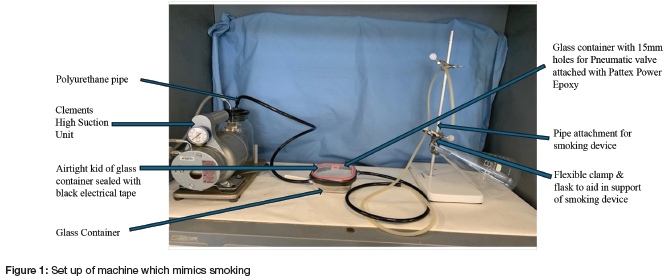
A machine which mimicked smoking was custom made. The machine was constructed using a Clements High Suction Unit (H.I. CLEMENTS PTY.LTD; Sydney, Australia), a glass container, pneumatic valves, and poiyurethane pipes (Figure 1). Two holes were prepared on the glass container and the pneumatic valve was attached to each, to control the inflow and outflow of air via these (Figure 1). The sealed glass container (airtight lid and black tape) also included polyurethane pipe connections to ensure a closed seal of the entire system. The Clements high suction unit was used to produce the required pressure to mimic the inhaling process, which was calibrated to be approximately 20mmHg.27 The machine was placed in a fume cupboard under a fume hood to remove all smoke produced by any of the methods of smoking.
Sample preparation:
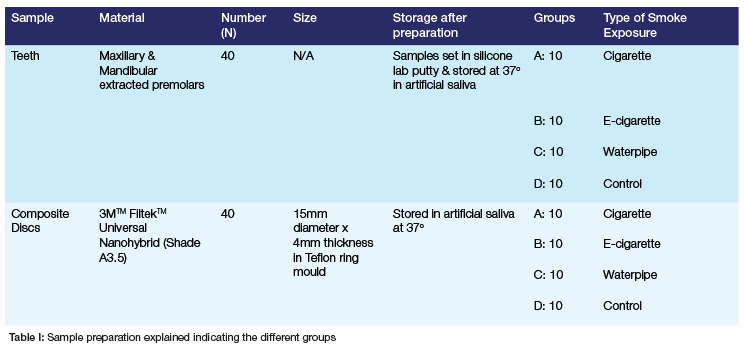
The table explains the groups used in the study.
All 40 extracted premolars were cleaned, sterilised, and scaled using a Satelec Newtron Handpiece and polished using a slow handpiece and NUPRO fluoridated polishing paste (Dentsply, USA) 2 weeks before the experiment was conducted and then kept moist. Tooth samples were set in silicone lab putty 24 hours before the experiment (Table I). Each increment of each composite disc (N=40) was cured using an Elipar DeepCure-S LED curing light (3M ESPE, USA), for 10 seconds as per manufacturer's instructions. Disc thickness was measured using an electronic digital calliper (Ketotek, China).
The discs were polished using the 3M ESPE Sof-Lex polishing discs and finished using the Enhance Finishing System from Dentsply Sirona (USA). Both tooth and composite disc samples were stored in artificial saliva, made in the laboratory, at 37°C (Table I).29
2. Testing Stage:
Group A: The smoking machine was set, and a Malboro cigarette filter tip was attached to the polyurethane pipe, sealed using a mouth tip and electrical tape. The cigarette was placed inside a flask to eliminate any air that may accelerate its burning. The Clements high suction unit was switched on, the cigarette lit, and the suction unit was switched off when the cigarette had burned up to the filter tip. The time for the consumption of each cigarette was also measured. The smoke produced during this action, was transferred to the glass container via the polyurethane pipe. A period of 10 minutes was allowed between each cigarette to allow the smoke to be circulated and its chemicals deposited on the teeth and composite discs. This smoking cycle was repeated 10 times per group of teeth and composites as there were 10 cigarettes per pack for 5 days.
Each cigarette's burning time was calculated, and an average daily exposure time was used to be a standard for the other two groups' cycle time. Both the teeth and composite discs were stored in distilled water at 37OC, that was replenished daily.22, 29
Group B: The SMOK® e-cigarette (ECIG) was installed and charged daily. The e-liquid was poured into the glass reservoir and filled for each cycle. The flask holder was used to hold the e-cigarette in place and the drip tip (mouth part) was fixed into the polyurethane pipe with electrical tape. The Clements high suction unit was turned on, as was the power switch of the e-cigarette. The produced smoke was transferred through the polyurethane pipes into the glass container. This cycle was repeated 10 times for 5 days for the composite discs and extracted teeth of Group B.
Group C: The waterpipe was set up, water filled 3/4 of the vase as recommended, 2 small spoons of Two Apples flavour (Al Fakher Tobacco Trading Co. Ajman, UAE) were stuffed in the bowl and covered with foil. The foil was punctured to allow the heat from the burnt charcoal to reach the flavoured tobacco. Two tablets of instant-light charcoal were used every 5 cycles. The mouthpiece was fixed into the polyurethane pipe with electrical tape. The Clements high suction was switched on and the produced smoke was transferred to the glass container via the polyurethane pipe. The cycle time was determined according to the average time for a cigarette to burn. This cycle was repeated 10 times a day for 5 days.
Group D: Both the composite discs and the teeth served as the control group, and these were not exposed to anything. The samples were stored in distilled water at 37OC which was replenished daily. The following protocols were followed for all 4 groups of tooth and composite samples daily. At the end of each smoking exposure cycle, the fume cupboard hood was turned on to remove any residual smoke.
3. Analysis Stage: Colour Changes
Prior to examining the colour measurement of the teeth and composite discs, the Zeiss Stemi 508 stereomicroscope (Zeiss, Oberkochen, Germany) was calibrated as per manufacturer's recommendations. Images were transferred using ZEN Lite software. To standardise the colour measurement process, the teeth were dried for 3 seconds, and then absorbent paper was used to remove excess moisture. A white sheet of paper was used as a background to eliminate any error in the readings.
The sample teeth were placed under the microscope and the colour readings of each sample were recorded usig the L*, a* and b* scale of the CIELAB colour space (Fig 2).

The explanation of the scales of the CIELAB colour space chart are:
- L* represents lightness from black to white on a scale of zero to 100,
- a* and b* represent chromaticity with no specific numeric limits,
- Negative a* corresponds with green, and positive a* corresponds with red, and
- Negative b* corresponds with blue and positive b* corresponds with yellow (Fig 2).30
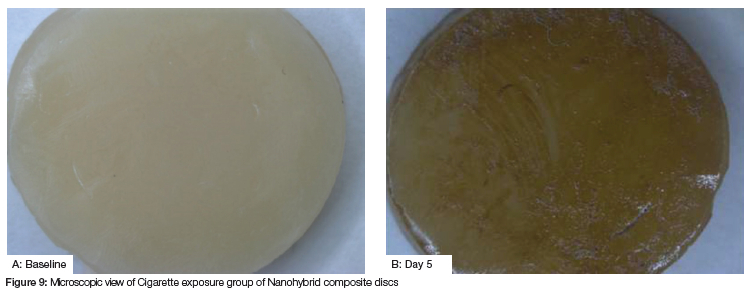
For this study, baseline colour readings were obtained for each sample, colour measurements were taken on both buccal and palatal/lingual surfaces. Each reading was repeated three times. Subsequent readings were obtained after 5 days. A single specimen from each group which was exposed to the different types of tobacco was photographed to visually demonstrate any possible effects. To illustrate the effect of the different types of smoked tobacco on nanohybrid composite restorations, one specimen of each group was photographed before and after exposure to smoke.
Disposal of the extracted teeth was done through Tygerberg hospital disposal system for human tissue.
Statistical Analysis
The changes in tooth colour and composite disc colour after staining were observed and recorded. The results hereof are displayed by box plots and mean and standard deviation tables. The statistical analysis includes the 2-way mixed measures ANOVA with Bonferroni corrections.
Results
For this cross-sectional laboratory study, the project was registered with the institutional ethics review board (BMREC Reg No: BM19/9/4). The results of the pilot study with teeth and composite discs (N=10) guided the sample size finalisation. Following this, the effect of the different types of smoking was studied and its impact on the colour of the teeth and composite material in the form of composite discs is reported below.
a. Changes in tooth colour
The sample of teeth (N=40) were finalised for each group exposed to:
• cigarette smoke (Group A),
• e-cigarette (Group B),
• water pipe (Group C) and
• control group (Group D - no exposure).
Colour readings were taken on both buccal and lingual surfaces of each tooth and an average per tooth was calculated. Readings were documented as an intensity mean value which indicates the hue of the tooth colour. All samples (tooth and composite) had readings done at baseline (Day 0) and on the 5th day of exposure (Day 5) (Figure 3).
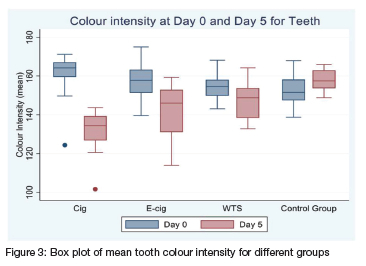
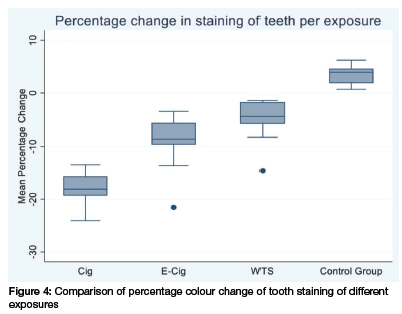
Figure 4 indicates the comparison of tooth staining between the different exposure groups, indicated by the mean percentage tooth colour change. The variation in colour changes between exposure groups was recorded at baseline and day 5. The negative change is indicative of darker colour intensity. The darkest colour is shown in group A exposed to cigarette smoke (mean colour change=132.51 and SD=10.03955), followed by group B exposed to e-cigarettes. Whilst the mean colour change for Group C that was exposed to waterpipe smoke, showed even less colour change compared to Groups A and B. The smallest percentage change in tooth colour is shown among group D, the control group.
To determine and compare the effects of different types of smoking exposures on teeth, a two-way mixed measures ANOVA with Bonferroni corrections for tooth discolouration analysis, was employed. The results of the ANOVA test where the average mean of tooth staining readings between groups was compared, indicates that there was a statistically significant difference in change of tooth colour between the four different exposure groups (p-value of < 0.001).
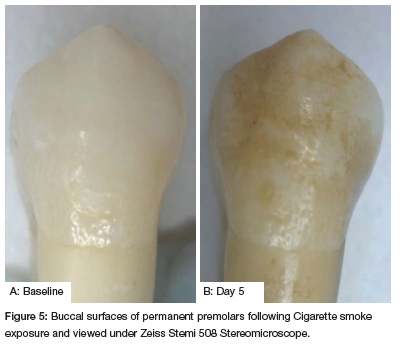
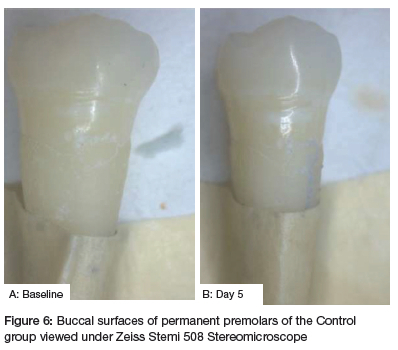
When applying the Bonferroni corrections for tooth discolouration analysis between these 4 exposure groups, the largest difference in tooth colour intensity was seen between group D and group A at a 95% confidence interval (Fig 4, 5). Group A was darker than group D with a contrast of 21.22 (CI: 16.51-25.96), which was statistically significant (p < 0.001). This was followed by a statistically significant difference (p < 0.001) between group C and group A with a contrast of 12.793 (CI: 8.082-17.504), and which was followed closely by the difference between group B and D (p < 0.001; CI: 8.025-17.447). A statistically significant difference was also observed between groups A and B (p < 0.001; CI: 3.777 to 13.199) and between groups C and D (p < 0.001; CI: 3.720 to 13.142). However, the smallest difference was seen between groups C and B with a contrast of 4.305 (CI: -.405 to 9.016) but this was not statistically significant (p-value = 0.091).
b) Composite Staining
The colour staining of 3MTM FiltekTM Universal Nanohybrid composite in the four study groups exposed to cigarette smoking, e-cigarettes, waterpipe smoking, and the control group was also measured. Two readings were recorded, first at baseline (Day 0), and then the second reading was taken on the fifth day after the exposure (Day 5). Reading values were reported according to the intensity mean value, which reflects the hue of the colour from the scale of the CIELAB colour space chart.
The box plot (Fig 7) displays the mean values of the study composite discs colour intensity on day 0, and day 5. Baseline colour was the lightest for group A, followed by group C then by group D, the control group. The darkest baseline colour was for group B, the E-cigarette group.
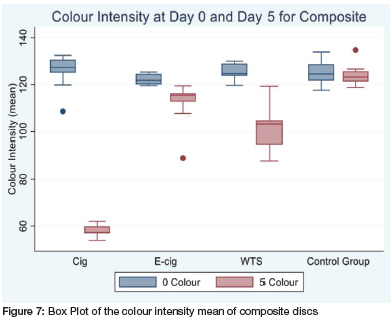
On day 5, the mean colour change was the lightest for groups D, B, C, and A with the intensity in this order (Figure 7 below).
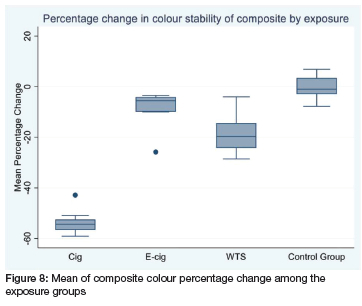
The mean composite colour % change among the four groups is shown in the box plot (Fig 8 below). The negative change is indicative of a darker colour intensity. The darkest colour showed in group A exposed to cigarette smoke (mean colour change -53 and SD=4.45), followed by the group C exposed to waterpipe smoke, then by group B, the E-cigarette sample. The smallest percentage change in composite colour was shown among group D, the control group (Fig 8 below).
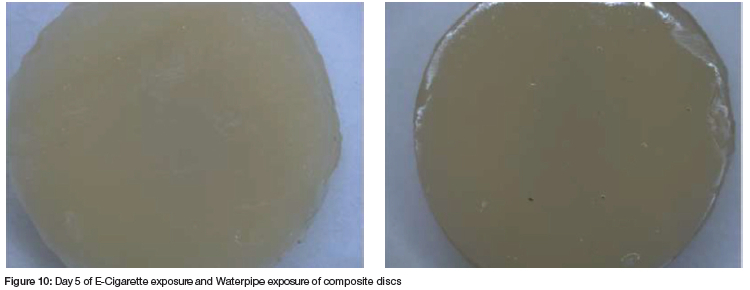
On average, the 3MTM FiltekTM Universal Nanohybrid composite colour is darker between day 0 and day 5 for the group exposed to cigarette smoke (Fig 9). The waterpipe exposure group C showed some colour changes too, with the E-cigarette showing minimal differences between the shades for this period. However, there was a decrease in colour intensity in exposure D control group.
The effects of different types of smoking exposures on 3MTM FiltekTM Universal Nanohybrid composite discs were measured, analysed, and compared across the study groups using a two-way mixed measures ANOVA with Bonferroni corrections for colour staining analysis.
When comparing the different exposure groups for the colour change of the composite samples by employing the ANOVA test, the average mean of the colour staining readings were found to be statistically significant (p-value< 0.0001). In addition, when applying the Bonferroni corrections for composite colour change analysis, to examine the comparison between exposure groups at a 95% confidence interval, results confirmed that there was a statistically significant difference between some of the exposure groups. The difference seen between exposure groups D and B was not statistically significant (p = 0.066).
The largest statistically significant difference in composite colour intensity was seen between groups D and A, where group A was darker with contrast of 53.11878 (p < 0.001; CI: 45.29316-60.94441). Comparing the different groups to Group A, the difference in colour intensity was also statistically significant between groups B and A (p < 0.001) and between groups C and A (p < 0.001), where Group A was always darker (Fig 9, 10). The difference between the control group D and group C (waterpipe group) was also statistically significant (p<0.001), but the difference between groups C and B was not significant (p=0.006).
DISCUSSION
Following the completion of this study and the outcomes achieved, the null hypothesis 'there is no significant difference in the impact of the different types of smoking tobacco on teeth and nanohybrid composite' can be refuted. The details of these outcomes are outlined further and in line with the literature.
This study was rather unique as it used different smoking types and compared these. In many other studies, the researchers demonstrated the effect of cigarette smoking on the staining of teeth, but very few have investigated the effects of e-cigarette and waterpipe smoke on teeth. For this study, the sample selection was also random, and it was observed that there was a difference between baseline colour readings in all the exposure groups as the sample of teeth were from different people. The importance of similar variables at baseline is thus important as difference can impact on the study outcomes.
It was also observed that staining between groups differed, especially between exposure to cigarettes and e-cigarettes. This could be attributed to the fact that the composition of tobacco in a cigarette is more complex than that of the liquid in an e-cigarette.10
The results from this study showed that different smoking methods may cause some degree of tooth staining and composite colour change, and this is supported by findings of several researchers.10, 22, 31 These findings reported how cigarette smoking causes the darkest tooth discolouration, followed by e-cigarette and waterpipe smoking, and where the control group was the lightest in colour, which is similar to this study.
The current study's results also showed that e-cigarette smoke resulted in less tooth discolouration compared to cigarettes. However, Dalrymple et al (2018)31 proposed that a more plausible explanation for this difference can be related to the complex nature of the composition of the cigarette compared to that of the e-cigarette.31 Zhao et al (2019)10, in line with this study's outcomes, indicated that cigarette smoke caused more discolouration of teeth than e-cigarette smoke.10 The effect of waterpipe smoking on tooth discolouration conducted in this study, was supported by the Lakdawala et al (2019) study.23 They investigated the effect of waterpipe smoking on enamel and found that it also caused an alteration in tooth colour.
This study showed that there was a statistically significant difference in the change of tooth colour amongst the four groups of different types of smoking. This is important and the outcomes significant as the study conditions were the same for each exposure group. The implication was that when different smoking methods are used under the same circumstances, each of them would have a different effect on tooth colour. However, there was only a small statistical difference between the effects of waterpipe smoking and e-cigarette smoking, while differences between the effects of other types of smoke exposure were significant. More importantly, the impact of smoking on teeth affects the aesthetics, which will be of great concern for clinical practitioners.
Similarly, for this study the greatest colour change on the composite discs was noted in the group exposed to cigarette smoke, followed by waterpipe smoking and e-cigarette smoking. Thus, all smoking methods lead to a change in composite colour, and the implication of this means that clinically exposure to smoking would lead to aesthetic failure. This conclusion is supported in the literature by findings by Zhao et al. (2019)10, Raptis et al. (1982)25, and Vieira-Junior et al. (2020).10, 25, 32
Raptis et al (1982)25 many years ago suggested that tobacco smoking caused a change in colour due to the remaining unreacted monomers after curing. Then years later, Vieira-Junior reported in 202032 that 99% of the nicotine present in the particulate phase of tobacco happens to be yellow in colour.32
Zhao et al (2019)10 conducted research and reported that cigarette smoke showed a greater colour change in composite colours than any exposure to e-cigarette smoke.10 It was also reported that the cause for the discolouration of both teeth and composites which are exposed to e-cigarettes was because of the yellowish colour which is produced from the oxidation of nicotine in the e-cigarette flavours.
New smoking trends have resulted in an increase of tobacco use across a much broader age spectrum. In contradiction to the various methods of tobacco use, there is a greater awareness and concern about dental aesthetics and the appearance of the smile. The population is becoming more concerned about having stain free, white teeth. Thus, the importance of conducting this research cannot be overemphasised and the next phase in translating these in vitro outcomes would be to conduct more clinically related research that could guide clinical practice.
CONCLUSION
The different means of consuming tobacco causes various degrees of tooth and composite discolouration. Cigarette smoking still causes more drastic tooth and composite colour changes, compared to an e-cigarette, and waterpipe smoking.
CLINICAL SIGNIFICANCE
The dental professional is in a good position to monitor "healthy" smokers and can identify tobacco-related conditions, and even recognise a patient as a smoker based on the presentation of the oral cavity. This means that the dental professional is in a unique position to counsel a patient on smoking cessation and should seek formal training to achieve this.
That said, not having had any formal training in counselling patients in smoking cessation, identifies this as an important gap in their undergraduate training. This type of counselling can be routinely included in the dental profession and should be part of plaque control, nutritional guidance, and oral hygiene instruction.17 In addition, during dental appointments, smoking cessation treatments (including counselling) are effective in helping patients quit smoking.12
LIMITATIONS
The study conducted was in vitro. Staining has a multifactorial aetiology and is impacted by several factors such as dental hygiene, consumption of certain foods and beverages and even the aging process.20 Since these factors cannot be addressed in an in vitro study, or was not even the aim of the researchers, it clearly is a limitation of the study. In addition, the composite discs (study sample) were polished using a handpiece, 3M ESPE Sof-Lex polishing discs and finished using finishing discs from the Enhance finishing system by Dentsply Sirona. The resultant thickness of the discs after polishing and the smoothness of the discs would differ from disc to disc as pressure during polishing would not have been consistent using a handpiece. This clearly makes polishing in this manner and its effect a limitation of the study.
REFERENCES
1. Omare MO, Kibet JK, Cherutoi JK, Kengara FO. A review of tobacco abuse and its epidemiological consequences. Journal of Public Health. 2021 Jan 6;30(6). [ Links ]
2. WHO, 2019. Don 't Let Tobacco Take Your Breath Away. World Health Organisation, p.1-12. [ Links ]
3. Nidhi N, Singh SP. Assessment of Prevalence of Dental caries among smokers and smokeless tobacco users - A Descriptive Study. International Journal of Contemporary Medicine, Surgery and Radiology. 2019 Jan;4(1). [ Links ]
4. Pisinger C, Døssing M. A systematic review of health effects of electronic cigarettes. Preventive Medicine. 2014 Dec; 69:248-60. [ Links ]
5. Res, M. et al. Prevalence of Filtek. Restorative, U. 2018 May, p. 517-520. doi: 10.4103/ijmr.IJMR. 'Filtek'. [ Links ]
6. Perez-Warnisher MT, De Miguel M del PC, Seijo LM. Tobacco Use Worldwide: Legislative Efforts to Curb Consumption. Annals of Global Health [Internet]. 2018 Nov 5;84(4):571. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6748295/ [ Links ]
7. Ford PJ, Rich AM. Tobacco Use and Oral Health. Addiction. 2021 Apr 6;116(12). [ Links ]
8. Vellappally S, Fiala Z, Šmejkalová J, Jacob V, Somanathan R. Smoking Related Systemic and Oral Diseases. Acta Medica (Hradec Kralove, Czech Republic). 2007;50(3):161-6. [ Links ]
9. Vellappally, S. Fiala, Z. Šmejkalová, J. Jacob, V. and Shriharsha, P. (2007). Smoking and Dental Caries. Central European Journal of Public Health, 15(3), p. 116-121 [ Links ]
10. Zhao X, Zanetti F, Wang L, Pan J, Majeed S, Malmstrom H, et al. Effects of different discolouration challenges and whitening treatments on dental hard tissues and composite resin restorations. Journal of Dentistry [Internet]. 2019 Oct 1; 89:103182. Available from: https://pubmed.ncbi.nlm.nih.gov/31430508/ [ Links ]
11. Grana R, Benowitz N, Glantz SA. E-Cigarettes. Circulation. 2014 May 13;129(19):1972-86. [ Links ]
12. Kumar P, Geisinger M, DeLong HR, Lipman RD, Araujo MWB. Living under a cloud: Electronic cigarettes and the dental patient. The Journal of the American Dental Association. 2020 Mar 1;151(3):155-8. [ Links ]
13. Rouabhia, M. Impact of Electronic Cigarettes on Oral Health: a Review. Journal Canadian Dental Association. 2020 86, p. k7. [ Links ]
14. Pintado-Palomino K, de Almeida CVVB, Oliveira-Santos C, Pires-de-Souza FP, Tirapelli C. The effect of electronic cigarettes on dental enamel color. Journal of Esthetic and Restorative Dentistry. 2018 Oct 27;31(2):160-5. [ Links ]
15. Raj AT, Sujatha G, Muruganandhan J, Kumar SS, Bharkavi SI, Varadarajan S, et al. Reviewing the oral carcinogenic potential of E-cigarettes using the Bradford Hill criteria of causation. Translational Cancer Research. 2020 Apr;9(4):3142-52. [ Links ]
16. Jha P. The Hazards of Smoking and the Benefits of Cessation: A Critical Summation of the Epidemiological Evidence in High-Income Countries. eLife [Internet]. 2020 Mar 24;9(1). Available from: https://elifesciences.org/articles/49979 [ Links ]
17. Reibel J. Tobacco and Oral Diseases. Medical Principles and Practice. 2003;12(Suppl. 1):22-32. [ Links ]
18. Jiang X, Jiang X, Wang Y, Huang R. Correlation between tobacco smoking and dental caries: A systematic review and meta-analysis. Tobacco Induced Diseases. 2019 Apr 19;17(April). [ Links ]
19. Terrades M, Coulter WA, Clarke H, Mullally BH, Stevenson M. Patients' knowledge and views about the effects of smoking on their mouths and the involvement of their dentists in smoking cessation activities. British Dental Journal. 2009 Dec; 207(11): E22-2. [ Links ]
20. Hattab FN, Qudeimat MA, Al-Rimawi HS. Dental Discoloration: An Overview. Journal of Esthetic and Restorative Dentistry. 1999 Nov;11(6):291-310. [ Links ]
21. Zanetti F, Xiu Song Zhao, Pan J, Peitsch MC, Hoeng J, Ren YF. Effects of cigarette smoke and tobacco heating aerosol on color stability of dental enamel, dentin, and composite resin restorations. Quintessence International. 2019 Jan 25;50(2):156-66. [ Links ]
22. Bertoldo CE. dos S, Miranda D. de A, Souza-Júnior EJ, Aguiar FHB, Lima DANL, Ferreira RL. Claes IL J. Surface hardness and color change of dental enamel exposed to cigarette smoke. (2011) Int Journal of Dental Clinics, 3(4), p. 1-4. [ Links ]
23. Lakdawala YA, Masood S, Shamsi B, Aftab H, Khattak L, Jaffrani A. Pipe Smoking and its Oral Health Effects on Smokers - A Survey. (2019) Pakistan Oral & Dental Journal, 39(1), pp. 69-71. [ Links ]
24. Menon, A. Ganapathy, DM. and Vadaguru Mallikarjuna, A. Factors that influence the color stability of composite resins. (2019) Drug Invention Today /. Available at: http://content.ebscohost.com/ContentServer. [ Links ]
25. Raptis CN, Powers JM, Fan PL, Yu R. Staining of composite resins by cigarette smoke. Journal of Oral Rehabilitation. 1982 Jul;9(4):367-71. [ Links ]
26. Mathias P, Costa L, Saraiva LO, Rossi TA, Cavalcanti AN, Da Rocha Nogueira-Filho G. Morphologic Texture Characterization Allied to Cigarette Smoke Increase Pigmentation in Composite Resin Restorations. Journal of Esthetic and Restorative Dentistry. 2010 Aug 2;22(4):252-9. [ Links ]
27. Alandia-Roman CC, Cruvinel DR, Sousa ABS, Pires-de-Souza FCP, Panzeri H. Effect of cigarette smoke on color stability and surface roughness of dental composites. Journal of Dentistry [Internet]. 2013 Aug [cited 2019 Nov 17]; 41: e73-9. Available from: https://www.sciencedirect.com/science/article/pii/S0300571212003272 [ Links ]
28. Zanetti F, Xiu Song Zhao, Pan J, Peitsch MC, Hoeng J, Ren YF. Effects of cigarette smoke and tobacco heating aerosol on color stability of dental enamel, dentin, and composite resin restorations. Quintessence International. 2019 Jan 25;50(2):156-66. [ Links ]
29. van der Bijl, P. and de Waal, J. Preparation and clinical evaluation of a high viscosity saliva substitute. (1994) The Journal of the Dental Association of South Africa (SADJ), 49(6). [ Links ]
30. https://www.hunterlab.com/blog/what-is-cielab-color-space/#:~:text=L*%20represents20lightness%20from%20black,positive%20b*%20corresponds%20with%20yellow). [ Links ]
31. Dalrymple A, Badrock TC, Terry A, et al. Assessment of enamel discoloration in vitro following exposure to cigarette smoke and emissions from novel vapor and tobacco heating products. American Journal of Dentistry. 2018, 31(5), pp. 227-233. [ Links ]
32. Vieira I, Vieira-Junior W, Pauli M, Theobaldo J, Aguiar F, Lima D, et al. Effect of inoffice bleaching gels with calcium or fluoride on color, roughness, and enamel microhardness. Journal of Clinical and Experimental Dentistry. 2020; e116-22. [ Links ]
 Correspondence:
Correspondence:
Dr Farzana Karjiker
Tel : +27 21 9373096. Email: fkarjiker@uwc.ac.za
Author contribution
YI: Contributed to study Conceptualisation; Protocol preparation, Data collection and Analysis, Thesis completion and Manuscript preparation and manuscript finalization. (50%)
SK: Contributed to Supervision, Protocol and its preparation, Data finalisation; Thesis completion, Manuscript preparation and manuscript finalization. (30%)
FK: Contributed to Conceptualisation, Data collection, Thesis completion and Manuscript preparation and manuscript finalization. (20%)

{kind=link}
{kind=link}
{kind=link}
{kind=link}