










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151Print version ISSN 0038-2361
S. Afr. j. surg. vol.60 n.3 Cape Town Sep. 2022
https://doi.org/10.17159/2078-5151/sajs3869
CASE REPORT
Nipple-areolar complex: commonest site of breast leiomyoma
W Ngwisanyi; G Tshimbidi; M Keyter; C-A Beim
Department of Surgery, University of the Witwatersrand, South Africa
ABSTRACT
Breast leiomyomas are extremely rare and commonly seen in the nipple-areolar complex due to the presence of smooth muscle. Identification of this rare benign tumour is based on its location and the presence of spindle cells on histology. We report a case of a breast leiomyoma in a female patient who had a six-year history of a unilateral breast mass. Breast ultrasound and mammography demonstrated a sub-areola mass and an ultrasound-guided core biopsy revealed a benign spindle cell neoplasm with smooth muscle differentiation. The lesion was excised and final histology confirmed a leiomyoma with clear margins.
Keywords: breast leiomyoma, sub-areolar, rare tumour, smooth muscle
Case report
A 59-year-old female with hypertension and type 2 diabetes, well-controlled on oral medications, presented to our breast clinic with a six-year history of a right breast mass. She described the mass as painless with no significant growth. There was no family history of breast cancer.
On clinical examination, a non-tender, immobile, 10 mm x 10 mm sub-areola lump was present in the right breast. No nipple discharge, skin or lymph node involvement were noted.
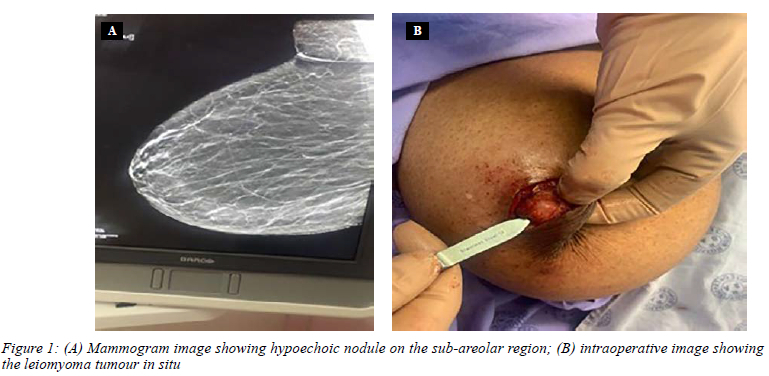
Mammography demonstrated a right sub-areolar mass measuring 10.8 mm x 6.4 mm, characterised as a Breast Imaging-Reporting and Data System (BI-RADS) 4 lesion (suspicious for malignancy). No suspicious axillary ade-nopathy was noted. The skin and nipple appeared normal (Figure 1A). Breast ultrasound reported an oval, well-defined, hypoechoic right sub-areolar nodule.
A core needle biopsy of the lesion showed a neoplasm consisting of spindle cells with smooth muscle differentiation and no mitotic activity, atypia or areas of necrosis, in keeping with a benign leiomyoma.
An excision biopsy of the mass without a margin was performed (Figure 1B). Histology showed a moderately cellular spindle cell proliferation with a fascicular growth pattern (Figure 2A). The neoplasm was unencapsulated, with a well-circumscribed border. The cells had abundant eo-sinophilic cytoplasm and central elongated, uniform nuclei. The spindle cells showed positive cytoplasmic staining with smooth muscle actin (SMA) (Figure 2B), which is present in myoepithelial cells, smooth muscle cells and myofibroblasts.
In light of the histological findings, the presence of SMA may have suggested smooth muscle proliferation (i.e., leiomyoma) or a reactive myofibroblastic proliferation. The presence of h-caldesmon staining, which identifies muscle specific contractile proteins specific to smooth muscle cells, not present in myofibroblasts, confirmed a smooth muscle proliferation rather than a myofibroblastic proliferation. This, together with the histological findings, is consistent with a benign leiomyoma.
Discussion
Leiomyomas are benign mesenchymal tumours composed of smooth muscle tissue and account for the majority of mesenchymal neoplasms of the gastrointestinal tract and uterus.1 Breast leiomyomas are extremely rare and represent less than 1% of all breast neoplasms. Only a few cases have been reported in the literature.13 Most breast leiomyomas occur sub-areola in both males and females, and present as small to medium-sized painless lumps.2,4,5 Breast leiomyomas have also been described on the breast skin and intra-parenchymal in the breast.6
In addition to the history and clinical examination, diagnosis of breast leiomyomas requires radiological, his-topathological and immunohistochemical studies to identify lesions as well as to guide management.1 The patients are usually asymptomatic; however, symptoms such as pruritus, increased breast volume, pain and hardening of the nipple or nodule have been reported.7 Our patient developed a small nodule in the sub-areolar area which remained unchanged for six years.
Mammography and ultrasound provide an important radiological assessment tool, whereas tissue biopsy analysis is required to make a definitive diagnosis. Mammography typically demonstrates homogenous dense lesions with well-defined margins without micro-calcifications.6 Of note, in our patient the mammographic features suggested a suspicious lesion. On ultrasound, lesions appear as solid, non-cystic homogenous circumscribed nodules.8 Magnetic resonance imaging can also be used to aid diagnosis.9
Breast leiomyomas share similar histologic and immunophenotypic features as leiomyomas found at other sites.10 Using immunohistochemical staining, leiomyomas are positive for desmin, SMA and h-caldesmon.5 Although myofibroblastic proliferations often show positivity with SMA, the presence of h-caldesmon staining confirms smooth muscle origin rather than a myofibroblastic proliferation.
Management of breast leiomyomas is usually surgical and involves simple enucleation of the lump. Notwithstanding the fact that the biological behaviour of these neoplasms has not been fully elucidated, recurrence is rare.5,7
These rare breast lesions tend to be non-aggressive and indolent. We wish to highlight their existence in order to permit proper assessment and management when they are encountered in surgical practice.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding was required.
Ethical approval
Ethical approval was obtained from the Human Research Ethics Committee of the University of the Witwatersrand (clearance certificate no M210568) and the research review board of Helen Joseph Hospital.
ORCID
W Ngwisanyi https://orcid.org/0000-0002-7675-6360
G Tshimbidi https://orcid.org/0000-0002-2316-3262
M Keyter https://orcid.org/0000-0003-1158-5641
C-A Benn https://orcid.org/0000-0002-4777-4316
REFERENCES
1. Sampaio GP, Koch MV, Boechat M, Matos VE, Dos Santos AA. Leiomyoma of the breast: an uncommon tumour. Radiol Bras. 2016;49(5):343-4. https://doi.org/10.1590/0100-3984.2014.0136. [ Links ]
2. Kafadar MT, Yalfin M, Gok MA, et al. Intraparenchymal leiomyoma of the breast: a rare location for an infrequent tumour. Eur J Breast Health. 2017;13(3):156-8. https://doi.org/10.5152/ejbh.2017.3472. [ Links ]
3. Goncalves I, Ventura N, Valente T, et al. Unanticipated diagnosis - intraparenchymal leiomyoma of the breast: case report. Int Surg J. 2020;8(1):368. https://doi.org/10.18203/2349-2902.isj20203905. [ Links ]
4. Pourbagher A, Pourbagher MA, Bal N, Oguzkurt L, Ezer A. Leiomyoma of the breast parenchyma. AJR Am J Roentgenol. 2005;185(6):1595-7. https://doi.org/10.2214/AJR.04.1453. [ Links ]
5. Granic M, Stefanovic-Radovic M, Zdravkovic D, et al. Intraparenchimal leiomyoma of the breast. Arch Iran Med. 2015;18(9):608-12. [ Links ]
6. Ende L, Mercado C, Axelrod D, et al. Intraparenchymal leiomyoma of the breast: a case report and review of the literature. Ann Clin Lab Sci. 2007;37(3):268-73. [ Links ]
7. Kotsuma Y, Wakasa K, Yayoi E, et al. A case of leiomyoma ofthe breast. Breast Cancer. 2001;8(2):166-9. https://doi.org/10.1007/BF02967498. [ Links ]
8. Munitiz V, Rios A, Canovas J, et al. Primitive leiomyosarcoma of the breast: case report and review of the literature. Breast. 2004;13(2):72-76. https://doi.org/10.1016/j.breast.2003.09.004. [ Links ]
9. Cho HJ, Kim SH, Kang BJ, et al. Leiomyoma of the nipple diagnosed by MRI. Acta Radiol Short Rep. 2012;1(9):arsr.2012.120025. https://doi.org/10.1258/arsr.2012.120025. [ Links ]
10. Diaz-Arias AA, Hurt MA, Loy TS, Seeger RM, Bickel JT. Leiomyoma of the breast. Hum Pathol. 1989;20(4):396-9. https://doi.org/10.1016/0046-8177(89)90052-X. [ Links ]
 Correspondence:
Correspondence:
W Ngwisanyi
Email: sisludongwis@gmail.com

{kind=link}
{kind=link}