










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151Print version ISSN 0038-2361
S. Afr. j. surg. vol.62 n.3 Cape Town 2024
https://doi.org/10.36303/SAJS.00163
LOWER GIT SURGERY
The accuracy of white cell count and C-reactive protein in diagnosing acute appendicitis at a tertiary hospital
N Tshuga; VC Ntola; R Naidoo
Department of Surgery, Nelson R Mandela School of Clinical Medicine, College of Health Sciences, University of Kwazulu-Natal, South Africa
ABSTRACT
BACKGROUND: Diagnostic accuracy in acute appendicitis (AA) may be improved by using inflammatory markers. This study assessed the reliability of inflammatory markers in diagnosing AA in our patient population.
METHODS: A retrospective cross-sectional study was conducted at King Edward Hospital (KEH) from January 2020 to June 2021. Data was collected on all patients with AA who underwent appendicectomy. Variables of age, gender, comorbidities, HIV status Alvarado score histology, C-reactive protein (CRP), and white cell count (WCC) were reviewed. A p-value of < 0.05 is deemed as statistically significant.
RESULTS: The study cohort was comprised of 150 patients - 58(39%) females and 92(61%) males. Thirty-two (21.3%) patients had a normal appendix, of whom 19 had a normal WCC. The majority of patients 80 (53.3%) had inflamed appendix, and 38 (25.3%) had ruptured appendix. The sensitivity and specificity of WCC and the CRP were 81% and 46% and 100% and 18.6% respectively. No patient with a ruptured appendix had normal CRP. The CRP correlated with the ruptured appendix with a median of 141.5 and, p-value of 0.01. The level of WCC and the presence of a ruptured appendix had a significant correlation with a p-value of 0.002, median of 15.2.
CONCLUSION: A combination of WCC and CRP tests improves the diagnostic accuracy. There is a correlation between CRP level and ruptured appendicitis. In our setting, AA is likely to present late once it has already ruptured. The reasons behind this late presentation need to be explored and addressed.
Keywords: acute appendicitis, inflammatory markers, surgical emergency
Introduction
Acute appendicitis (AA) is the most common abdominal non-trauma surgical emergency and often the most challenging to diagnose.1 Worldwide AA remains the most common intra-abdominal condition requiring surgical intervention. There is a noted steady decline in the incidence of appendicitis since the 1940s. Annually, up to 250 000 cases of appendicectomies are reported in the US, with an estimated lifetime risk of 7%. The overall lifetime risk of developing AA is 8.6% for males and 6.7% for females.1 In Africa, the lifetime risk is 2% as compared to the USA at 9% and Europe at 8%.2 It occurs most commonly between the ages of 10-30 years, with a male preponderance.1
The majority of patients with AA typically present with right iliac fossa pain, nausea or vomiting, and fever. These are nonspecific symptoms, which can be mimicked by various other pathologies.1 The diagnosis is largely based on clinical grounds. To improve diagnostic accuracy, clinicians rely on a good history and sound clinical examination augmented by laboratory investigations which include white cell count (WCC) and C-reactive protein (CRP) levels; however, both these inflammatory makers are non-specific. The negative appendicectomy rate is estimated to be around 10%.3 CRP was identified in 1930 and regarded as an acute-phase protein that has been studied as a screening tool for inflammation. Within 4 to 6 hours of the tissue insult, there is noted production of CRP with a peak sensitivity at 24 to 48 hours after the onset of the inflammatory event.4 WCC and CRP are simple laboratory tests that are cheap, readily available, and carried out routinely. However, various studies conducted to evaluate their role in improving the diagnostic accuracy of AA remain equivocal.
Advances in imaging in computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound (US) have shown improvement in diagnosing AA; each modality comes with its advantages and disadvantages - increasing radiation exposure associated with CT has been shown to increase lifetime risk for cancer especially in the paediatric population and contrast induced nephropathy1,5,6,7 and some of this imaging is not available after hours or in all hospitals.7 A South African systemic review by Yang et al. that looked at the studies done on appendicitis in South Africa found a trend in a delayed presentation in South Africans as a whole as compared to other developing countries. This led to higher perforation rate (36%).6,7 Contributary factors to this phenomenon included, poor socioeconomic conditions, health systems weakness, the use of traditional medicine, rural origin and lastly lack of awareness. Madiba et al. found that 43% of patients had perforated appendicitis.8-11 Late presentation or failure to diagnose and correctly manage this condition may lead to appendiceal perforation which is associated with increased cost, longer hospital stay, higher morbidity and mortality.
Objective
To evaluate the accuracy of clinical examination and inflammatory markers in diagnosing AA, in relation to the histological findings in our patient population.
Patients and methods
This was a retrospective observational descriptive study that used patients' chart reviews. The medical records of patients who underwent appendicectomy from January 2020 to June 2021 were reviewed. The preoperative laboratory results from admission and histology results were retrieved from our local laboratory and recorded. All patients who had clinical and imaging findings suggestive of appendicitis and underwent appendicectomy with CRP, WCC, and histology results available on National Health Laboratory Services (NHLS) were included in the study. Both adults and children were included, irrespective of age. Exclusion criteria were patients with no blood and histology results and incomplete medical records with no inpatient numbers to trace results on the NHLS website. Patients who underwent interval appendicectomy after non-operative management, and those with proven malignancy on histology, missing blood, and histology results were not included nor followed up in the study. This study compared the WCC and CRP done on admission before appendicectomy and their respective histopathological findings.
Statistical analysis and model
Continuous data were summarised using medians and interquartile ranges. Kruskal-Wallis tests were used to compare histology types and box plots used to display the data. The association between demographic and clinical risk factors with histology was examined using chi-square tests or Fisher's exact tests. WCC and CRP were also dichotomised into high and low. Using histology as the gold standard, sensitivity, specificity, negative and positive predictive values are presented for different combinations of WCC and CRP. Youden's index was used to establish the optimum cut-off point for estimating a ruptured appendix. Stata V17 statistical software was used for the analysis. Ethical approval for the study was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (BE3931/2022) and permission to conduct the study was obtained from the Hospital Research Review Board.
Results
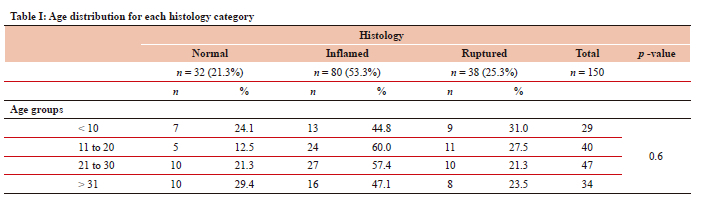
A total of 252 patients underwent appendicectomy between January 2020 and June 2021. A total number of 150 patients met our inclusion criteria; of these patients, 92 were males and 58 females. Patients were grouped according to age, with an age range between 4-61 years and a median age of 22.0. The age group with the highest number of patients was 21-30 years (n = 47, 31.3%) and the age group with the lowest number of patients was above 60 years, which was only 1 (0.7%) patient. It was noted that above the age of 30 years, the number of patients decreases (Table I). In our patients' cohort, 22 patients were retroviral disease (RVD) reactive, 5 patients had diabetes mellitus, and 2 patients had pulmonary tuberculosis. Imaging was done on 23 patients (12 ultrasound and 11 contrasted CT abdomen).
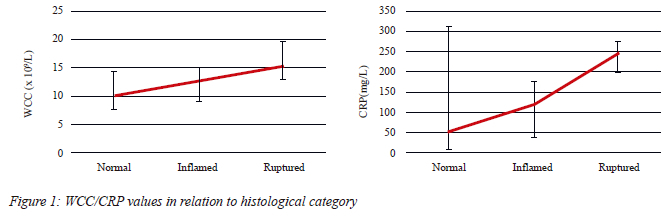
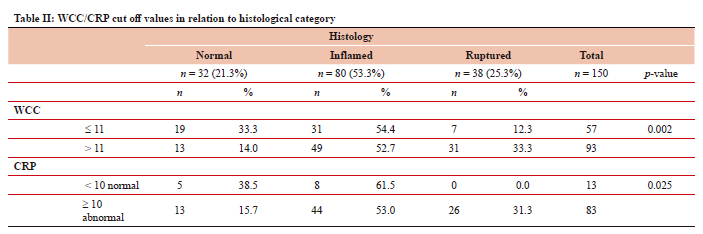
Histological findings were classified into three categories - inflamed, which occurred in 80 cases, ruptured in 38 cases and 32 patients were found to have histological normal appendix. We analysed the CRP and WCC to assess its sensitivity in diagnosing appendicitis, both combined and in isolation. All our patients had WCC, 96 patients had both WCC and CRP, and 54 patients had no CRP results. The median WCC was 12.9 x 10A9/L (IQR: 9.22-15.8, min 4.0), and the median for CRP was 141.5 mg/L (IQR: 242, min 9) (Figure 1). The WCC was raised in 93 cases - histologically normal appendix 13 (40.6%), inflamed 49 (61.3%), ruptured 31 (81.6%). It was below normal in 57 patients - histologically normal appendix 19 (59.4%), inflamed 31 (38.8%), ruptured 7 (18.4%) (Table II).
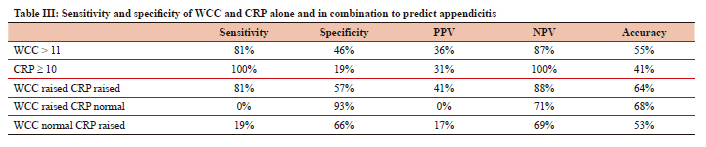
ROC curve analysis, looking at both CRP and WCC to distinguish between ruptured and inflamed appendix, indicates the area under the curve for CRP 0.82 and WCC 0.70, which shows that CRP has a better distinguishing ability than WCC. However, WCC also can be used to categorise rupture. We further analysed CRP and WCC in cases where both were available, using local laboratory cut-off values to assess their sensitivity and specificity in diagnosing appendicitis, both combined and in isolation. WCC > 11 109 cells/l had a sensitivity of 81% and specificity of 46%, p-value 0.002, negative predictive value (NPV) of 86.5%, and positive predictive value (PPV) of 35.6%. CRP > 10 mg/l had a sensitivity of 100% and specificity of 19%, p-value 0.025, NPV 100%, and PPV of 31.3%. When both CRP and WCC were raised - sensitivity of 81% and specificity of 57.1%, p-value of 0.002, NPV of 88.1%, and PPV of 41.2% - the sensitivity and specificity, NPV and PPV were raised as compared to evaluating each value in isolation. Also noted is that when CRP is raised the sensitivity was higher but very low specificity as compared to isolated raised WCC, and these findings were associated with a ruptured appendix (Table III).
The Kruskal-Wallis test was performed to assess the relationship between the raised WCC and CRP in relation to histological findings. The p-value was 0.002, which was statistically significant in WCC when comparing ruptured with inflamed appendix and normal appendix, the median (IQR) was 10.2 for normal appendix, 12.6 and 15.2 for inflamed and ruptured appendix respectively, with a chi-square test of 0.002. The median (IQR) for CRP was 54.5 for normal appendix, 121.5 and 141.5 for inflamed and ruptured appendix respectively, the p-value was 0.9 and the Fisher's exact test was 0.01.
Discussion
AA is a common surgical condition. The current incidence is 5.7 per 100 000 per year with a peak between 10-30.1,2,12 Diagnosis is predominantly clinical and to improve its diagnostic accuracy, several scoring systems have been advocated to aid in early diagnosis and prompt management. CT abdomen and US imaging is not routinely done in our setting as they are not always available, but when in diagnostic doubt the patient is usually booked for a US first; if that is still not conclusive, then a CT is requested. Diagnostic laboratory work-up should include a WCC and CRP routinely in patients with suspected AA, although literature has shown that these inflammatory makers have varying sensitivity and specificity. Different perspective adult cohort studies have shown high sensitivity and specificity of these biomarkers and that has shown to decrease the dependency on imaging to evaluate AA. A South African study by Withers et al. in a paediatric population showed that CRP > 10 mg/l is a strong predictor of AA with a good discriminative power between complicated and uncomplicated AA.4 This is in comparison to our result, which combined both adults and paediatric population and showed that high CRP was associated with ruptured appendicitis; we found higher sensitivity of 100% than WCC and lower specificity of 19%, p-value 0.002. This was statistically significant as raised CRP was associated with a ruptured appendix, the same results were also found in a study done by Van den Worm et al. where they reported greater diagnostic accuracy of the CRP compared to the WCC, with a low specificity of 24.5%.13
The diagnostic value of these markers in AA has been extensively studied and each has been shown to fall short when used as a single diagnostic marker; the combination has been shown to improve diagnostic accuracy. Kim et al. showed that the sensitivity and specificity of the WCC were 66.5% and 66% respectively, and the sensitivity and specificity of CRP were 79% and 59% respectively;14 in comparison to our results which show a high sensitivity of 100% and specificity of 19% for CRP and WCC, 81% and 46% respectively, when CRP and WCC combined and both raised sensitivity 81%, with specificity of 57%, NPV 88.9%. This supported the consensus that inflammatory markers are an important adjunct in the work-up of patients and have shown enhanced sensitivity and accuracy in a patient with suspected AA. Our study found that all patients with ruptured appendix had raised CRP with a median (IQR) 141.5, p-value 0.01, which is higher than a local study by Worm et al. in Capetown.13 These findings we attributed to a lot of factors, such as delayed presentation, as most of our population are from a location with poor socioeconomic status. A normal appendix is likely to have normal CRP; 13 patients had normal CRP and no patient had normal CRP and ruptured appendix. Studies by Sengupta et al. and Khan et al. both found that normal inflammatory markers had a NPV of 100%, allowing AA to be ruled out in these patients.15,16 Whereas Vaughan-Shaw et al. and Yang et al. both found that a small percentage of patients with AA had normal inflammatory markers (5.7% and 1.8%, respectively),7,17-19 and thus AA could not be ruled out based solely on normal inflammatory markers. The clinician should also be cautious when dealing with normal inflammatory makers in patients with clinical suspicion of AA. In a review study by Kim et al. 39.8% of patients had normal WCC and CRP but histologically confirmed AA. This figure is clinically significant emphasising the importance of not only using inflammatory markers to rule out AA. However, our findings also show that about 59.4% normal WCC and 15.6% normal CRP had a histologically normal appendix, NPV of WCC 86.5% and CRP 100%. This confirms that if these inflammatory makers are normal, appendicitis is unlikely.14 There is a significant association between the combined WCC CRP category and histology. Based on this information the combination of these two biomarkers improves their diagnostic power for inflamed and ruptured AA.19 In our study, we found no significant difference in the WCC median between the inflamed appendix and the ruptured appendix. Raised levels in both CRP and WCC increase the likelihood of ruptured appendicitis and their sensitivity and accuracy are improved to 81%, but they cannot be used in isolation; clinical acumen and the addition of imaging are still important adjuncts.
Conclusion
In our setting, CRP and WCC are cheap and easily accessible; these are important adjuncts when there is a clinical suspicion of AA. A combination of WCC and CRP tests improves the diagnostic accuracy of AA; when both are raised, it is likely to confirm appendicitis. However, when both are low this still does not rule out AA, therefore clinicians should not entirely rely on them to exclude AA. We then recommend that all patients with suspected AA have both biochemical markers tested.
Limitations
This is a retrospective study. Further limitations were difficult retrieval of patients' files from the hospital filing system and unavailable important and necessary data in the files including unclear detail on theatre notes. The fact that there was no grading for AA limited the understanding of the severity of the AA in our study.
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
The study protocol was approved by the University of KwaZulu-Natal Biomedical Research Ethics Committee (BE3931/2022) and permission to conduct the study was obtained from the Hospital Research Review Board.
ORCID
N Tshuga https://orcid.org/0000-0003-2667-5375
VC Ntola https://orcid.org/0000-0002-9667-1591
R Naidoo https://orcid.org/0000-0002-1992-5615
REFERENCES
1. Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15(1):1-42. [ Links ]
2. Lamm R, Kumar SS, Collings AT, et al. Diagnosis and treatment of appendicitis: systematic review and meta-analysis. Surg Endosc. 2023;37(12):8933-90. https://doi.org/10.1007/s00464-023-10456-5. [ Links ]
3. Er S, Çomçalı B, Soykurt A, et al. Diagnosis of appendicitis in patients with a normal white blood cell count: A cross-sectional study. Bull Emerg Trauma. 2018;6(2):128. https://doi.org/10.29252/beat-060207. [ Links ]
4. Withers AS, Grieve A, Loeland JA. Correlation of white cell count and CRP in acute appendicitis in paediatric patients. S Afr J Surg. 2019;57(4):40. https://doi.org/10.17159/2078-5151/2019/v57n4a2953. [ Links ]
5. Chang ST, Jeffrey RB, Olcott EW. Three-step sequential positioning algorithm during sonographic evaluation for appendicitis increases appendiceal visualisation rate and reduces CT use. Am J Roentgenol. 2014;203(5):1006-12. https://doi.org/10.2214/AJR.13.12334. [ Links ]
6. Huckins DS, Copeland K, Self W, et al. Diagnostic performance of a biomarker panel as a negative predictor for acute appendicitis in adult ED patients with abdominal pain. Am J Emerg Med. 2017;35(3):418-24. https://doi.org/10.1016/j.ajem.2016.11.027. [ Links ]
7. Yu CW, Juan LI, Wu MH, et al. Systematic review and meta-analysis of the diagnostic accuracy of procalcitonin, C-reactive protein and white blood cell count for suspected acute appendicitis. Br J Surg. 2013;100(3):322-9. https://doi.org/10.1002/bjs.9008. [ Links ]
8. Yang E, Kahn D, Cook C. Acute appendicitis in South Africa: a systematic review. S Afr J Surg. 2015;53(3and4):1-8. [ Links ]
9. Madiba TE, Haffejee AA, Mbete DL, et al. Appendicitis among African patients at King Edward VIII Hospital, Durban, South Africa: a review. East Afr Med J. 1998;75(2):81-4. [ Links ]
10. Atema JJ, Gans SL, Beenem LF, et al. Accuracy of white cell count and c-reactive protein levels related to duration of symptoms in patients suspected of acute appendicitis. Acad Emerg Med. 2015;22(9):1015-24. https://doi.org/10.1111/acem.12746. [ Links ]
11. Kong VY, Sartorius B, Clarke DL. Acute appendicitis in the developing world is a morbid disease. Ann R Coll Surg Engl. 2015;97:390-5. https://doi.org/10.1308/003588415X14181254790608. [ Links ]
12. Kong VY, van der Linde S, Aldous C, Handley JJ, Clarke DL. Quantifying the disparity in outcome between urban and rural patients with acute appendicitis in South Africa. S Afr Med J. 2013;103(10):742-5. https://doi.org/10.7196/SAMJ.7109. [ Links ]
13. Van den Worm L, Georgiou E, De Klerk M. C-reactive protein as a predictor of severity of appendicitis. S Afr J Surg. 2017;55(2):14-7. [ Links ]
14. Kim JJY, Dobson BH, Ng CLH, et al. Can normal inflammatory markers rule out acute appendicitis? The reliability of biochemical investigations in diagnosis. ANZ J Surg. 2020;90(10):1970-4. https://doi.org/10.1111/ans.15559. [ Links ]
15. Sengupta A, Bax G, Paterson-Brown S. White cell count and C-reactive protein measurement in patients with possible appendicitis. Ann R Coll Surg Engl. 2009;91(2):113-5. https://doi.org/10.1308/003588409X359330. [ Links ]
16. Khan MN, Davie E, Irshad K. The role of white cell count and C-reactive protein in the diagnosis of acute appendicitis. J Ayub Med Coll Abbottabad. 2004;16(3):17-9. [ Links ]
17. Vaughan-Shaw PG, Rees JR, Bell E, Hamdan M, Platt T. Normal inflammatory markers in appendicitis - evidence from two independent cohort studies. JRSM Short Rep. 2011;2(5):43. https://doi.org/10.1258/shorts.2011.010114. [ Links ]
18. Siddique K, Baruah P, Bhandari S, Mirza S, Harinath G. Diagnostic accuracy of white cell count and C-reactive protein for assessing the severity of paediatric appendicitis. JRSM short reports. 2011;2(7):1-6. https://doi.org/10.1258/shorts.2011.011025. [ Links ]
19. Dayawansa NH, Segan JD, Yao HH, et al. Incidence of normal white cell count and C-reactive protein in adults with acute appendicitis. ANZ J Surg. 2018;88(6):E539-43. https://doi.org/10.1111/ans.13760. [ Links ]
 Correspondence:
Correspondence:
email: noztshuga@yahoo.com

{kind=link}
{kind=link}
{kind=link}
{kind=link}