










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151Print version ISSN 0038-2361
S. Afr. j. surg. vol.62 n.4 Cape Town 2024
https://doi.org/10.36303/SAJS.00168
ENDOCRINE SURGERY
Experience of a tertiary/quaternary unit with surgery for endocrine hypertension
I Bombil; RA Muganza; R Netshamutsindo
Department of Surgery, School of Clinical Medicine, Chris Hani Baragwanath Academic Hospital, University of the Witwatersrand, South Africa
ABSTRACT
BACKGROUND: Endocrine hypertension is believed to be underestimated worldwide especially in the developing countries. There is a scarcity of publications on endocrine hypertension in sub-Saharan Africa. The aim of this study was to reflect the profile of patients with endocrine hypertension of adrenal/paraganglioma origin at Chris Hani Baragwanath Academic Hospital (CHBAH). The objective was to determine the aetiology, the lead time to diagnosis of endocrine hypertension and to reflect on the surgical approach and outcome.
METHODS: This descriptive observational study reviewed all surgical procedures performed at CHBAH from 1 January 2013 to 31 December 2020. Parameters analysed included the demographics, the aetiologies, the location of the disease, the surgical approach, the histopathology, the incidence of malignancy, the lead time and the 30-days outcome.
RESULTS: Of the 44 patients analysed, there were 66% female and 34% male. The mean age was 38 years. The majority of the cases were due to catecholamine secreting tumours (65.9%). Overall, 43.1% of the procedures were completed laparoscopically. Altogether, the mean lead time ranged from 5 to 12 years. The incidence of malignancy and the 30-day mortality were 15.9% and 4.5% respectively. The index presentation of endocrine hypertension was due to complications in 9% of the cases.
CONCLUSION: Catecholamine producing tumours were the most common aetiology. Laparoscopy was successful in 43.1%. The lead time was long and there were more tumours on the left side. The mortality rate was 4.5%.
Keywords: endocrine hypertension, South Africa, adrenalectomy
Introduction
Hypertension is one of the most common chronic medical conditions. In the majority of cases, the aetiology is unknown and is labelled "essential hypertension".1 Although an endocrine aetiology is rare, we believe that the incidence may be underestimated worldwide especially in low-to middle-income countries. The literature is scarce in sub-Saharan Africa with some publications reported from Cape Town and Johannesburg in South Africa.2'3'4 Selective screening of young patients, those with newly diagnosed hypertension and patients on three or more anti-hypertensive drugs is beneficial to enable early diagnosis of endocrine hypertension.5 Regardless of aetiology, hypertension has systemic repercussion on the target organs that affects the quality of life if undiagnosed.
Early detection is likely to prevent irreversible structural damage to the kidney that will perpetuate the hypertension even when the underlying pathology is eventually dealt with. Surgery is the definitive treatment of endocrine hypertension obviating the need for chronic anti-hypertensive medications in some cases. The most common cause of endocrine hypertension is primary hyperaldosteronism.6
In this study, we reviewed all surgical procedures performed for endocrine hypertension of adrenal/paraganglioma origin at Chris Hani Baragwanath Academic Hospital (CHBAH) to reflect the disease profile. The primary aim was to establish the aetiology of endocrine hypertension seen at CHBAH, the lead time to diagnosis of endocrine hypertension and the surgical approaches. The secondary aim was to determine the incidence of malignancy and the 30-day mortality. We hypothesise that patients who made it to surgery may only represent the tip of the iceberg.
Methods
This was a descriptive observational study which retrospectively analysed all surgical procedures performed for endocrine hypertension at CHBAH from 1 January 2013 to 31 December 2020. Parameters analysed included patient demographics, aetiology of endocrine hypertension, location of the disease, surgical approach, histopathological report, incidence of malignancy, delay from the onset of hypertension to the diagnosis of endocrine aetiology (lead time) and the 30-day postoperative mortality. Continuous variables were presented as mean for normal distribution or as median for data not normally distributed, whereas categorical variables were expressed as frequencies (numbers, proportion, or percentage). Patients who underwent laparoscopic adrenalectomy not associated with hypertension (one benign mesothelial cyst and two non-secreting adenoma) were excluded. Ethical approval was obtained from the Human Ethics Committee of the University of the Witwatersrand and the research review board of CHBAH (clearance certificate No. M211044).
Results
The data of 44 patients were analysed. There were 16 male (36.3%) and 28 female (63.6%) patients with a male to female ratio of 1:2. The mean age was 38 years ranging from 13 to 71 years. There were 42 black (95.4%) patients.
In terms of laterality, 65.9% (29/44) and 43.1% (19/44) of tumours were located on the left and right side, respectively.
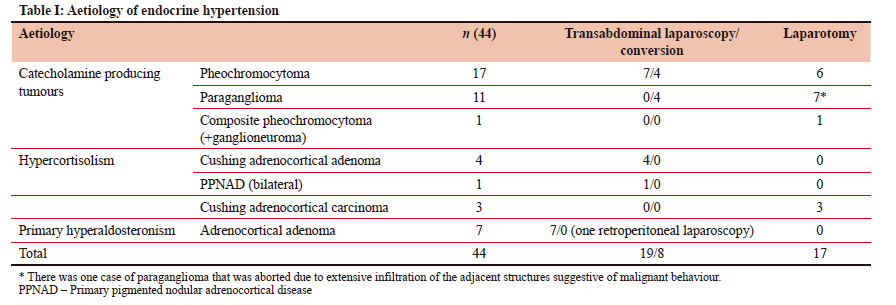
Table I summarises the aetiology of endocrine hypertension in the 44 patients.
There were 29, 8 and 7 cases of catecholamine secreting tumours, hypercortisolism and hyperaldosteronism respectively.
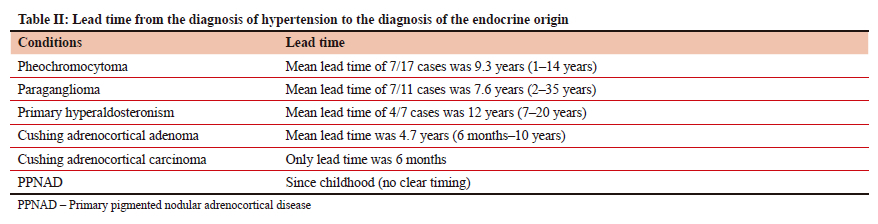
Table II describes the lead time from the diagnosis of hypertension to the diagnosis of the endocrine origin, which was 9.3, 7.6, 12 and 4.7 years respectively for pheochromocytoma, paraganglioma, hyperaldosteronism and Cushing adenoma.
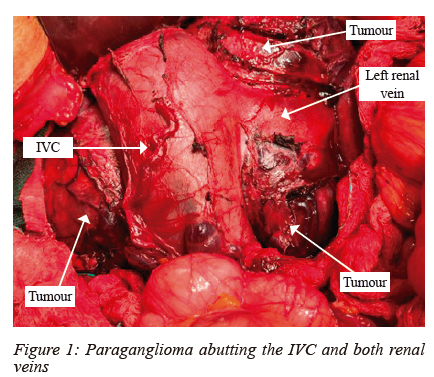
Overall, 43.1% (19/44) of the procedures were completed laparoscopically. Of the 27 cases eligible for laparoscopy, 70.3% (19/27) were completed successfully and 29.6% (8/27) were converted to laparotomy. All conversions were via a subcostal incision except in one patient where a right thoracotomy was indicated for an intrathoracic paraganglioma that was reported on computed tomography scan (CT scan) as a right adrenal mass. The 17 planned laparotomies were via a midline incision (Figure 1).
In four patients (13.7%) complications of catecholamine secretion led to the diagnosis of four of the catecholamine secreting tumours. A transient ischaemic attack (TIA) and catecholamine crisis were each caused by a paraganglioma. A cerebrovascular accident (CVA) and profuse diarrhoea were related to pheochromocytomas one of which was a composite pheochromocytoma associated with ganglioneuroma. The patient with a catecholamine crisis was a 34-year-old female with no comorbidity, who presented as an emergency and was admitted to the intensive care unit (ICU) with multi-organ dysfunction of unknown origin. The incidental finding of paraganglioma on ultrasound prompted the work up that confirmed catecholamine secreting tumour. Preoperatively she developed gangrene of both lower limbs that resulted in bilateral below knee amputation at the same setting with the excision of the paraganglioma. The intraoperative finding was not suggestive of a malignancy and on histopathological report the PASS (pheochromocytoma of the adrenal gland scaled score) score was 1/20, suggestive of benign tumour. Postoperative recovery was uneventful.
Prior to surgery, one out of 7 cases of primary hyperaldosteronism had a TIA.
The incidence of hypertension-related complications was 11.3% (5/44), of which 9.0% (4/44) contributed to the diagnosis of endocrine hypertension.
All 7 open cases of pheochromocytoma, including the composite pheochromocytoma, were due to big size (> 8 cm). Three exhibited malignant behaviour evidenced by local infiltration of the inferior vena cava (IVC) and the 4 conversions from laparoscopy were due to bleeding.
Bilateral pheochromocytomas were noted in two patients and one pheochromocytoma was associated with hyperparathyroidism without goitre and with a normal calcitonin level.
There was one other patient with three tumours (bilateral pheochromocytoma and an infrarenal paraganglioma along the right sympathetic chain) who recovered well post-surgery.
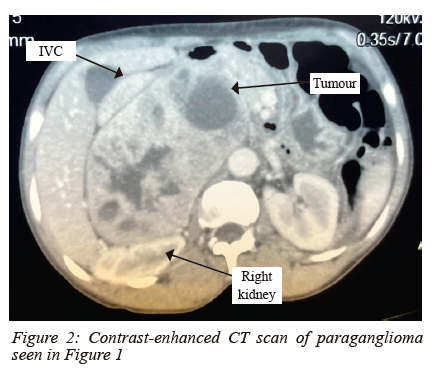
Of the 11 paragangliomas, 7 were not candidates for laparoscopy (Figures 1 and 2) and 4 were converted to laparotomy.
The diagnosis of endocrine hypertension was made incidentally in 13.6% (6/44) patients - three with a pheochromocytoma, one with a paraganglioma and two with an adrenocortical carcinoma.
The catecholamine producing tumours exhibited the classic response of hypotension post excision and benefited from inotropic support postoperatively for no longer than 24 hours.
All cases of hyperaldosteronism had small tumours (1.5-3 cm).
The three Cushing adrenocortical carcinomas were large tumours weighing more than 1000 mg with the mean largest diameter of 150 mm.
The diameter of the catecholamine producing tumours ranged from 50 to 200 mm.
Two patients with adrenocortical carcinoma (4.5%) died within 30 days; one from brain metastasis and the other from sepsis. Three patients (6.8%) required a relook laparotomy due to bleeding - two patients with pheochromocytoma and one patient with paraganglioma.
The incidence of malignancy based on intraoperative findings and imaging was 15.9% (7/44).
Discussion
The 44 cases of endocrine hypertension over an 8-year period may seem insignificant in comparison to all causes of hypertension.
However, the emphasis was rather on the correctable nature of this condition that needed to be identified and treated early to minimise the complications of hypertension that can be fatal. Awareness of endocrine hypertension especially in the African population is of utmost importance to raise a high index of suspicion and to be considered in the differential diagnosis of the causes of hypertension especially in young patients as reflected in Huddle's audit of 54 black patients over 30 years at CHBAH in Johannesburg.4
It is important to highlight the long lead time in the diagnosis of endocrine hypertension. This may be a reflection of the scarcity of endocrinologists, the lack of awareness by the general practitioners and possibly the inadequate work-up of newly diagnosed hypertension.
The management of endocrine hypertension is straightforward and depends on the underlying aetiology.
It starts with screening of the suspected group of patients followed by confirmation of the diagnosis and eventually the localisation.5
The relatively shorter lead time in hypertension caused by hypercortisolism may be due to the obvious clinical picture from the onset. The hyperaldosteronism aetiology has the longest lead time presumably because it is often clinically asymptomatic. Even on biochemistry, the hypokalemia is not an early finding and is only present in about 50% of the cases.5
The catecholamine producing tumours were the most common (65.9%), contrary to the literature that is in favour of hyperaldosteronism as the most common cause of endocrine hypertension.6 This may be due to the underdiagnosis of the hyperaldosteronism cases due to the lack of obvious symptoms beside hypertension. Conradie et al. from Tygerberg Hospital had an almost even number of patients with hyperaldosteronism, catecholamine secreting tumours and hypercortisolism that were 7, 6 and 6 respectively.3 This finding is different from the literature and our study.
The 13.7% of catecholamine producing tumours that presented with complications were not significantly higher than the 11% reported in the literature.7
The 6.8% incidence of bilateral disease in catecholamine producing tumours was less than the underestimated 10% reported in the literature.8
The one case of composite pheochromocytoma reflected the rarity of this subgroup and it is not clear whether the neuroblastic component does alter the outcome.9,10 The multiple endocrine neoplasia (MEN 2) was noted in one case of pheochromocytoma associated with parathyroid adenoma.
The patient with triple tumours fared better than the one who had one paraganglioma complicated with catecholamine crisis that resulted in bilateral gangrene of lower limb.
It is not clear why this particular patient behaved in such an aggressive manner since neither the intraoperative findings nor the histopathological report suggested aggressive behaviour, nor did she have any underlying comorbidity.
There are few cases of catecholamine crisis reported in the literature and most of them were not associated with malignancy.11 The age of the reported cases ranged from 33 to 76 years with half of the cases below 45 years; this does not suggest an underlying vasculopathy.11 Our patient was a young adult. We are not aware of any genetic link to a catecholamine crisis, and we are unable to comment on the genetic profile of our patient as this was not done. Catecholamine crisis is a rare, dire endocrine emergency with a mortality rate of around 15% caused by sudden, excessive release of catecholamines.11,12 The pathophysiology behind this surge of catecholamines is unknown.11 The patient who survived lives with a disability that could have been avoided with early diagnosis.
We did not encounter any publications that mentioned the lead time to the diagnosis of endocrine hypertension to compare with our study. Because of the paucity of signs at presentation, we posit that the lead time is long worldwide. This needs to be proven with a multi-centre prospective study.
The fact that only about half of the cases (43.1%) were eligible for laparoscopy can be explained by an underlying malignancy in 15.9% of cases, the late diagnosis, and the higher incidence of catecholamine producing tumours. Beside the catecholamine secreting tumours, all other tumours eligible for laparoscopy had a 100% laparoscopic success rate. Possible explanation is the large size and the hypervascularity of the catecholamine secreting tumours as well as the learning curve.
Furthermore, paragangliomas are often challenging to excise via laparoscopy due to their unpredictable blood supply, altered anatomy and the vicinity of major vasculature.13
Nel et al. from Groote Schuur Hospital in Cape Town had a male to female ratio of 1:3 that is similar to our study and completed 55% of the cases laparoscopically but in their series all cases were due to catecholamine secreting tumours.2
Although rare, the adrenocortical carcinoma is the most aggressive endocrine malignancy and is associated with poor prognosis.14
The limitation of the study was its retrospective nature with expected missing data, the small number of cases and the unknown cases that were not referred to surgery.
Conclusion
Catecholamine producing tumours were the most common endocrine pathology in our institution. Overall, the lead time to diagnosis of the endocrine hypertension was long and ranged from 5 to 12 years. Only 43.1% of procedures were completed laparoscopically, mostly due to the high incidence of large catecholamine secreting tumours. Overall, 15.9% of patients were found to harbour a malignancy. The 30-day mortality was 4.5% and occurred in two of the three patients with adrenocortical carcinoma.
Recommendation
We believe that raising awareness of endocrine hypertension will enforce the selective screening of newly diagnosed patients with hypertension, young hypertensive patients and those on three or more anti-hypertensive agents.
We suggest that all incidental adrenal mass discovered on imaging be referred to the endocrinologist for work-up.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding source to be declared.
Ethical approval
Ethical approval was obtained from the Human Research Ethics Committee of the University of the Witwatersrand and the research review board of CHBAH (clearance certificate No. M211044).
ORCID
I Bombil https://orcid.org/0000-0002-4819-0785
RA Muganza https://orcid.org/0000-0001-5832-6095
R Netshamutsindo https://orcid.org/0000-0003-0706-0092
REFERENCES
1. Vallee A, Safar ME, Blacher J. Essential hypertension: Definitions, haemodynamic, clinical and therapeutic review. Presse Med. 2019;48(1 Pt 1):19-28. https://doi.org/10.1016/j.lpm.2018.11.017. [ Links ]
2. Nel D, Panieri E, Malherbe F, Steyn R, Cairncross L. Surgery for pheochromocytoma: A single-centre review of 60 cases from South Africa. World J Surg. 2020;44(6):1918-24. https://doi.org/10.1007/s00268-020-05420-6. [ Links ]
3. Conradie W, Conradie M, Geldenhuys E, et al. Retroperitoneoscopic adrenalectomy: Introducing a new surgical technique in South Africa. S Afr J Surg. 2023;61:1-6. https://doi.org/10.36303/SAJS.3836. [ Links ]
4. Huddle KR. Pheochromocytoma in black South Africans: A 30-year audit. S Afr Med J. 2011;101:184-8. https://doi.org/10.7196/SAMJ.4320. [ Links ]
5. Koch C, Papadopoulou-Marketou N, Chrousos GP. Overview of endocrine hypertension. [Updated 2020 Feb 4]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278980/. [ Links ]
6. Thomas RM, Ruel E, Shantavasinkul PC, Corsino L. Endocrine hypertension: An overview on the current etiopathogenesis and management options. World J Hypertens. 2015;5(2):14-27. https://doi.org/10.5494/wjh.v5.i2.14. [ Links ]
7. Riester A, Weismann D, Quinkler M, et al. Life-threatening events in patients with pheochromocytoma. Eur J Endocrinol. 2015;173(6):757-64. https://doi.org/10.1530/EJE-15-0483. [ Links ]
8. LamAKY. Update onparagangliomasandpheochromocytomas. Turk Patoloji Derg. 2015;31(Suppl):105-12. https://doi.org/10.5146/tjpath.2015.01318. [ Links ]
9. Garcia AT, Ramírez Plaza CP, Ruiz Diéguez P, Marín Camero N, Santoyo Santoyo J. Ganglioneuroma as an uncommon cause of adrenal tumour. Endocrinol Nutr. 2011;58(8):443-6. https://doi.org/10.1016/j.endoen.2011.02.005. [ Links ]
10. Mylonas KS, Schizas D, Economopoulos KP. Adrenal ganglioneuroma: What you need to know. World J Clin Cases. 2017;5(10):373-7. https://doi.org/10.12998/wjcc.v5.i10.373. [ Links ]
11. Barbara-Batallera E, Del Rosario FM, Mendez-Suareza L, Aleman-Sancheza C, Henriquez MS. Acral ischemia secondary to pheochromocytoma. CIR ESP. 2018;96(9):587-97. https://doi.org/10.1016/j.cireng.2018.10.007. [ Links ]
12. Ando Y, Ono Y, Sano A, et al. Clinical characteristics and outcomes of pheochromocytoma crisis: A literature review of 200 cases. J Endocrinol Invest. 2022;45:2313-28. https://doi.org/10.1007/s40618-022-01868-6. [ Links ]
13. Xu W, Li H, Ji Z, et al. Retroperitoneal laparoscopic management of paraganglioma: A single institute experience. PloS One. 2016;11(2):e0149433. https://doi.org/10.1371/journal.pone.0149433. [ Links ]
14. Scollo C, Russo M, Trovato MA, et al. Prognostic factors for adrenocortical carcinoma outcomes. Front Endocrinol. 2016;7:99. https://doi.org/10.3389/fendo.2016.00099. [ Links ]
 Correspondence:
Correspondence:
email: ifongobombil@gmail.com

{kind=link}
{kind=link}