










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151Print version ISSN 0038-2361
S. Afr. j. surg. vol.63 n.3 Cape Town 2025
https://doi.org/10.36303/SAJS.02270
CASE REPORT
Colonic obstruction secondary to trauma induced intramural haematoma: a rare case report
KS MöllerI; E GeorgiouI; Y GurdayalII
IPaarl Provincial Hospital, South Africa
IINational Health Laboratory Services, Tygerberg Hospital, South Africa
SUMMARY
We report an unusual case of complete bowel obstruction as a result of an intramural haematoma (IMH) in the ascending colon, resulting from blunt abdominal trauma. The patient presented with acute abdominal pain, nausea and vomiting, preceded by four days of constipation, obstipation and worsening abdominal distention. Symptoms were preceded by a history of sustaining a kick to the abdomen during an altercation. Explorative laparotomy was performed, revealing an obstructing ascending colon mass, where a right hemicolectomy and primary anastomosis was performed. Histology confirmed the mass to be an IMH.
Keywords: intramural, bowel obstruction, blunt trauma, colonic, haematoma
Case report
A 31-year-old male presented to the emergency department with a four-day history of worsening abdominal pain associated with nausea, vomiting, constipation and obstipation. The patient had no comorbidities, was not on any medication, reported no constitutional symptoms and had no history of abdominal surgery.
He had normal vital signs (blood pressure 118/76 mmHg and heart rate 78 beats per minute), was apyrexial (temperature 36.8oC) and not hypoxic (saturation 98% on room air). Clinically the abdomen was distended with generalised tenderness maximal in the right iliac fossa and right flank. There were no hernias and rectal examination was normal.
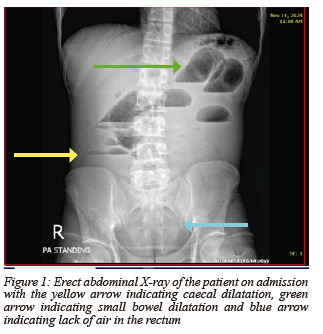
Blood gas revealed a normal lactate of 0.8 mmol/l (0.6-1.7 mmol/l) with a mild metabolic alkalosis (pH 7.464, range 7.38-7.44 and serum bicarbonate of 25.8 mmol/l, range 21-28 mmol/l). Serum creatinine was at 81 μmol/l, but there was a slight hyponatraemia of 131 mmol/l (136-145 mmol/l). The white cell count and C-reactive protein were both normal at 9.30 x 10 9 /l (4.4-11 x 10 9 /l) and 7 mg/l (< 10mg/l) respectively. Platelet count was also assessed as normal at 351 x 10 9 /l (171-388 x 10 9 /l). Erect chest X-ray revealed no free air under the diaphragm, while supine and erect abdominal x-rays revealed extensive small bowel obstruction as well as lack of air in the colon and rectum (Figure 1).
Due to the complete level of obstruction without an apparent cause, and the lack of computer tomography after hours at our facility, the patient was taken to theatre for an explorative laparotomy. Intraoperatively a large obstructing mass was noted in the mid ascending colon with proximal dilatation. No perforation or contamination was associated with the obstructing colon mass. A right hemicolectomy with primary anastomosis was performed, and the patient was transferred to the general surgical ward postoperatively.
The provisional histological result was that of an intramural haematoma (IMH) splitting the muscularis layer, with no features of malignancy, granulomas or inflammation. On further evaluation, the patient confirmed that he had sustained blunt abdominal trauma from a kick to the abdomen, due to an altercation the day before the onset of his symptoms.
The patient was discharged home six days postoperatively. He was followed up three weeks later for review of the final histology result and had made a full recovery with no associated wound complications.
The final histology reported an intramural haemorrhagic mass, measuring 50 x 45 x 30 mm, located in the ascending colon. The mass was identified 110 mm from the proximal resection margin and 120 mm from the distal resection margin. No macroscopic evidence of a tumour was identified at gross assessment of the sample.
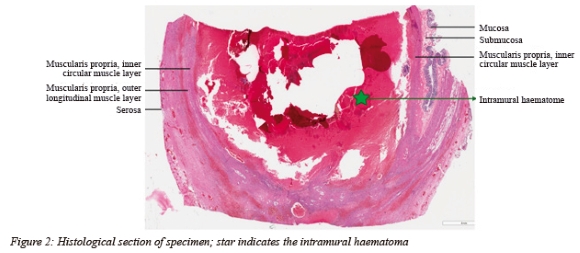
Microscopic evaluation revealed a large haematoma localised within the muscularis propria, intersecting the inner circular muscle layer of the muscularis propria. The haematoma lacked features of organisation and bacterial colonisation. Adjacent fibrin thrombi were not identified. No evidence of dysplasia or invasive malignancy were identified and evaluation of the accompanying lymph nodes demonstrated only reactive changes.
Further evaluation of the background large bowel revealed viable resection margins. Concomitant bacterial, viral and parasitic organisms, granulomatous inflammation, polyposis and dysplasia were not identified on the evaluated sections (Figure 2).
Discussion
Bowel obstruction results in the blockage of flow through the lumen of the bowel, occurring in both small bowel and large bowel. The most common causes of bowel obstruction include adhesions after prior abdominal surgery, hernias, malignant tumours or strictures, and benign inflammatory strictures resulting from conditions such as diverticulitis, ulcerative colitis and Crohn's disease.1
Large bowel obstruction (LBO) constitutes up to 25% of all the cases of bowel obstruction and holds significant challenges for the treating surgeon. It contributes to around 4% of emergency admissions and often results in higher morbidity and mortality due to a delay in the diagnosis.2,3 Many unusual causes of LBO attributed to infection, gallstones, foreign bodies/objects, intussusception, iatrogenic causes, congenital causes as well as trauma have been reported in the literature.3
Colonic obstruction due to blunt abdominal trauma is a rare entity, with IMH as the underlying cause being very rare. Only a few cases of acute IMH in the large bowel following blunt trauma have been reported over the past 25 years.45 The most common finding associated with a IMH is the presence of haemoperitoneum, which was not present in the case discussed. The associated risk factors for the development of IMH include haemophilia, leukaemia, lymphoma and anticoagulation therapy.6 Most of the documented cases involve patients on warfarin or another form of anticoagulation.
The mechanism involved in the formation of IMH is a result of rupture of the intramural blood vessels, presumed to be rare in the colon as the taeniae coli have an apparent protective mechanism to prevent the blood from dissecting through the muscularis propria.6 Generally, a long segment of bowel is affected, compared to the tumour like presentation noted in the case report.
The development of an IMH can result in both acute and chronic complications. These include rupture of the IMH with haemodynamic instability, intussusception of the bowel with IMH as lead point, bowel obstruction and gangrene of the segment of bowel.7 Chronic complications include the formation of fibrotic strictures in the bowel wall resulting in partial or complete obstruction.
The preferred investigations for patient presenting with bowel obstruction due to IMH is contrast enhanced computer tomography (CECT) scan. In resource-constrained health systems, this might not always be feasible, and surgical intervention is often the means of diagnosis. Ultrasound can be used in certain instances, although it is not the modality of choice in bowel obstruction with multiple confounding factors influencing the result, e.g. overlying bowel gas and user variability. It can, however, contribute to monitoring the size of the haematoma once diagnosed in CECT.8
Management of LBO due to IMH depends on the underlying cause. Anticoagulation induced IMH is ideally managed by non-operative means. This involved the correction of the coagulation abnormality by the administration of vitamin K and the transfusion of fresh frozen plasma or freeze-dried plasma. This correction generally occurs within 72 hours, after which the IMH tends to decrease in size and resolve.9
Surgical exploration remains a common means by which an IMH is diagnosed as the cause of bowel obstruction when the clinical presentation warrants intervention. However, by acquiring CECT prior to surgery, many patients could potentially be managed expectantly, especially IMH induced by coagulation disorders and some secondary to trauma.10 LBO due to trauma induced IMH in the absence of coagulation disorders remains a rare entity to this day.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding was required.
Ethical approval
The author/s declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
Prior to commencement of the case write-up, informed consent was obtained from the patient.
ORCID
KS Möller https://orcid.org/0009-0002-5297-7553
E Georgiou https://orcid.org/0000-0003-0920-079X
Y Gurdayal https://orcid.org/0009-0008-3739-0918
REFERENCES
1. Mayo Clinic. Intestinal obstruction - symptoms and causes [Internet]. Mayo Clinic. 2021. Available from: https://www.mayoclinic.org/diseases-conditions/intestinal-obstruction/symptoms-causes/syc-20351460. [ Links ]
2. Johnson WR, Hawkins AT. Large bowel obstruction. Clin Colon Rectal Surg. 2021;34(04):233-41. https://doi.org/10.1055/s-0041-1729927. [ Links ]
3. Farkas NG, Welman TJP, Ross T, et al. Unusual causes of large bowel obstruction. Curr Probl in Surg. 2019;56(2):49-90. https://doi.org/10.1067/j.cpsurg.2018.12.001 [ Links ]
4. Jebin Aaron D, Bhattarai S, Shaikh O, Sistla SC. Traumatic acute colonic intramural haematoma: a rare entity and successful expectant approach. Cureus. 2020;12(8):e9694. https://doi.org/10.7759/cureus.9694 [ Links ]
5. Yin WY, Gueng MK, Huang SM, Chen HT, Chang TM. Acute colonic intramural haematoma due to blunt abdominal trauma. Int Surg. 2000;85(1):51-4. [ Links ]
6. Vecchio R, Cacciola E, Figuera M, et al. Idiopathic intramural haematoma of the right colon. A case report and review of the literature. Int J Surg Case Rep. 2019;60:16-20. https://doi.org/10.1016/j.ijscr.2019.05.004 [ Links ]
7. Nozu T. Idiopathic spontaneous intramural haematoma of the colon: a case report and review of the literature. Clin J Gastroenterol. 2009;2(3):161-5. https://doi.org/10.1007/s12328-008-0061-9. [ Links ]
8. Ibraheem H S, Hashem MS, Ebrahim SH, et al. A rare case of traumatic colonic intramural haematoma in Saudi Arabia. Cureus. 2024 ;16(1):e51461. https://doi.org/10.7759/cureus.51461. [ Links ]
9. Lobo L, Koudki R, Kishan Prasad HL, Shetty B. Colon obstruction due to an anticoagulant induced intramural haematoma: a rare case report. J Clin Diagn Res. 2013;7(4):739-41. https://doi.org/10.7860/JCDR/2013/5283.2899. [ Links ]
10. Polat C, Dervisoglu A, Guven H, et al. Anticoagulant-induced intramural intestinal haematoma. Am J Emerg Med. 2003;21(3):208-11. https://doi.org/10.1016/S0735-6757(02)42258-9. [ Links ]
 Correspondence:
Correspondence:
email: ksmollie123@gmail.com
