










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151Print version ISSN 0038-2361
S. Afr. j. surg. vol.63 n.4 Cape Town 2025
https://doi.org/10.36303/SAJS.02713
TRAUMA SURGERY
Risk factors for foetal loss in injured pregnant patients: an analysis of 105 patients managed at a major trauma centre in South Africa
LN YongI; CY ChungII; VY KongI, III, IV; J KoIII; H LeeV; H WainIV; W BekkerIV; JL BruceIV; GL LaingIV; DL ClarkeIV, VI
IUniversity of Auckland, New Zealand
IIDepartment of Obstetrics and Gynaecology, Western General Hospital, Scotland
IIIDepartment of Surgery, Auckland City Hospital, New Zealand
IVDepartment of Surgery, University of KwaZulu-Natal, South Africa
VDepartment of Surgery, Royal Adelaide Hospital, Australia
VIDepartment of Surgery, University of the Witwatersrand, South Africa
ABSTRACT
BACKGROUND: Pregnant patients in trauma present a unique challenge for clinicians to manage both foetal and maternal well-being, requiring specialised resuscitation algorithms. This study reviews the outcome of pregnant trauma patients in a major trauma centre in South Africa and the risk factors associated with foetal loss.
METHODS: This is a retrospective analysis of all pregnant patients admitted to the Pietermaritzburg Metropolitan Trauma Service (PMTS) from January 2012 to December 2023. Patient data abstracted included mechanism of injury, physiological parameters, injury severity score (ISS), gestational age, diagnostic and surgical procedures performed, complications, and maternal and foetal mortality. Univariate logistic regression analysis was used.
RESULTS: During the study period, a total of 124 female pregnant patients were admitted, and 105 were analysed after excluding 19 patients with missing data. The mean age of the patients in the study was 26 years, with an average gestation age of 18 weeks. Blunt trauma accounted for majority of the injuries (62%). Foetal death occurred in 16% of cases. Risk factors associated with foetal death were high shock index (OR 38.0, 95% CI: 0.8-1793.0), high ISS (OR 1.2, 95% CI: 1.1-1.3), and the need for laparotomy (OR 6.9, CI: 1.4-34.1
CONCLUSION: Risk factors for foetal loss include injury severity, shock on admission and the need for laparotomy. Identifying these risk factors might improve management of foetal and maternal health.
Keywords: trauma, pregnancy, foetal outcome, adverse pregnancy outcomes, mortality
Introduction
Trauma in South Africa remains a significant burden to the healthcare system. Over the last five decades South African surgeons have documented the trauma burden they have confronted and, in the process, have generated a rich oeuvre of publications on the topic.1,2 This bibliography has made a major contribution to our modern understanding of trauma care and has provided a solid evidence base for current strategies in the management of trauma patients. Despite this prodigious effort there remain specific subgroups of patients who are particularly vulnerable as trauma victims, yet who seem to be relatively overlooked or under-researched. These vulnerable populations include women, children and the elderly. A specific group of vulnerable trauma patients is pregnant trauma victims. A pregnant trauma patient presents a unique clinical scenario of "dual-patient complexity" in which both the mother and the foetus are at risk. The scenario poses unique challenges to clinicians. Optimal maternal resuscitation offers the best outcome for the foetus and the management of the pregnant trauma patient has been extensively taught in the Advanced Trauma Life Support (ATLS) course.
Studies have previously looked at a range of factors associated with foetal loss. A consistent finding across several retrospective reviews, is the association between high injury severity score (ISS) and increased risk of foetal demise.3,4 Maternal physiological factors, such as hypotension and elevated lactate, have also emerged as potential predictors, though findings regarding their reliability remain mixed.4-6 Certain injury characteristics, such as severe abdominal trauma, penetrating mechanisms and the presence of disseminated intravascular coagulation (DIC), have significantly correlated with foetal mortality.5,7,8 Esposito et al 9. noted that conventional vital signs like maternal blood pressure and pulse rate may be poor surrogates for foetal wellbeing, highlighting the complexity of maternal-foetal assessment. Despite these insights, there remains variability in reported risk factors, reflecting the heterogeneity of trauma presentations and the limited prospective data available. This study aims to further characterise the predictors of foetal loss, using a large electronic database at a busy institution in South Africa.
Materials and methods
Clinical setting
The Pietermaritzburg Metropolitan Trauma Service (PMTS) is based at Greys Hospital in Pietermaritzburg, South Africa. This is a very busy trauma service which admits over two thousand severely injured patients annually. The ATLS approach is widely regarded as the standard of care in the PMTS and is religiously enforced and followed. All pregnant trauma patients are resuscitated based on ATLS principles. All female patients of childbearing age are routinely screened (urinary and/or serum HCG) for pregnancy. Resuscitating the mother and treating her according to her injuries is prioritised. The foetus is of secondary concern. Although an obstetrical opinion is obtained early during the admission, it is predominantly to confirm the pregnancy state and to ascertain if the foetus is viable. In patients who sustain trauma while in an advanced state of pregnancy, and if the foetus is mature enough to survive, consideration is given to delivery, which makes management of the mother less complex. If the foetus is immature, an expectant approach is adopted. Managing the mother's injuries remains the priority. Informed consent for radiological investigations is documented in patient records prior to imaging. Obstetric consultation is obtained early in all cases. The PMTS has maintained a regional electronic trauma registry, known as the Hybrid Electronic Medical Registry (HEMR) since December 2012. This system captures clinical data on all patients admitted to our trauma centre.
The study
Data from HEMR from January 2012 to December 2023 were retrospectively reviewed. All patients who were documented to be pregnant and sustained injuries admitted to our institution were included. Patient demographics, admitting physiological parameters, operative findings and clinical outcomes were reviewed.
Statistical analyses
IBM SPSS version 29 was used to analyse the data. Independent variables were screened for inclusion in the multivariable logistic regression model using univariate logistic regression analysis. Variables with a p-value less than 0.2 were selected to enter the multivariable model. Two approaches were taken, after which the results were compared. The first approach was a complete case analysis using logistic regression, excluding two predictors with high percentage of missing data. The second approach used multiple imputation of the values with a high percentage of missing, followed by pooled logistic regression analysis of the imputation datasets including the imputed variables.
Results
Characteristics of patients at admission
During the 12-year study period 19 873 trauma patients were admitted, of which, 3 421 (17%) were female of whom 33% sustained interpersonal violence. Of 3 421 female trauma patients, 124 (3.6%) were pregnant. In 19 patients, incomplete data precluded further analysis. Of the 105 patients included in analyses, the mean age was 26 ± 7 years and the mean gestational age was 18 ± 9 weeks.
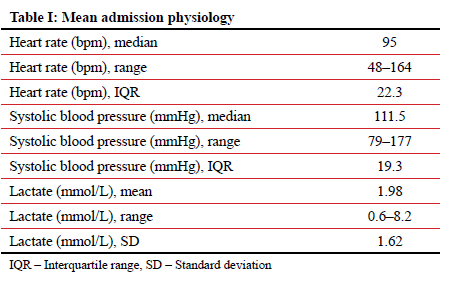
The overall admission physiology characteristics are summarised in Table I.
Forty (38%) patients sustained a penetrating injury. Knife wounds, gunshot wounds and others accounted for 57.5%, 30% and 17.5% of all penetrating injuries respectively. The remaining 65 (62%) of patients sustained a blunt injury. Motor vehicle crashes, assault, pedestrian strike, falls and others account for 43.1%, 35.4%, 13.8%, 4.6% and 17.5% of all blunt injuries respectively. Seven patients suffered more than a single mechanism of injury. Just under two-thirds of patients sustained injuries secondary to interpersonal violence.
The overall median ISS was 4 (1-37). Injury distribution by anatomical region was highest in the head and abdominal region, each accounting for 36 cases. This was followed by injuries to the thorax, lower limbs, upper limbs, neck, face, and pelvis, as seen in 31, 24, 22, 17, 15 and 7 cases respectively.
Investigations and management
Plain radiographs were obtained for 72 (69%) of patients, making up a total of 156 images. Chest films were the most frequently performed (n = 53), followed by cervical spine (n = 30), extremity (n = 23), skull (n = 20), pelvic (n = 19), abdominal (n = 9), contrast swallow studies (n = 1) and cystogram studies (n = 1). Fifty (48%) patients required a CT scan, making a total of 77 cross-sectional images undertaken. A total of 77 cross-sectional investigations were performed, including 74 CT scans: head (n = 20), angiography (n = 16), abdomen (n = 11), neck (n = 10), pelvis (n=8), thorax (n = 5), and whole-body (n = 4); and 3 MRI scans: thorax (n = 2) and neck (n = 1). Fourteen (13%) patients were investigated with Focused Assessment with Sonography in Trauma (FAST) scans, and 32 (30%) patients underwent a formal ultrasound scan. This comprised abdominal (n = 15), obstetric (n = 7), pelvic (n = 7), cardiac (n=4), and forearm (n = 1) scans, with some patients undergoing more than one type of scan (34 scans in total).
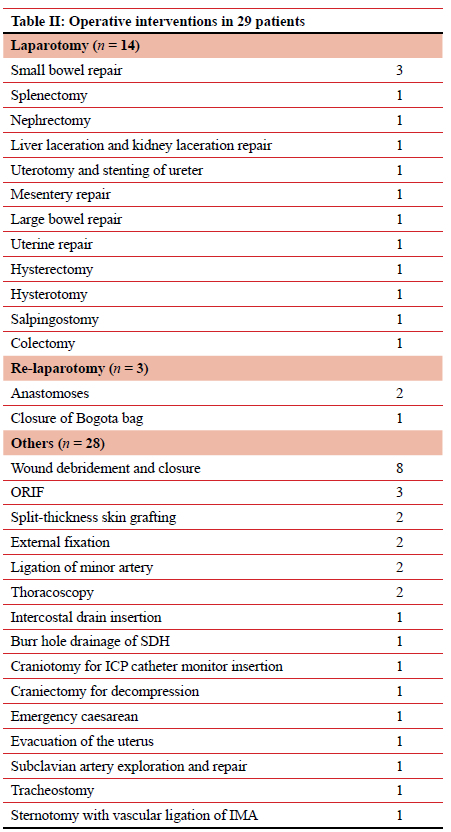
A total of 29 (28%) patients required operative management. This is summarised in Table II.
Complications
Only 14% of patients required admission to the intensive care unit (ICU). Three required ventilatory support, and the mean ICU stay was four days. The mean duration of hospital stay for all 105 patients was six days and 10% experienced one or more complication during admission. The overall mortality was 1% (1/104). The single patient who died suffered a massive pulmonary embolism.
Obstetric characteristics and outcomes
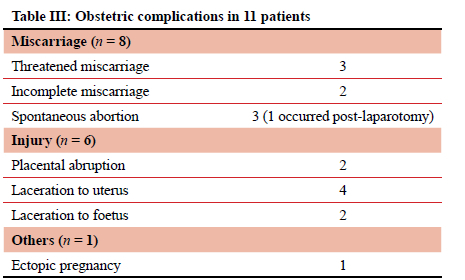
The mean gestational age was 18 weeks, and it ranged from 3 to 36 weeks. Thirty (29%) foetuses were within the first trimester, 50 (48%) within the second trimester, and 14 (13%) within the third trimester. The gestational age was unknown in 11 (10%) patients. A total of 11 (10%) patients experienced obstetric complications. These are summarised in Table III.
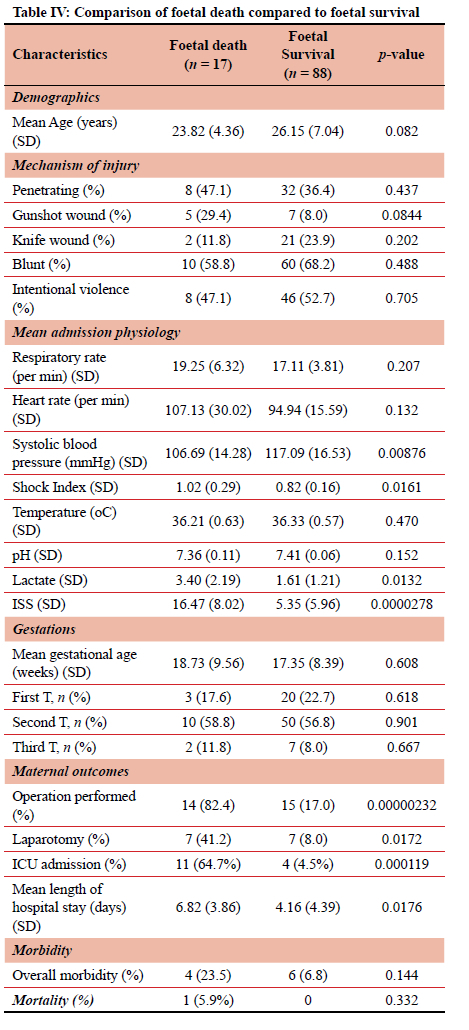
Foetal survival at discharge was 88 (84%). Foetal death was documented in 17 (16%). This included a single maternal death. Among the 17 cases of foetal death, 15 were intrauterine deaths, one a premature birth at 28 weeks, and one a stillbirth at 36 weeks. A comparison between patients with foetal death and foetal survival is summarised in Table IV
Foetal mortality
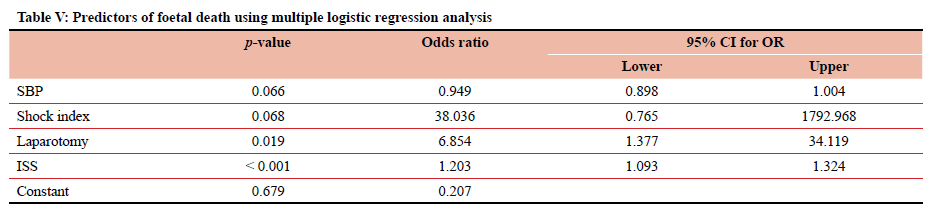
Increase in shock index by 1 resulted in 37 times higher odds of foetal death (p = 0.068). Every 0.1 increase in shock index resulted in 1.4 times higher risk of foetal mortality. A 1 mmHg increase in SBP resulted in a 5% decrease in odds of foetal death (p = 0.066). One unit increase in ISS resulted in 1.2 times higher odds of foetal death (p < 0.001). Patients having a laparotomy were 6.9 times more likely to have a foetal death than those not having a laparotomy (p = 0.019). These results are summarised in Table V
Intentional injury
Approximately half (51%) of the injuries were a result of intentional injury. Among those with available data, 22 reported assailants were known to the patient, a majority being current or former intimate partners (n = 17), followed by family members (n = 4) and an acquaintance (n = 1). Four patients reported assailants who were unknown to them, through robbery incidents (n = 2), a single unidentified assailant (n = 1) and a group assault (n = 1).
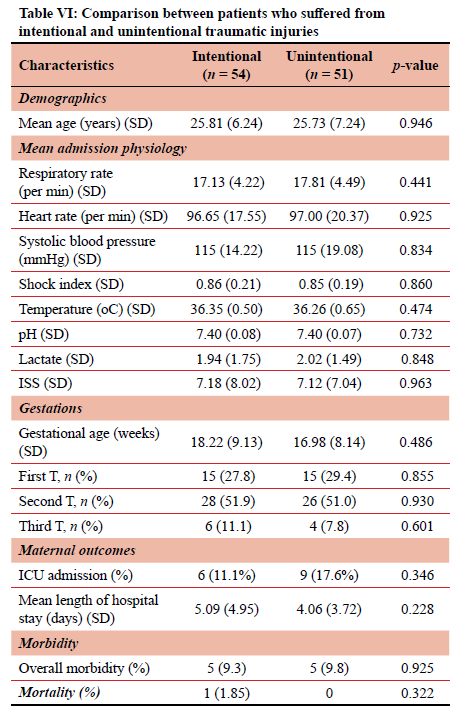
Among the 54 patients, six experienced more than one mechanism of injury. Penetrating trauma was involved in 36 cases, involving knife wounds (n = 21), gunshot wounds (n = 11), and other mechanisms (n = 6). Two patients sustained more than one type of penetrating injury. All 22 cases of blunt trauma were a result of physical assault. Table VI compares the outcome in patients with intentional and non-intentional trauma.
Discussion
Managing the pregnant trauma patient can be challenging as there are physiological changes which may complicate the resuscitation. Despite this the parameters of resuscitation are largely the same as in the non-pregnant patient. The mother remains the priority as the only way to improve foetal outcome is by ensuring optimal maternal outcome.
Trauma in pregnancy is encountered in just under four per cent of female trauma patients. Of concern is that half of all pregnant trauma patients experience interpersonal violence and in half of these cases, this is inflicted by an intimate partner. This reflects the unacceptably high rates of gender-based violence in South Africa. In most series blunt mechanisms are much more common than penetrating mechanisms in pregnant trauma patients. A MEDLINE-based review found that trauma affected eight per cent of all pregnancies but in only 16 per cent was the mechanism penetrating, whilst a major retrospective audit from the Los Angeles County trauma service had an incidence of penetrating trauma of nine per cent.5,11 In our service the ratio of penetrating to blunt trauma was in the order of 40:60. The relatively high proportion of penetrating injuries in our cohort contrasts with international findings, and reflects the difference of South African patterns of trauma.
In the case of trauma to the pregnant patient, the foetus is at much higher risk than the mother as evidenced by the significant discrepancy between maternal mortality (1%) and foetal loss (16%). Our findings reinforce previous literature showing that foetal loss is strongly associated with markers of maternal instability, injury severity, and the need for operative intervention. Improving outcomes in the management of the pregnant trauma patient must focus on reducing the rate of foetal loss. The only way to achieve this is by optimising maternal management. Shock needs to be treated aggressively, and laparotomy must be restricted to those patients who absolutely need this intervention.
Future research could benefit from the inclusion of clinical variables to more comprehensively assess the management and outcomes of pregnant trauma patients, particularly those presenting in shock. Data in initial resuscitative efforts, including fluid administration, blood and blood product transfusion, and RhD testing would provide valuable insights. The use of Kleihauer-Betke testing, RhoGAM, and cardiotocography (CTG) monitoring may also inform the adequacy of obstetric-specific interventions.10 CTG monitoring is not routinely performed before foetal viability is reached, as defined by local institutional protocols. In South Africa, viability is recognised at 26 weeks' gestation in accordance with legal definitions. With access to advanced neonatal care, viability may be considered from as early as 24 weeks or at a foetal weight exceeding 500 grams. Consequently, limited assessment of foetal well-being is possible on admission for patients presenting before this gestational threshold. Otherwise, CTG offers a non-invasive method of foetal surveillance that can provide critical insights into foetal status, such as persistent bradycardia, reduced variability or late decelerations, all early indicators of obstetric complications.11 Inclusion of these parameters in future studies would enhance our understanding of the clinical course and inform best practices for the care of future trauma victims.
Conclusion
Trauma in pregnancy is uncommon but is associated with a high rate of foetal loss. Risk factors for foetal loss include injury severity, shock on admission and the need for laparotomy. Identifying these risk factors might improve management of foetal and maternal health in the context of trauma.
Acknowledgements
Thanks to Tonya Esterhuizen, Biostatistician at Stellenbosch University, who supported with statistical analyses.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding was required.
Ethical approval
Ethical approval for ongoing maintenance of HEMR and for conducting this study was granted by the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal (UKZN) [Ethical approval number: BCA 221/13].
ORCID
LN Yong https://orcid.org/0009-0003-3627-8610
G Chung https://orcid.org/0009-0004-4806-3550
VY Kong https://orcid.org/0000-0003-2291-2572
J Ko https://orcid.org/0000-0001-8139-5208
H Lee https://orcid.org/0000-0001-8461-9932
H Wain https://orcid.org/0000-0002-6693-0062
W Bekker https://orcid.org/0000-0003-0695-5994
JL Bruce https://orcid.org/0000-0001-8666-4104
GL Laing https://orcid.org/0000-0001-8075-0386
DL Clarke https://orcid.org/0000-0002-8467-1455
REFERENCES
1. Moffatt SE, Goldberg B, Kong VY, et al. Trauma in pregnancy at a major trauma centre in South Africa. S Afr Med J. 2020;110(7):667-70. https://doi.org/10.7196/samj.2020.v110i7.14153. [ Links ]
2. Wall SL, Figueiredo F, Laing GL, Clarke DL. The spectrum and outcome of pregnant trauma patients in a metropolitan trauma service in South Africa. Injury. 2014;45(8):1220-3. https://doi.org/10.1016/j.injury.2014.04.045. [ Links ]
3. Rogers FB, Rozycki GS, Osler TM, et al. A multi-institutional study of factors associated with foetal death in injured pregnant patients. Arch Surg. 1999;134(11):1274-7. https://doi.org/10.1001/archsurg.134.11.1274. [ Links ]
4. Aboutanos SZ, Aboutanos MB, Dompkowski D, et al. Predictors of foetal outcome in pregnant trauma patients: a five-year institutional review. Am Surg. 2007;73(8):824-7.https://doi.org/10.1177/000313480707300820. [ Links ]
5. Petrone P, Talving P, Browder T, et al. Abdominal injuries in pregnancy: a 155-month study at two level 1 trauma centres. Injury. 2011;42(1):47-9. https://doi.org/10.1016/j.injury.2010.06.026. [ Links ]
6. Baerga-Varela Y, Zietlow SP, Bannon MP, Harmsen WS, Ilstrup DM. Trauma in pregnancy. Mayo Clin Proc. 2000;75(12):1243-8. https://doi.org/10.4065/75.12.1243. [ Links ].
7. Ali J, Yeo A, Gana TJ, McLellan BA. Predictors of foetal mortality in pregnant trauma patients. J Trauma. 1997;42(5):782-5. https://doi.org/10.1097/00005373-199705000-00005. [ Links ]
8. Shah KH, Simons RK, Holbrook T, Fortlage D, Winchell RJ, Hoyt DB. Trauma in pregnancy: maternal and foetal outcomes. J Trauma. 1998;45(1):83-6. https://doi.org/10.1097/00005373-199807000-00018. [ Links ]
9. Esposito TJ, Gens DR, Smith LG, Scorpio R, Buchman T. Trauma during pregnancy. A review of 79 cases. Arch Surg. 1991;126(9):1073-8. https://doi.org/10.1001/archsurg.1991.01410330027003. [ Links ]
10. Liggett MR, Amro A, Son M, Schwulst S. Management of the pregnant trauma patient: a systematic literature review. J Surg Res. 2023;285:187-96. https://doi.org/10.1016/j.jss.2022.11.075. [ Links ]
11. Alfirevic Z, Gyte GM, Cuthbert A, et al. Continuous cardiotocography (CTG) as a form of electronic foetal monitoring (EFM) for foetal assessment during labour. Cochrane Database of Syst Rev. 2017;2(2):CD006066.https://doi.org/10.1002/14651858.CD006066.pub3. [ Links ]
 Correspondence:
Correspondence:
email: victorywkong@yahoo.com

{kind=link}