










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.115 n.6 Pretoria Jul. 2025
https://doi.org/10.7196/SAMJ.2025.v115i6.2608
RESEARCH
Intravenous antibiotic use in a private mining hospital in North West Province, South Africa
D SeimelaI; J M du PlessisII; M VorsterIII; A F van NiekerkIV
IBPharm; Medicine Usage in South Africa, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IIMB ChB, MPharm; Medicine Usage in South Africa, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IIIBPharm, MBA; Medicine Usage in South Africa, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IVBPharm, MScPharm; Medicine Usage in South Africa, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
ABSTRACT
BACKGROUND. The misuse and overuse of intravenous (IV) antibiotics contribute to the spread of multidrug resistance, consequently increasing mortality. These effects can be minimised through treatment reviews that aim to optimise antibiotic therapy without compromising patient clinical outcomes. There is therefore a need to evaluate and monitor intravenous antibiotic usage in hospitals.
OBJECTIVES. To describe IV antibiotic use in admitted patients at a private hospital in North West Province, South Africa.
METHODS. A cross-sectional study design was followed using retrospective data from patient files and the hospital electronic healthcare software (TriMed) between 1 January and 31 December 2022. A Microsoft Excel spreadsheet was used to capture demographic information for each patient profile that met the inclusion criteria, and data on IV antibiotic use were captured for each admission episode. The data were analysed using IBM statistical software.
RESULTS. Demographic data were recorded for 677 patient profiles, with males representing 53.8% (n=364). A total of 731 admissions occurred during the study period. The most prevalent indication for IV antibiotic use, according to the provisional diagnosis, was upper and lower respiratory tract disorders, which represented 25.2% of the total admissions. Staphylococcus aureus was the most commonly treated micro-organism, representing 22.8% (n=23) of the total isolated micro-organisms. IV antibiotics were initiated 885 times, and amoxicillin-clavulanic acid was the most used antibiotic (51.2%). Most antibiotics (48.2%) were used at a dose of 1 200 mg, with a dosing frequency of three times a day (72.3%). A total of 806 review actions, out of 885 intravenous antibiotic initiations, were conducted (91.1%). The prevalence of IV-to-oral switch was 49.0%, while 41.3% of IV antibiotics were stopped after review. IV antibiotic de-escalation represented 7.2% of the total reviews, while an oral antibiotic was added to 1.7% of the IV antibiotics after review. At review, the prevalence of adding IV antibiotics to another IV antibiotic was 0.7%. The average length of hospital stay was 5.8 days, while patients continuously received IV antibiotics for 3.4 days on average.
CONCLUSION. There is a need to monitor IV antibiotic use and encourage IV antibiotic de-escalation to limit the rampant use of broad-spectrum antibiotics and manage the most prevalent infections effectively in the shortest possible time, consequently reducing the average duration of hospitalisation. IV antibiotic treatment review is therefore pivotal to optimise antibiotic therapy, the transition of IV to oral antibiotics, and discontinuation of IV antibiotics when they are no longer necessary.
Keywords: intravenous antibiotics, antibiotic use, in-hospital antibiotics, IV-to-oral switch, antibiotic de-escalation
Antibiotics are agents used to treat and manage confirmed or suspected bacterial infections. These include, among others, urinary tract infections, meningitis, pneumonia, intra-abdominal infections and bloodstream infections that can originate in hospital or community settings.[1] In surgical procedures, they are used as prophylaxis to prevent infections during or after a procedure.[1] The use of antibiotics in hospital settings is considered a cornerstone of contemporary medicine.[2]
Intravenous (IV) antibiotic use, common in both low- and high-income countries, plays a crucial role in saving lives, especially by treating and managing life-threatening bacterial infections.[3] Antibiotics are administered intravenously to efficiently achieve serum peak concentrations in the shortest possible time, consequently reducing mortality.[4,5] It is commonly believed that IV antibiotics are superior to oral formulations, especially when treating severe infections.[6] In South African (SA) hospitals, a study evaluating antibiotic use indicated that >50% of the prescribed antibiotics were administered intravenously.[7] The overuse and misuse of IV antibiotics when oral formulations with equivalent efficacy are available is a form of irrational antibiotic use that can compromise patient outcomes and strain healthcare systems financially owing to increased costs associated with IV administration and prolonged hospital stays.[8]
The overuse and misuse of IV antibiotics enable antibiotic resistance (ABR) that causes antibiotics to lose their effectiveness against various pathogens.[9,10] ABR is a global public health crisis that can lead to increased mortality, morbidity and healthcare costs.[11] By 2050, it is estimated that ABR will have caused >10 million deaths.[12] This figure can be reduced by implementing global and national action plans that aim to reduce the spread of ABR through surveillance, effective communication, training and research.[13] The World Health Organization (WHO) has introduced the AWaRe (Access, Watch and Reserve) classification, which aims to promote rational antibiotic use and reduce the prevalence of ABR by encouraging the use of antibiotics from the Access group rather than the Watch and Reserve groups.[14] Antibiotics in the Access group have a lower chance of resistance and are active against commonly isolated bacterial pathogens, while those in the Watch group are used to treat a limited number of specific bacterial infections and have a higher chance of resistance.[14] Antibiotics in the Reserve group should only be used for confirmed or suspected bacterial infections caused by multidrug-resistant pathogens.[14] Irrational use of IV antibiotics can also be associated with risks that may compromise patient clinical outcomes.
The risks associated with IV antibiotic use include IV-line complications, dose miscalculations, and errors in IV preparation and administration.[15] Antibiotic utilisation monitoring programmes in healthcare institutions have implemented measures such as IV-to-oral switches to reduce these adverse effects.[16] The IV-to-oral switch in clinically suitable patients who can tolerate oral formulations is a recommendation of global and local initiatives to guide antibiotic prescribing practices.[17,18] Short-term administration of IV antibiotics for 2 - 3 days, followed by an oral formulation, can be implemented in the treatment plan for bacterial infections.[18-20] The IV-to-oral switch is associated with a shorter length of hospital stay (LOS), reduced adverse effects, and a reduction in expenditure associated with IV antibiotic use.[21]
IV antibiotic de-escalation is an intervention that is associated with reduced adverse effects, optimal clinical outcomes, and a decrease in the spread of ABR. It entails discontinuing one or more antibiotics during empirical therapy and switching to a narrow-spectrum antibiotic specifically targeting the isolated bacterial pathogen.[22,23] De-escalation in IV antibiotic therapy is an important concept that monitoring programmes and international guidelines on antibiotic use have adopted.[24] However, in some instances, antibiotics are used in combination to broaden the spectrum of antibiotic activity, promote the rapid killing of bacterial pathogens, and delay the emergence of resistance. Combination therapy is associated with optimised clinical outcomes, but it is expensive and increases the risk of adverse effects.[25]
Surveillance strategies have been implemented as part of a worldwide healthcare standard to measure IV antibiotic use and improve antibiotic prescribing practices in hospitals. They include defined daily dose (DDD), days of therapy (DOT) and length of therapy (LOT) methods.[26] These methods aim to improve the quality of patient care by reducing unnecessary and excessive antibiotic use, thus reducing the spread of ABR.[27] Through the present study, we aimed to contribute to the existing knowledge base and to shed light on the patterns of IV antibiotic use in North West Province, SA. It is part of a surveillance strategy to monitor IV antibiotic prescribing practices at a private hospital in North West Province by describing IV antibiotic use, stratified by the name of the active pharmaceutical ingredient (API), clinical indication, dose and dosing frequencies, treatment periods, and actions taken after IV treatment review.
Methods
Study design and setting
A cross-sectional study design was followed using retrospective data from 1 January 2022 to 31 December 2022 from a private hospital in North West Province. The hospital provides healthcare services exclusively to people working in the mining area and is affiliated with the company's medical plan. It has 236 beds and four wards, namely general, medical, female and surgical wards. The female ward has a section within the ward that admits paediatric patients.
Study population
An all-inclusive sampling method was adopted for patient records that met the following inclusion criteria: (i) admitted patient who received at least one IV antibiotic, regardless of their age and sex; and (ii) admitted in one of the four wards of the private hospital. The study excluded patient records of outpatient department consultations, patients admitted as theatre cases, and patients admitted for a medical emergency and not affiliated with the company's medical plan.
Data collection
Data were collected on an Excel spreadsheet, Microsoft Office 2021 (Microsoft, USA), using a data collection tool based on the WHO process and outcome indicators for IV antibiotic use.[28] Primary data sources were patient hard-copy files and the hospital's electronic healthcare software (TriMed, version 2022.1.0; TriFour Systems, SA). The information captured from the data sources included demographic information, treatment plans and clinical notes. Demographic information such as age, sex, ward and comorbidities was collected from the patient file and the TriMed system and recorded for each patient profile that met the inclusion criteria. Ages were stratified into different groups to indicate paediatrics (<12 years), teenagers (12 - 17 years), working age groups (18 - 24 years, 25 - 39 years and 40 - 59 years), and pensioners (>60 years). Information on IV antibiotic use, including provisional diagnosis on admission, micro-organism identified (if a microbiology test was conducted), name of the API, dose (in mg), dosing frequency, treatment period, review action and LOS (in days), was collected from the patient files and recorded for each time the patient was admitted. Themes were generated to report on provisional diagnoses by grouping them based on the human anatomical system, and the provisional diagnoses frequently recorded. Each API name was recorded together with the WHO classification of Access, Watch and Reserve. The dosing frequency was expressed as daily, immediate dose (stat), twice a day (bd), three times a day (tds) and four times a day (qid). The review actions were recorded in five categories: add IV to IV, add oral to IV, de-escalation, stop, and IV-to-oral switch. The collection of information using the patient file in hard copy and the TriMed system ensured the accuracy and validity of the collected data.
Data analysis
The collected data were analysed using Statistical Package for the Social Sciences (SPSS) software, version 27 (IBM, USA). Descriptive statistics were calculated for all study variables. Categorical variables were expressed as frequencies and percentages, while continuous variables were expressed as means and standard deviations (SDs).
Ethical considerations
All ethical requirements as predefined by North-West University and the study setting were followed. Approval to conduct the study was obtained from the hospital management and the North-West University Health Research Ethics Committee (ref. no. NWU- 00056-23-A1).
Results
Demographic information
A total of 677 patient profiles were retrospectively recorded. Male patients represented 53.8% (n=364) of the total admissions, while females represented 46.2% (n=313). The mean (SD) age at the time of admission was 40 (19.81) years, and the median (interquartile range (IQR)) age was 42 (26) years. The youngest patient recorded in the study was 1 year old, while the oldest was 88. Fig. 1 illustrates the age and sex distribution of the admitted patients in the different age groups.
Of 677 patient profiles, 48.1% (n=326) were reported without comorbidities. HIV was a comorbidity in 20.8% (n=140) of the total patient profiles. Hypertension was the highest recorded non-communicable comorbidity, representing 25.8% (n=175) of the patient profiles. Multiple comorbidities were present in 18.1% (n=123) of the patient profiles.
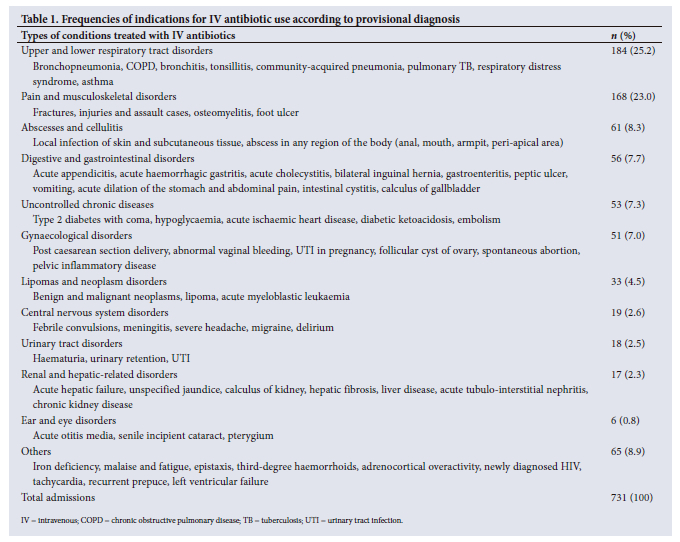
The most common indications for in-hospital IV antibiotic use, according to the provisional diagnosis based on the total admissions, were respiratory tract disorders and musculoskeletal disorders. They represented 25.2% (n=184) and 23.0% (n=168) of the total admissions, respectively. Table 1 retrospectively reports on indications for in-hospital IV antibiotic use as per the provisional diagnosis.
A total of 179 microbiology tests were conducted, of which 78 yielded no growth. Staphylococcus aureus was the most commonly identified micro-organism following microbiology testing, representing 22.8% (n=23) of total micro-organisms. Fig. 2 shows the most commonly isolated micro-organisms in admitted patients who received IV antibiotics.
Patterns of IV antibiotic use
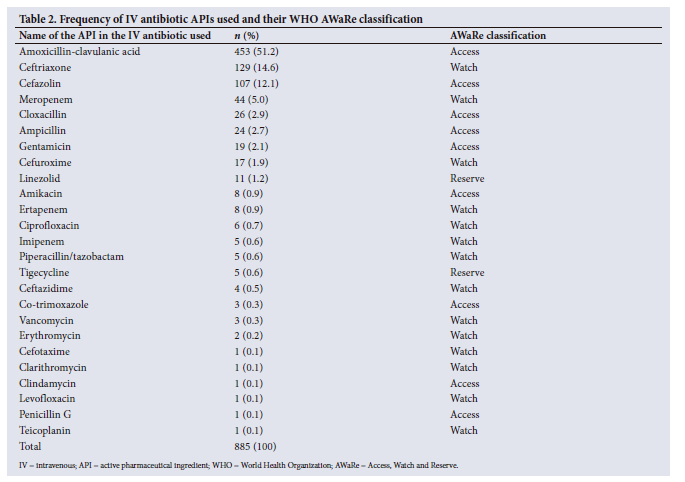
IV antibiotics were initiated 885 times. The most used IV antibiotic was amoxicillin-clavulanic acid (51.2%) in the Access group, ceftriaxone (14.6%) in the Watch group, and linezolid (1.2%) in the Reserve group (based on the WHO AWaRe classification). The overall IV antibiotic usage as per the WHO AWaRe classification revealed that 72.4% were in the Access group, followed by 25.7% in the Watch group and 1.8% in the Reserve group. Table 2 shows the frequency of the IV antibiotic APIs and their WHO AWaRe classifications.
Dosing and dosing frequency of IV antibiotic use
A dose of 1 200 mg, representing 48.2% (n=427) of the total IV antibiotics initiated, was mostly used for amoxicillin-clavulanic acid, which is the most used IV antibiotic in the study setting. The second most prescribed dose was 1 000 mg for ceftriaxone at 34.0% (n=301). IV antibiotics were used primarily at tds frequency, representing 72.3% (n=640) of the total IV antibiotics used. The dosing frequency of tds correlated with the recommended dosing frequency for both amoxicillin-clavulanic acid and ceftriaxone, which were the most used IV antibiotics.
Treatment period of IV antibiotics
The average duration of continuous IV antibiotic use in admitted patients was 3.4 days, with an SD of 4.4 and a median of 2.0 days. Thereafter, the IV antibiotic was stopped, changed, or switched to an oral formulation. The longest recorded duration of continuous IV antibiotic use was 67.0 days, for a patient with hypertension and diabetes who was admitted for abscess and cellulitis infection, where a microbiology test identified Escherichia coli.
Duration of hospital stay
The mean (SD) LOS was 5.8 (7.4) days, and the median (IQR) 7.4 (4.0) days. A high SD indicates significant variability in the LOS. A total of 45 of 731 admissions were for >10 days. The longest recorded duration of hospitalisation was 84.0 days, while the shortest was 0 days. The LOS correlated with the duration of continuous IV antibiotic use; the longer the duration of IV antibiotic, the longer the LOS.
Review of IV antibiotics
A total of 806 review actions were performed on IV antibiotics initiated. The review actions were grouped into five categories: add IV to IV, add oral to IV, IV antibiotic de-escalation, stop IV antibiotics, and IV-to-oral switch. The IV-to-oral switch represented 49.0% (n=395) of the total reviews, while 41.3% (n=333) represented discontinuation of IV treatment after the review. Table 3 indicates the review actions, frequencies and percentages.

The average duration of hospital stay after treatment review was 2.0 days, with a mode of 0 days.
Discussion
This study evaluated IV antibiotic use and the review actions taken after initiating IV antibiotics. The following are the key findings: respiratory and musculoskeletal disorders were the most commonly recorded provisional diagnoses at admission, while S. aureus was the most commonly identified micro-organism after microbiological testing. Amoxicillin-clavulanic acid was the IV antibiotic agent most commonly used in the study setting, with the majority of IV antibiotics prescribed falling into the Access group. The most commonly prescribed dose was 1 200 mg for amoxicillin-clavulanic acid, representing >48% of the prescribed doses, while 72.3% of the IV antibiotics were prescribed at a dosing frequency of tds. The dosing frequency of tds could indicate compliance with the SA dosing guidelines for the use of amoxicillin-clavulanic acid and ceftriaxone, which were the most commonly used IV antibiotics in the study.
In some instances, the IV antibiotics were continuously administered for durations longer than recommended, and during the treatment review, IV antibiotics were mainly switched to oral formulations or stopped, based on the clinical presentation of the patient, microbiology results, and whether or not the patient was able to tolerate oral formulations.[18] The duration exceeding the normal recommended duration was noted in a patient provisionally diagnosed with cellulitis and given IV antibiotics for over 2 months, with E. coli being the identified micro-organism. A study on E. coli cellulitis in immunocompromised patients indicated that patients clinically improve after 11 days of IV antibiotic therapy, and thereafter the treatment regime should be downgraded to oral antibiotic formulations.[29] The prevalence of IV antibiotic de-escalation was low, indicating that antibiotic de-escalation was rarely done in the study setting.
The study was conducted in a private hospital in North West Province, where most admitted patients were males between 25 and 59 years old, representing the 'working group' in the SA population. The female ward had the highest admission rate, as it uniquely accommodated both female and paediatric patients, unlike the other three wards, which exclusively admitted male patients. Upper and lower respiratory tract disorders, followed by pain and musculoskeletal disorders, represented the highest percentages of admissions. This finding could be because the working environment of the private company is characterised by strenuous working activities and air pollution.[30,31] Guidelines specifically targeting IV antibiotic use in respiratory and musculoskeletal disorders must be strengthened to optimise the clinical outcomes of patients presenting with these disorders.
Amoxicillin-clavulanic acid in the Access group was the IV antibiotic used the most, representing just over 50% of all IV antibiotics used. With regard to overall usage of antibiotics, 72.4% were in the Access group, followed by 25.7% in the Watch group. The WHO has recommended that by 2023, Access antibiotics should represent at least 60% of all antibiotics used; the research findings therefore show that the hospital was adherent to the WHO guidelines.[14] In some settings, a lack of institutional antibiotic usage guidelines could be the possible cause of non-adherence to the specific recommendations of the WHO.[32] Antibiotic monitoring programmes such as antibiotic stewardship involving multidisciplinary healthcare professionals can ensure compliance and improve antibiotic usage through education, training, updating of guidelines, and active monitoring of antibiotic use.[33]
Our study further revealed that the average duration of continuous IV antibiotic use was 3.4 days (>72 hours), and IV treatment was reviewed after that. The time it takes to review IV antibiotics from the date of initiation is of paramount importance in ensuring that patients receive optimal clinical care in the shortest time possible.[34] The study found a 91.1% prevalence of IV treatment reviews, primarily involving IV-to-oral switches (49.0%) or stopping IV antibiotics (41.3%), with limited de-escalation (7.2%), and an average continuous IV antibiotic use of 3.4 days before review. A 100% prevalence of IV treatment review is encouraged, as it indicates a complete review of all IV antibiotics prescribed. An IV-to-oral switch, representing 49.0% of the total reviews, could have been influenced by the many patients whose IV antibiotics were stopped after review. The practice of IV-to-oral switch has been proven beneficial for both the patient and the hospital setting.[16] An Austrian study indicated that an IV-to-oral switch 48 - 72 hours after initiation reduces the readmission rate, minimises the reoccurrence of infections, and has been proven to avoid >6 000 doses of IV antibiotics.[4] An IV-to-oral switch can therefore be practised in clinically stable patients to reduce LOS, which was recorded as 5.8 days in the present study. Antibiotic de-escalation occurred 58 times, representing 7.2% of the total reviews. Antibiotic de-escalation is essential to reduce the spread of ABR by using narrow-spectrum antibiotics that specifically target the cultured pathogen and limit the use of broad-spectrum antibiotics, which are associated with spread of ABR when misused or overused.[35]
The present study showed that most patients were discharged after IV treatment was reviewed and switched to an oral formulation. This finding could indicate that the IV-to-oral switch was conducted because the patient had to be discharged, and it was not necessarily an in-hospital intervention. The study also revealed 14 instances where oral antibiotics were added to IV antibiotics during treatment review. This addition could have been because the API of the specified antibiotic agent was procured only in oral formulation in the study setting. Adding an oral formulation to the IV antibiotic indicates that the patients qualified to take oral formulations, yet were put on IV antibiotics. Ward rounds with the involvement of a pharmacist are recommended to assist in addressing pharmacokinetic concerns and ensuring that the appropriate IV-to-oral switch is performed to treat patients optimally.[36]
Study limitations
The study was conducted in a single setting in North West Province, and as a result the findings cannot be generalised to all hospitals in SA or even North West Province. The study population is a mining community, so the findings cannot be generalised to the ordinary population outside the mining community or patients in private hospitals in North West Province. The study did not assess whether the dose and frequency of the prescribed antibiotics were appropriate for the identified diagnosis, so conclusions on the appropriateness of antibiotic prescribing cannot be drawn.
Conclusion
The study results highlight the need to monitor IV antibiotic use in hospital settings. Appropriate monitoring will help minimise unnecessary use of IV antibiotics when patients can be managed effectively with oral formulations, and limit the use of broad-spectrum antibiotics through de-escalation. IV antibiotic use in hospitals can also be improved by encouraging the selection of antibiotic agents in the WHO Access group and reducing the use of Watch and Reserve antibiotics at the point of initial admission, thus assisting in minimising the spread of ABR. The study also identified a gap in the practice of IV antibiotic de-escalation. We propose future research studies focusing on factors that hinder the practice of antibiotic de-escalation when conducting IV treatment reviews.
Data availability. The datasets generated and analysed during the present study are available from the corresponding author (JMdP) on reasonable request. Any restrictions or additional information regarding data access can be discussed with the corresponding author.
Declaration. None.
Acknowledgements. The authors thank the private hospital (study setting) for giving permission to conduct the study and providing the necessary data to achieve the study objectives.
Author contributions. All authors contributed to the conception and the design of the study. DS performed data collection. JMdP and DS analysed the data. All authors reviewed and commented on subsequent versions of the manuscript. All authors read and approved the final version of the manuscript.
Funding. None.
Conflicts of interest. DS is employed as a pharmacist in the study setting. The study retrospectively looked at the use of IV antibiotics as prescribed by medical practitioners. DS therefore did not have any direct influence on the issues the study aimed to address. The other authors had no conflict of interest.
References
1. Lakoh S, Adekanmbi O, Jiba DF, et al. Antibiotic use among hospitalised adult patients in a setting with limited laboratory infrastructure in Freetown Sierra Leone, 2017-2018. Int J Infect Dis 2020;90:71-76. https://doi.org/10.1016/jijid.2019.10.022 [ Links ]
2. Maxson T, Mitchell DA. Targeted treatment for bacterial infections: Prospects for pathogen-specific antibiotics coupled with rapid diagnostics. Tetrahedron 2015;72(25):3609-3624. https://doi.org/10.1016/j.tet.2015.09.069 [ Links ]
3. Li HK, Agweyu A, English M, Bejon P. An unsupported preference for intravenous antibiotics. PLoS Med 2015;12(5)e1001825. https://doi.org/10.1371/journal.pmed.1001825 [ Links ]
4. McCarthy K, Avent M. Oral or intravenous antibiotics? Aust Prescr 2020;43(2):45-48. https://doi.org/10.18773/austprescr.2020.008 [ Links ]
5. Kapoor G, Saigal S, Elongavan A. Action and resistance mechanisms of antibiotics: A guide for clinicians. J Anaesthesiol Clin Pharmacol 2017;33(3):300-305. https://doi.org/10.4103/joacp.JOACP_349_15 [ Links ]
6. Landersdorfer CB, Gwee A, Nation RL. Clinical pharmacological considerations in an early intravenous to oral antibiotic switch: Are barriers real or simply perceived? Clin Microbiol Infect 2023;29(9):1120-1125. https://doi.org/10.1016/j.cmi.2023.04.009 [ Links ]
7. Skosana P, Schellack N, Godman B, et al. A point prevalence survey of antimicrobial utilisation patterns and quality indices amongst hospitals in South Africa: Findings and implications. Expert Rev Anti Infect Ther 2021;19(10):1353-1366. https://doi.org/10.1080/14787210.2021.1898946 [ Links ]
8. Tamma PD, Avdic E, Li DX, Dzintars K, Cosgrove SE. Association of adverse events with antibiotic use in hospitalised patients. JAMA Intern Med 2017;177(9):1308-1315. https://doi.org/10.1001/jamainternmed.2017.1938 [ Links ]
9. Collignon PC, Conly JM, Andremont A, et al. World Health Organization ranking of antimicrobials according to their importance in human medicine: A critical step for developing risk management strategies to control antimicrobial resistance from food animal production. Clin Infect Dis 2016;63(8):1087-1093. https://doi.org/10.1093/cid/ciw475 [ Links ]
10. World Health Organization. Antibiotic resistance. WHO fact sheet. https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed 15 April 2022). [ Links ]
11. Jadimurthy R, Mayegowda SB, Nayak SC, Mohan CD, Rangappa KS. Escaping mechanisms of ESKAPE pathogens from antibiotics and their targeting by natural compounds. Biotechnol Rep (Amst) 2022;34:e00728. https://doi.org/10.1016/j.btre.2022.e00728 [ Links ]
12. World Health Organization. New report calls for urgent action to avert antimicrobial resistance crisis. 29 April 2019. https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis (accessed 21 February 2024). [ Links ]
13. Shabangu K, Essack SY, Duma SE. Barriers to implementing national action plans on antimicrobial resistance using a One Health approach: Policymakers' perspectives from South Africa and Eswatini. J Glob Antibicrob Resist 2023;33:130-136. https://doi.org/10.1016/j.jgar.2023.02.007 [ Links ]
14. World Health Organization. 2021 AWaRe classification. WHO Access, Watch, Reserve classification of antibiotics for evaluation and monitoring of use. 30 September 2021. https://www.who.int/publications/i/item/2021-aware-classification (accessed 19 May 2023). [ Links ]
15. Abbasinazari M, Hajhossein Talasaz A, Mousavi Z, Zare-Toranposhti S. Evaluating the frequency of errors in preparation and administration of intravenous medications in orthopedic, general surgery and gastroenterology wards of a teaching hospital in Tehran. Iran J Pharm Res 2013;12(1):229-234. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3813204/ (accessed 2 October 2023). [ Links ]
16. Tefera GM, Sileshi T, Mekete MD, Umeta GT. Opportunities, associations, and impact of early intravenous to oral antimicrobial switch for hospitalised patients in Ethiopia. SAGE Open Med 2023;11:e20503121231161192. https://doi.org/10.1177/20503121231161192 [ Links ]
17. Boyles TH, Brink A, Calligaro GL, et al. South African guideline for the management of community-acquired pneumonia in adults. J Thorac Dis 2017;9(6):1469-1502. https://doi.org/10.4102/sajid.v33i1.22 [ Links ]
18. Government of South Australia. IV to oral switch clinical guideline for adult patients: Can antibiotics S.T.O.P.? https://www.sahealth.sa.gov.au/wps/wcm/connect/86d0af8047ca4a108ca28dfc651ee2b2/Clinical_Guideline_IV+to+Oral_Switch_v1.1_06.06.2019.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-86d0af8047ca4a108ca28dfc651ee2b2-oC--qMV (accessed 20 August 2023). [ Links ]
19. Cyriac JM, James E. Switch over from intravenous to oral therapy: A concise overview. J Pharmacol Pharmacother 2014;5(2):83-87. https://doi.org/10.4103/0976-500X.130042 [ Links ]
20. Tamilselvan T. Influence of intravenous to oral antibiotic conversion and its practice in a tertiary care hospital. Saudi J Med Pharm Sci 2021;7(3):160-164. https://doi.org/10.36348/sjmps.2021.v07i03.002 [ Links ]
21. Broom J, Broom A, Adams K, Plage S. What prevents the intravenous to oral antibiotic switch; A qualitative study of hospital doctors' accounts of what influences their clinical practice. J Antimicrob Chemother 2016;71(8):2295-2299. https://doi.org/10.1093/jac/dkw129 [ Links ]
22. Battula V, Krupanandan RK, Nambi PS, Ramachandran B. Safety and feasibility of antibiotic de-escalation in critically ill children with sepsis - a prospective analytical study from a pediatric ICU. Original Research. Front Pediatr 2021;9:640857. https://doi/org/10.3389/fped.2021.640857 [ Links ]
23. Alanazi A, Almuhaya R, Almohaimeed M, et al. Impact of antibiotic de-escalation on antibiotic consumption, length of hospitalisation, mortality, and cost: A systematic review and meta-analysis. Pharmacoepidemiology 2023;2(4):289-306. https://doi.org/10.3390/pharma2040025 [ Links ]
24. Umpleby H, Dushianthan A, Catton T, Saeed K. Antimicrobial stewardship programmes focused on de-escalation: A narrative review of efficacy and risks. J Emerg Crit Care Med 2022;6:23. https://doi.org/10.21037/jeccm-22-6 [ Links ]
25. Woods RJ, Read AF. Combination antimicrobial therapy to manage resistance. Evol Med Public Health 2023;11(1):185-186. https://doi.org/10.1093/emph/eoad005 [ Links ]
26. Schellack N, Bronkhorst E, Coetzee R, et al. SASOCP position statement on the pharmacist's role in antibiotic stewardship 2018. South Afr J Infect Dis 2018;33(1);28-35. https://doi.org/10.4102/sajid.v33i1.24 [ Links ]
27. Stordeur F, Miliani K, Lacavé L, et al. How to measure hospital antibiotic consumption: Comparison of two methods from data surveillance in France. JAC Antimicrob Resist 2020;2(3):dlaa059. https://doi.org/10.1093/jacamr/dlaa059 [ Links ]
28. World Health Organization. Antimicrobial stewardship programmes in health-care facilities in low-and middle-income countries: A WHO practical toolkit. 22 October 2019. https://www.who.int/publications/i/item/9789241515481 (accessed 7 December 2023). [ Links ]
29. Nguyen JK, Hoxhallari E, Daffy J. An unusual case of Escherichia coli cellulitis and bacteremia in an immunocompetent patient. Dermatol Rep 2023;15(2)9603. https://doi.org/10.4081/dr.2023.9603 [ Links ]
30. Rabiei H, Malakoutikhah M, Vaziri MH, Sahlabadi AS. The prevalence of musculoskeletal disorders among miners around the world: A systematic review and meta-analysis. Iran J Public Health 2021;50(4):676-688. https://doi.org/10.18502/ijph.v50i4.5992 [ Links ]
31. Naidoo RN. Mining: South Africa's legacy and burden in the context of occupational respiratory diseases. Glob Health Action 2013;6(1). https://doi.org/10.3402/gha.v6i0.20512 [ Links ]
32. Mugada V, Mahato V, Andhavaram D, Vajhala SM. Evaluation of prescribing patterns of antibiotics using selected indicators for antimicrobial use in hospitals and the Access, Watch, Reserve (AWaRe) classification by the World Health Organization. Turk J Pharm Sci 2021;18(3):282-288. https://doi.org/10.4274/tjps.galenos.2020.11456 [ Links ]
33. Mendelson M, Morris AM, Thursky K, Pulcini C. How to start an antimicrobial stewardship programme in a hospital. Clin Microbiol Infect 2020;26(4):447-453. https://doi.org/10.1016/j.cmi.2019.08.007 [ Links ]
34. Matuluko A, Macdonald J, Ness V, Currie K. Interventions to improve the review of antibiotic therapy in acute care hospitals: A systematic review and narrative synthesis. JAC Antimicrob Resist 2020;2(3):dlaa065. https://doi.org/10.1093/jacamr/dlaa065 [ Links ]
35. De Waele JJ, Schouten J, Beovic B, Tabah A, Leone M. Antimicrobial de-escalation as part of antimicrobial stewardship in intensive care: No simple answers to simple questions - a viewpoint of experts. Intensive Care Med 2020;46(2):236-244. https://doi.org/10.1007/s00134-019-05871-z [ Links ]
36. Khumra S, Mahony AA, Stewart K, Bergen PJ, Elliott RA. Coaching ward pharmacists in antimicrobial stewardship: A pilot study. Explor Res Clin Soc Pharm 2022;5:100131. https://doi.org/10.1016/j.rcsop.2022.100131 [ Links ]
 Correspondence:
Correspondence:
J M du Plessis
jesslee.duplessis@nwu.ac.za
Received 3 September 2024
Accepted 16 April 2025

{kind=link}
{kind=link}
{kind=link}
{kind=link}