










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.115 n.11 Pretoria 2025
https://doi.org/10.7196/SAMJ.2025.v115i11.2565
IN PRACTICE
New case definitions and thresholds for environmental notifiable medical conditions in South Africa: Pesticide, lead and mercury poisoning
A MatheeI; C StephenII; S A NzenzeIII; L ChanduIV
IPhD, MSc; Environment and Health Research Unit, South African Medical Research Council, and Environmental Health Department, Faculty of Health Sciences, University of Johannesburg, South Africa
IIMB ChB, DCH (SA); Poisons Information Centre, Red Cross War Memorial Children's Hospital, and Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
IIIMB ChB, PhD; Division of Public Health Surveillance and Response, National Institute for Communicable Diseases, National Health Laboratory Service, Johannesburg, South Africa
IVMPH, MSc (Med); Division of Public Health Surveillance and Response, National Institute for Communicable Diseases, National Health Laboratory Service, Johannesburg, South Africa
ABSTRACT
Notifiable medical conditions (NMCs) are diseases that pose significant public health risks, and may result in outbreaks, epidemics or pandemics with high morbidity and mortality rates. The World Health Organization provides an overarching framework for countries to meet obligations related to data collection, processing and notification of and rapid response to, as needed, cases of NMCs. South Africa has recently introduced new case definitions for the three NMCs related to environmental exposures: poisoning by agricultural or stock remedies (pesticides), lead and mercury. In this article, the revised case definitions and processes for reporting of NMCs are outlined. We also discuss the benefits and challenges of processing and using NMC data, and urge more widespread and effective participation in the process of notifying these important environmental medical conditions.
Keywords: environmental notifiable medical conditions, South Africa, lead, mercury, pesticide poisoning
Notifiable medical conditions (NMCs) are diseases that pose significant public health risks, and may result in outbreaks, epidemics or pandemics with high morbidity and mortality rates. Diagnosing clinicians and laboratories are legally obligated to report NMCs to government health authorities. The World Health Organization (WHO)'s International Health Regulations (IHR) of 2005 provide an overarching global legal framework that defines member countries' obligations in handling public health events that have the potential to traverse borders. This includes notification to the WHO of any event that may constitute a public health emergency of international concern.[1] In South Africa (SA), the legal basis for disease notification is the National Health Act 61 of 2003, coupled with the 'Regulations relating to the surveillance and control of notifiable medical conditions'.[2] These regulations also prescribe the roles and responsibilities of various stakeholder groups. Operational responsibility for the NMC system in SA has been devolved to the National Institute for Communicable Diseases (NICD),[3] with oversight from the National Department of Health.
The notifiable medical conditions process
In SA, 56 NMCs for human health are legislated through the National Health Act. They are categorised according to the reporting time requirements: category 1 requires reporting within 24 hours; category 2 and 3 conditions need to be reported within 7 days, while category 4 conditions are required to be reported within 1 month of diagnosis. The categories are indicative of the level of urgency of the requisite public health responses. Healthcare providers (public and private) are mandated to notify suspected or confirmed cases of NMCs according to standardised case definitions and using prescribed forms and tools.[2] In 2018, the NMC system was revitalised through the institution of an electronic, real-time reporting application (web-based and mobile) to facilitate rapid reporting and public health action. Since then, notifications occur predominantly through electronic mechanisms, such as mobile or web-based electronic applications, which require prior registration and authorisation (https://nmc.nicd.ac.za). The relatively small proportion of healthcare providers using paper-based notification systems do so via email, facsimile or WhatsApp. The results are captured manually at the NICD, potentially incurring delays. Data captured electronically by an authorised healthcare provider are transferred directly to the NMC system's data mart. Currently, the NMC system receives daily direct feed of laboratory-confirmed notifications within the public sector (Appendix Fig. S1 shows a summary of the NMC data flow of the notification process). Data transferred to the NMC system's data mart from clinicians or laboratories are immediately accessible to all relevant focal persons at health establishments at sub-district, district, provincial and national levels, for rapid public health response.
Studies in Taiwan have shown that electronic NMC reporting systems were associated with improved timeliness, greater accuracy and increased convenience.[4] Similarly, in a controlled before-and-after trial in Indiana (USA), electronic case reporting was found to be effective in improving notifiable disease reporting rates, as well as the completeness of the information submitted.[5] A study in north-eastern Nigeria likewise showed a significant increase in the number of health facilities reporting NMC cases, and in the timeliness of reporting, following the implementation of a regional electronic NMC system. Interviews with key stakeholders revealed greater satisfaction with the electronic NMC system,[6] and perceptions of its superiority. In addition, daily notifications of NMCs were shown to be a success factor in NMC systems reporting.[7] These consistently positive views of electronic NMC systems raise expectations of similarly significant improvements in SA.
Environmental notifiable medical conditions
SA has three environmental NMCs: agricultural or stock remedy (pesticide) poisoning, lead poisoning and mercury poisoning. Pesticide poisoning has recently been upgraded from a category 2 to a category 1 condition, requiring notification within 24 hours of clinical or laboratory diagnosis by private or public healthcare providers or laboratories. Lead poisoning and mercury poisoning are classified as category 2, and need to be notified within 7 days.[2] Healthcare providers are required to provide clinical and demographic details of the case(s) notified. These details support case investigations performed by environmental health practitioners (EHPs) in line with prescribed guidelines[8] to facilitate remediation and the prevention of further poisoning cases.
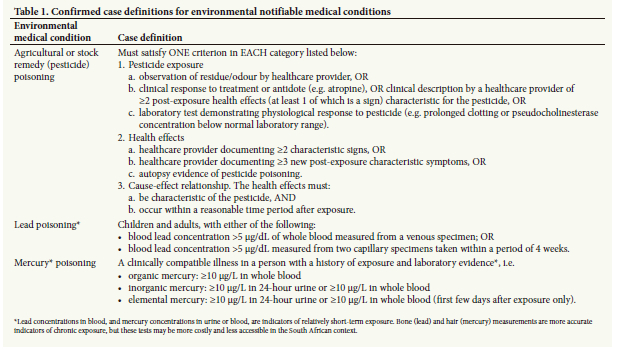
The new case definitions for agricultural or stock remedy (pesticide) poisoning, lead poisoning and mercury poisoning provide definitions for suspected, probable and confirmed cases.[9] Table 1 provides the confirmed case definitions for agricultural or stock remedy (pesticide), lead, mercury and pesticide poisoning.
Weaknesses of the notifiable medical conditions surveillance system
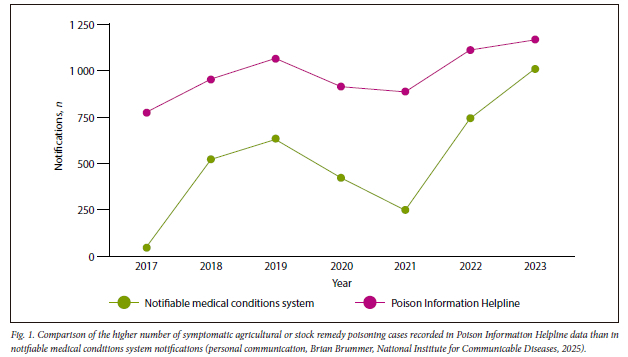
Numerous evaluations of the SA NMC surveillance system point to incompleteness of the data set due to low levels of knowledge of the NMC reporting requirements among health personnel, incorrect or incomplete reporting of data and discrepancies between data in the NMC system and laboratory reports.[10-13] Fig. 1 compares the higher number of symptomatic agricultural or stock remedy poisoning cases recorded in Poison Information Helpline data with the number of NMC notifications during the same time period. These weaknesses compromise the utility of the NMC system as a valuable public health tool, especially for environmental NMCs, which continue to constitute important public health concerns, especially in settings of poverty. In this article we describe the new case definitions and thresholds for pesticide, lead and mercury poisoning, and call for increased awareness and stricter adherence to the NMC process by all relevant stakeholders.
Background to poisoning by stock remedies (pesticide), lead and mercury
Agricultural or stock remedies (pesticides)
Agricultural or stock remedies, known collectively as pesticides, include any chemical substance, or mixture of chemicals, intended to kill, repel or control forms of plant or animal life considered to be pests, or to regulate plant growth. Pesticides include herbicides, insecticides, fungicides, rodenticides and repellents, and some pesticides can remain in soil and water for years.
Pesticides are potentially toxic to humans and the environment, and can have both acute and chronic health effects, depending on the type of pesticide, the quantity and routes of exposure. Pesticide poisoning can be classified as occupational if exposure occurs while at work, or non-occupational, which includes non-intentional or accidental exposures at home, as well as all cases involving suicide or self-harming behaviour.
Pesticides may cause life-threatening symptoms or death, particularly highly hazardous pesticides such as organophosphates (insecticide), aluminium phosphide (rodenticide) or paraquat (herbicide). Symptoms vary widely according to the type of pesticide and exposure, and include vomiting, abdominal pain, burning of the skin, respiratory difficulty, nervous system instability, cardiovascular collapse and bleeding tendencies.
In SA, acute pesticide poisoning is a persistent and prevalent health issue, leading to considerable morbidity and mortality.[14-17] It is frequently observed in agricultural communities owing to the ready availability and ease of access to pesticides. Additionally, individuals living in poorer urban socioeconomic conditions, where pest infestations are widespread, also experience the detrimental effects of pesticide poisoning. Unregistered pesticides are informally distributed in these communities, and these products often possess significant toxicity and are not intended for domestic use.[18]
The NMC case definitions for agricultural or stock remedy poisoning include all symptomatic patients with a plausible history of, and appropriate clinical findings associated with, pesticide exposure, and refer mainly to acute exposures.
Case study 1: Pesticide poisoning
A family living in greater Cape Town, SA, welcomed a new baby to their home early in 2023, and owing to the presence of rats in the house, the child's father bought a rodenticide from a local store, which he placed in all rooms of the house. The following morning, five family members presented to the local emergency department with gastrointestinal symptoms of diarrhoea, vomiting and abdominal pain. They were treated and began to improve, but the clinical condition of the 4-week-old baby suddenly deteriorated, as she developed severe difficulty breathing and heart failure. Despite extensive supportive treatment, including artificial ventilation, the baby died a few hours later. The remaining family members recovered, with only a transient reduction in white blood cell counts. Case notifications were submitted through the NICD NMCs app, and an investigation by local EHPs identified the rodenticide QuickPhos (aluminium phosphide), an extremely toxic pesticide reserved only for registered pest control agents, as the cause of the poisoning (personal communication, Cindy Stephen, 2024).
Lead poisoning
Even at very low concentrations in blood, lead is a potent neurotoxin, and causes harm to virtually all organ systems. In a systematic review of the blood lead concentrations of children in developing countries published in 2021, it was estimated that 7.8 million SA children aged between 0 and 14 years had blood lead concentrations >5 μg/dL (the new threshold concentration for reporting a case of lead poisoning through the NMC system in SA), while 4.7 million children had blood lead concentrations >10 μg/dL.[19] These estimates are poorly reflected in the SA NMC system, where only three cases of lead poisoning were reported in the 5-year period between 2018 and 2022; by contrast, the national Poisons Information Helpline (PIH) fielded 22 calls[20] related to lead poisoning, and epidemiological investigations conducted over the same period revealed at least 737 cases with blood lead concentrations >5 μg/dL.[21-23]
Case study 2: Lead poisoning
An epidemiological study[22] was undertaken among male children incarcerated for both violent and non-violent crimes in Gauteng Province juvenile detention centres. Blood lead concentrations in this group ranged from 1.7 to 48.1 μg/dL, with the mean (standard deviation) concentration 5.5 (6.4) μg/dL. Of the total sample of 192 children, 34% had blood lead concentrations >5 μg/dL. Children convicted of violent offences had significantly elevated blood lead concentrations relative to those convicted of non-violent crimes. Case histories showed that the highest blood lead concentrations were found in children with a history of working on decommissioned mining land to extract residual gold. Nonspecific symptoms such as headaches, gastrointestinal pain and muscle weakness, which are often associated with lead poisoning, were reported by children with elevated blood lead concentrations.[22,24] None of the children included in the study had received a blood lead test, despite their history of involvement in artisanal mining.
Health economists have indicated that around 8.9% of sub-Saharan gross domestic product is lost annually due to lost intelligence quotient (IQ) points and to mortality from cardiovascular disease associated with lead exposure.[25] Settings and activities currently associated with elevated lead exposure in SA include subsistence fishing, the use of firearms and ammunition, traditional medicines, the use of aluminium cooking pots crafted from waste products, low-cost alcoholic beverages, mining operations (including artisanal mining), worker and para-occupational exposure (pollutants transferred from workplaces into homes) in lead-related industries and old lead-based paint applied to toys, furniture and older housing.[26,27]
Mercury poisoning
Mercury is a naturally occurring element, with a wide range of anthropogenic applications, including in medical equipment (such as sphygmomanometers and thermometers), electrical switches, fluorescent light bulbs, coal-fired power plants, cement production, batteries, biocides and pesticides, skin lightening creams and dental amalgam filling. The use of mercury is also widespread in the informal sector, including in artisanal gold mining and in the production of traditional medicines in SA.[28] Elevated mercury concentrations have been measured in environmental samples around SA landfill sites,[29] in polluted river systems, such as the Olifants River barrage[30] and the Inanda Dam,[31,32] and in communities with high levels of fish consumption.[33] Mercury is a neurotoxin associated with a variety of neurological effects. Typical symptoms of mercury poisoning include headaches, numbness and tingling of the hands and feet (peripheral neuropathy), visual difficulties, loss of hearing, tremors, unsteady gait, skin rash and emotional and cognitive difficulties.
Case study 3: Mercury poisoning
During 2023, a toddler was admitted to hospital in the Western Cape Province as his mother was increasingly concerned about his overall wellbeing. During the preceding 3 months the child had ceased playful activities and experienced weight loss, lethargy, constipation and intermittent episodes of fever. On admission, the toddler was drooling and preferred to lie down. Physical examination revealed age-appropriate growth but global weakness, pronounced head lag and an unsafe swallow. Concurrently, a red, desquamating rash on the hands and feet was noted. A comprehensive battery of tests and imaging studies was performed, involving consultations with surgical, neurological and dermatological specialists. Subsequently, a diagnosis of mercury poisoning was considered, and this was substantiated by a urine test showing a markedly elevated mercury concentration of 261 μg/L (notifiable at >10 μg/L). The child was eligible for chelation therapy, and after a protracted section 21 process, dimercaptopropane sulfonate was procured, and administered in daily doses over a 5-day period. He responded well, and within a few months he was running and playing, and the drooling had resolved. The case was notified through the NMC system as an instance of mercury poisoning, and home visits were conducted by EHPs and healthcare workers. These visits identified potential sources of both mercury and lead exposure, including the heating of elemental mercury to clean jewellery, electronic appliance repair using lead solder and the manufacture of 'tik' (methamphetamine) pipes from broken fluorescent tubes (personal communication, Cindy Stephen, 2024).
Discussion
Agricultural or stock remedy (pesticide), lead and mercury poisoning continue to constitute important public health risks in SA, associated with morbidity and mortality, from both intentional and unintentional exposures. A well-designed and operated NMC system offers an invaluable tool for tracking, analysis and response to cases or patterns of key diseases, and specific environmental poisonings. The NMC system represents a relatively low-cost public health tool for the rapid identification of cases or outbreaks, and swift intervention.
Despite data from 2023 indicating the possibility of a slight uptick in reports to the NMC system, regrettably, levels of adherence among key stakeholders to the NMC processes continue to be very low, as illustrated by significant discrepancies between cases reported through the NMC system on one hand, and epidemiological studies and calls to the national Poisons Information Helpline on the other. The key concerns include inadequate awareness and understanding among healthcare workers, and especially medical practitioners, of the NMC system and the obligatory processes to be followed. A lack of timeous public health responses to the data reported may also contribute to the suboptimal value currently being derived from the NMC system.
The revitalisation of the NMC system, and the finalisation of case definitions and thresholds for the environmental NMCs, presents an opportunity to issue a call for increased attention and observance among all stakeholders of the NMC system to optimise its public health value. There is a need for boosted education and training campaigns to increase awareness and knowledge of the system, and the concomitant legal obligations of healthcare practitioners. It is hoped that adherence levels will be amplified by the introduction of electronic mechanisms for reporting (including by smartphone and the internet), and the capacity for real-time data analysis.
With regard to the environmental NMCs (agricultural or stock remedy (pesticides), lead and mercury poisoning), the NMC system constitutes a powerful platform for the identification of high-risk locations, settings and groups. When coupled with the recent publication of guidelines[8] for EHPs to investigate the sources, pathways of exposure and sociobehavioural risk factors associated with agricultural or stock remedy (pesticide), lead and mercury poisoning, the NMC system presents an important opportunity for deeper understanding of the role and nature of environmental exposures in public health outcomes. High levels of health practitioner adherence to NMC reporting are essential, and this may be encouraged by energetic, timely and thorough responses from EHPs.
Data availability. N/a.
Declaration. None.
Acknowledgements. We acknowledge the role of the National Institute for Communicable Diseases in initiating this work.
Author contributions. All authors conceptualised the article; AM prepared the first draft with significant critical input from SN, CS and LC. All authors reviewed and approved the final draft.
Funding. We acknowledge the direct and/or in-kind financial support received from the South African Medical Research Council, the National Institute for Communicable Diseases and the Poisons Information Helpline of the Western Cape.
Conflicts of interest. None.
References
1. World Health Organization. International Health Regulations 2005. 3rd ed. Geneva: WHO, 2016. www.who.int/publications/i/item/9789241580496 (accessed 24 July 2024). [ Links ]
2. National Department of Health, South Africa. Regulations relating to the surveillance and the control ofnotifiable medical conditions, 2017. Government Gazette No. 604. https://www.gov.za/sites/default/files/gcis_document/201706/40945gon604.pdf (accessed 24 July 2024). [ Links ]
3. National Institute for Communicable Diseases. Overview. Johannesburg: NICD, 2023. https://www.nicd.ac.za/nmc-overview (accessed 24 July 2024). [ Links ]
4. Lee LH, Chuang JH, Wu, YC, et al. Factors influencing the effectiveness of adopting electronic medical record-based reporting systems for notifiable disease surveillance: A quantitative analysis. J Med Syst 2023;47:70. https://doi.org/10.1007/s10916-023-01971-y [ Links ]
5. Dixon BE, Zhang Z, Arno JN, et al. Improving notifiable disease case reporting through electronic information exchange - facilitated decision support: A controlled before-and-after trial. Public Health Rep 2020;135(3):401-410. https://doi.org/10.1177/0033354920914318 [ Links ]
6. Ibrahim LM, Okudo I, Stephen M, et al. Electronic reporting of integrated disease surveillance and response: lessons learned from northeast, Nigeria, 2019. BMC Public Health 2021;21:916. https://doi.org/10.1186/s12889-021-10957-9 [ Links ]
7. Meckawy R, Stuckler D, Mehta A, et al. Effectiveness of early warning systems in the detection of infectious diseases outbreaks: A systematic review. BMC Public Health 2022;22:2216. https://doi.org/10.1186/s12889-022-14625-4 [ Links ]
8. National Department of Health, South Africa. Guidelines for investigation and environmental control of human chemical exposure and poisoning cases, 2022. Pretoria: NDoH, 2022. https://www.health.gov.za/wp-content/uploads/2023/09/DOH-Guideline-Investigation-Human-Chemical-Poisoning-1.pdf (accessed 24 July 2024). [ Links ]
9. National Institute for Communicable Diseases. Notifiable medical conditions (NMC) case definitions flipchart 2021. Johannesburg: NICD, 2021. https://www.nicd.ac.za/wp-content/uploads/2023/06/Updated_NMC_category-2-case-definitions_Flipchart_01October-2021_29May2023.docx.pdf (accessed 25 July 2024). [ Links ]
10. Karim SA, Dilraj A. Reasons for under-reporting of notifiable conditions S Afr Med J 1996;86(7):834-836. https://www.researchgate.net/publication/14437641_Reasons_for_under-reporting_of_notifiable_conditions (accessed 24 July 2024). [ Links ]
11. Nkgudi B, Robertson KA, Volmink J, Mayosi BM. Notification of rheumatic fever in South Africa -evidence of underreporting by healthcare professionals and administrators. S Afr Med J 2006;96(3):206-208. https://journals.co.za/doi/epdf/10.10520/EJC68680 (accessed 24 July 2024). [ Links ]
12. Benson F, Musekiwa A, Blumberg L, Rispel L. Comparing laboratory surveillance with the notifiable diseases surveillance system in South Africa. Int J Infect Dis 2017;59:141-147. http://doi.org/10.1016/j.ijid.2017.03.007 [ Links ]
13. Morifi M, Malevu N, Odayan S, McCarthy K, Kufa T. Congenital syphilis case surveillance in South Africa 2017 - 19: Experience, challenges and opportunities. J Trop Ped 2021;67(4):1-11. https://doi.org/10.1093/tropej/fmab079 [ Links ]
14. Dippenaar R, Diedericks RJ. Paediatric organophosphate poisoning - a rural hospital experience. S Afr Med J 2005;95(9):678-681. https://hdl.handle.net/10520/EJC68552 (accessed 7 November 2025). [ Links ]
15. Balme KH, Roberts JC, Glasstone M, et al. Pesticide poisonings at a tertiary children's hospital in South Africa: An increasing problem. Clin Toxicol 2010;48(9):928-934. https://doi.org/10.3109/15563650.2010.534482 [ Links ]
16. Veale DJ, Wium CA, Muller GJ. Amitraz poisoning in South Africa: A two year survey (2008 - 2009). Clin Toxicol 2011;49(1):40-44. https://doi.org/10.3109/15563650.2010.542159 [ Links ]
17. Davies B, Hlela MBKM, Rother HA. Child and adolescent mortality pesticide toxicity in Cape Town, South Africa, 2010 - 2019: A retrospective case review. BMC Public Health 2023;23(1):792. https://doi.org/10.1186/s12889-023-15652-5 [ Links ]
18. Rother H-A. Falling through the regulatory cracks: Street selling of pesticides and poisoning among urban youth in South Africa. Int J Occup Environ Health 2010;16(2):183-194. https://doi.org/10.1179/107735210799160264 [ Links ]
19. Ericson B, Hu H, Nash E, et al. Blood lead levels in low-income and middle-income countries: A systematic review. Lancet Planet Health 202;5(3):e145-e153. https://doi.org/10.1016/S2542-5196(20)30278-3 [ Links ]
20. Stephen CR. Poisons Information Helpline of the Western Cape (PIHWC) Annual Review, 2019. Cape Town: PIHWC, 2021. https://health.uct.ac.za/sites/default/files/media/documents/health_uct_ac_za/547/poisons_information_helpline_annual_review_2019_1.pdf (accessed 29 July 2024). [ Links ]
21. Nkomo P, Naicker N, Mathee A, et al. The association between environmental lead exposure with aggressive behavior, and dimensionality of direct and indirect aggression during mid-adolescence: Birth to Twenty Plus cohort. Sci Total Env 2018;612:472-479. https://doi.org/10.1016/j.scitotenv.2017.08.138 [ Links ]
22. Mbonane TP, Mathee A, Swart A, Naicker N. Lead poisoning among male juveniles due to illegal mining: A case series from South Africa. Int J Environ Res Public Health 2021;18(13):6838. https://doi.org/10.3390/ijerph18136838 [ Links ]
23. Mathee A, Haman T, Nkosi V, Naicker N, Street R. Elevated soil and blood lead levels with increasing residential proximity to a mine tailings facility in Soweto, South Africa. Sci Total Env 2022;851(Pt 1):158158. https://doi.org/10.1016/j.scitotenv.2022.158158 [ Links ]
24. Mbonane TP. Prevalence of blood lead levels and its association with violent criminal behaviour amongst young males in conflict with the law. Doctoral thesis. Johannesburg: University of Johannesburg, 2022. https://hdl.handle.net/10210/502090 (accessed 25 July 2024). [ Links ]
25. Larsen B, Sánchez-Triana E. Global health burden and cost of lead exposure in children and adults: A health impact and economic modelling analysis. Lancet Planet Health 2023;7(10):e831-e840. https://doi.org/10.1016/S2542-5196(23)00166-3 [ Links ]
26. Mathee A. Towards the prevention of lead exposure in South Africa: Contemporary and emerging challenges. Neurotox 2014;45:220-223. https://doi.org/10.1016/j.neuro.2014.07.007 [ Links ]
27. Mathee A, Street R, Teare J, Naicker N. Lead exposure in the home environment: An overview of risks from cottage industries in Africa. Neurotox 2020;81:34-39. https://doi.org/10.1016/j.neuro.2020.08.003C [ Links ]
28. Street RA, Kabera GM, Connolly C. Metallic mercury use by South African traditional health practitioners: Perceptions and practices. Environ Health 2015;14:67. https://doi.org/10.1186/s12940-015-0053-4 [ Links ]
29. Daso A, Nevondo V, Okonkwo O, Malehase T. Leachate seepage from landfill: A source of groundwater mercury contamination in South Africa. Water SA 2019;45(No. 2):225-231. https://doi.org/10.4314/wsa.v45i2.09 [ Links ]
30. Verhaert V, Teuchies J, Vlok W, et al. Bioaccumulation and trophic transfer of total mercury in the subtropical Olifants River Basin, South Africa. Chemosphere 2019;216:832-843. https://doi.org/10.1016/j.chemosphere.2018.10.211 [ Links ]
31. Oosthuizen J, Ehrlich R. The impact of pollution from a mercury processing plant in KwaZulu-Natal, South Africa, on the health of fish-eating communities in the area: An environmental health risk assessment. Int J Environ Health Res 2001;11(1):41-50. https://doi.org/10.1080/09603120020019638 [ Links ]
32. Papu-Zamxaka V, Mathee A, Harpham T, et al. Elevated mercury exprosure in communities living alongside the Inanda Dam, South Africa. J Environ Monit 2010;12(2):472-477. https://doi.org/10.1039/B917452D [ Links ]
33. Channa K, Odland J0, Kootbodien T, et al. Differences in prenatal exposure to mercury in South African communities residing along the Indian Ocean. Sci Total Env 2013;463-464:11-19. https://doi.org/10.1016/j.scitotenv.2013.05.055 [ Links ]
 Correspondence:
Correspondence:
A Mathee
amathee@mrc.ac.za
Received 23 August 2024
Accepted 13 June 2025

{kind=link}
{kind=link}