










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.116 n.1 Pretoria Feb. 2026
https://doi.org/10.7196/SAMJ.2025.v116i1.2304
RESEARCH
Engagement in antenatal and HIV care among pregnant women before and after Option B+ policy implementation in South Africa
C HwangI, II; N JingaIII; M DhedaIV; O MhlongoV; P PhungulaVI; K ClouseVII, VIII, IX; M D HuffmanX, XI; M P FoxXII, XIII, XIV; M MaskewXV
IMD; Health Economics and Epidemiology Research Office, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMD; Department of Internal Medicine, Stanford University School of Medicine, Stanford, USA
IIIMPhil; Health Economics and Epidemiology Research Office, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVB Pharm; National Department of Health Pharmacovigilance Centre for Public Health Programmes, Pretoria, South Africa
VB Cur, Diploma Gen; KwaZulu-Natal Department of Health, Pietermaritzburg, South Africa
VIB Cur Advanced Midwifery; KwaZulu-Natal Department of Health, Pietermaritzburg, South Africa
VIIPhD; Health Economics and Epidemiology Research Office, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIIPhD; Vanderbilt University School of Nursing, Nashville, USA
IXPhD; Vanderbilt Institute for Global Health, Vanderbilt University Medical Center, Nashville, USA
XMD, MPH; Division of Cardiology, Department of Medicine, Washington University School of Medicine, St. Louis, USA
XIMD, MPH; The George Institute for Global Health, University of New South Wales, Sydney, Australia
XIIDSc, MPH; Health Economics and Epidemiology Research Office, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XIIIDSc, MPH; Department of Global Health, Boston University School of Public Health, Boston, USA
XIVDSc, MPH; Department of Epidemiology, Boston University School of Public Health, Boston, USA
XVMB BCh, PhD; Health Economics and Epidemiology Research Office, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Substantial gains have been made in South Africa (SA) in the prevention of vertical transmission of HIV over the past decade
OBJECTIVE: To determine whether engagement in antenatal and HIV care among pregnant women living with HIV (WLWH) differed after Option B+ implementation
METHODS: We analysed cohort data from a pregnancy and birth defects surveillance system in KwaZulu-Natal (KZN). We report on two co-primary outcomes related to engagement in HIV care: (i) timing and number of antenatal care (ANC) visits during the pregnancy period; and (ii) timing of antiretroviral therapy (ART) initiation (both self-reported ART use in interviews and observed initiation of treatment in maternal records). The association of policy era on the timing of ANC presentation was assessed using log-binomial regression modelling. We also report proportions initiating ART before or during pregnancy stratified by policy era
RESULTS: Data from 40 357 women, including 16 016 (40%) WLWH were analysed. During the Option B+ era, 24% of pregnant WLWH attended their first antenatal care visit during the first trimester, compared with 16% during the Option B era (relative risk 1.52; 95% confidence interval 1.41 - 1.64). The proportion of WLWH who initiated ART prior to pregnancy was also higher during the Option B+ era than the Option B era, though this result was limited by missing data
CONCLUSION: Engagement in antenatal and HIV care improved after Option B+ implementation. In the Option B+ era, SA has made significant progress toward the goal of eliminating mother-to-child transmission of HIV
Keywords: antenatal, mother-to-child transmission, HIV, pregnancy, women, antiretroviral therapy, Option B
Substantial gains have been made in South Africa (SA) in the prevention of vertical transmission of HIV over the past decade, but the elimination of mother-to-child transmission of HIV (MTCT) has not yet been achieved. The national estimate of early MTCT was 2.6% in 2012 - 2013.[1] By 2015, it was reduced to 1.4% at 6 weeks postpartum and 2% at 18 months.[2] National surveys by the South African Medical Research Council (SAMRC) and Centers for Disease Control and Prevention showed that between 2010 and 2015, the prevention of MTCT of HIV (PMTCT) programme in SA prevented ~80 000 - 85 000 newborn infections per year.[2]
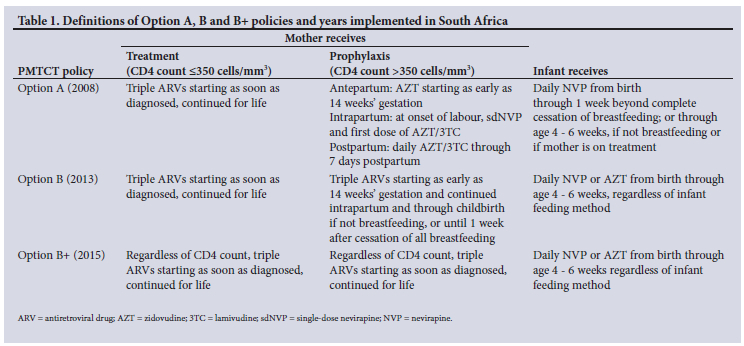
SA's policy for providing antiretroviral therapy (ART) to pregnant women living with HIV (WLWH) has evolved over time, following World Health Organization (WHO) recommendations (Table 1). In April 2008, a dual-therapy PMTCT programme was implemented through which women were offered zidovudine starting at 28 weeks' gestation, or ART at a CD4 count <200 cells/μL.[3] Option A was introduced with zidovudine given starting at 14 weeks' gestation for women with a CD4 count >350 cells/μL, or triple-drug ART for women with a CD4 count <350 cells/μL.[4] Option A was replaced in 2013 by the WHO-recommended Option B approach, where women were offered triple-drug therapy, with postpartum withdrawal of antiretrovirals after cessation of breastfeeding for those ineligible for lifelong treatment.[5] The progression from Option B to Option B+ in 2015, where pregnant WLWH were offered lifetime ART regardless of CD4 count, was one of the key developments in the SA national HIV policy.[6]
An effective PMTCT programme ideally engages with WLWH as early as possible during pregnancy, because increased time on ART before delivery is associated with reduced risk of vertical transmission of HIV in utero, during labour and delivery and during breastfeeding.[8] WHO guidelines for high-quality antenatal care (ANC) in low- and middle-income countries specify that the first contact should occur within the first trimester and there should be a minimum of eight contacts. Prior to 2016, the WHO recommended minimum number of ANC contacts was four.[9]
We assessed the association of implementation of the Option B+ policy with engagement in antenatal and HIV care among a cohort of pregnant WLWH in KwaZulu-Natal (KZN) Province, SA. Here, we compare the timing of ANC and ART initiation during the periods before and after Option B+ implementation, to assess SA's progress toward achieving the UNAIDS 2025 goals related to pregnant women, specifically having 90% of pregnant WLWH initiated on ART before their current pregnancy.[10]
Methods
Setting and population
The Understanding Birth Outcomes for Mothers and Infants (UBOMI) cohort was initially developed by the SA National Department of Health, in partnership with the KZN Provincial Department of Health, to assess the risk of congenital malformations and adverse birth outcomes from exposure to ART during pregnancy.[11] The majority of data were collected at Prince Mshiyeni Memorial Hospital, a large public tertiary healthcare centre in Durban providing care for ~14 000 deliveries each year.
We analysed data from the UBOMI cohort of all pregnant women who presented at Prince Mshiyeni Memorial Hospital for delivery, and at three obstetric units within the hospital's catchment area for ANC from October 2013 to August 2017. The study period overlapped the transition from Option B to B+ implementation. Trained surveillance nurses interviewed pregnant women at their first ANC visit and obtained information on demographics, health and health-seeking behaviours during pregnancy, obstetric and neonatal history, HIV status and ART history, and maternal disease and substance exposures. These data were collected via a standardised digital form. Study enrolment was initially limited to weekdays owing to limited data collector availability in the first year of the study, and in subsequent years study enrolment was expanded to every day. Consent was waived because these were routinely collected during data gathering for the national pregnancy exposure and birth defects surveillance system. Maternal case record data at the time of delivery were used to confirm and expand on what was reported in the interview. Gestational age at birth was routinely documented by nursing staff based on the estimated date of delivery calculated during the first ANC visit using last menstrual period, and confirmed by ultrasound, when available.
Study variables
We defined the Option B era as the period from October 2013 to December 2014, while the Option B+ era was defined as the period from January 2015 to August 2017. We report on two co-primary outcomes related to engagement in HIV care: (i) timing and number of ANC visits during the pregnancy period; and (ii) timing of ART initiation (both self-reported ART use in interviews and observed initiation of treatment in maternal records).
Statistical analysis
The characteristics of women who engaged in HIV care and the timing and frequency of their participation in ANC before and after the implementation of Option B+ are described using frequencies and simple proportions, stratified by policy era. The association between policy era and timing of ANC presentation was assessed using log-binomial regression modelling. Estimated risk differences (RDs) and crude relative risks (RRs) with 95% confidence intervals (CIs) were reported. We also reported proportions initiating ART before or during pregnancy by policy era. Results are first reported with missing data excluded, which are then examined using a bestand worst-case sensitivity analysis.
Log-binomial regression models were used to estimate RRs and 95% CIs for the association between main exposure(s) and outcome. Prior to multivariable modelling, univariate analyses were conducted to assess the association between each covariate and the outcome. Variables p<0.05 in the univariate analysis were considered for inclusion in the multivariable model. This bivariate screening approach was used to reduce model complexity and focus on variables with a potential association with the outcome. Final models were assessed for collinearity and model fit.
Ethical considerations
Approval for this surveillance system was obtained from the SAMRC's ethics committee (ref. no. EC015-7/2013, approved 30 July 2013). As this provincial surveillance system has since evolved to become a national sentinel surveillance system, consent for routine data gathering was not required, but digital photography of infants with congenital malformations, as well as stillbirths, which is not routine, required explicit consent. Analyses of de-identified data was also approved by the Human Research Ethics Committee of the University of the Witwatersrand (Medical) (ref. no. M200237, approved 15 June 2020).
Results
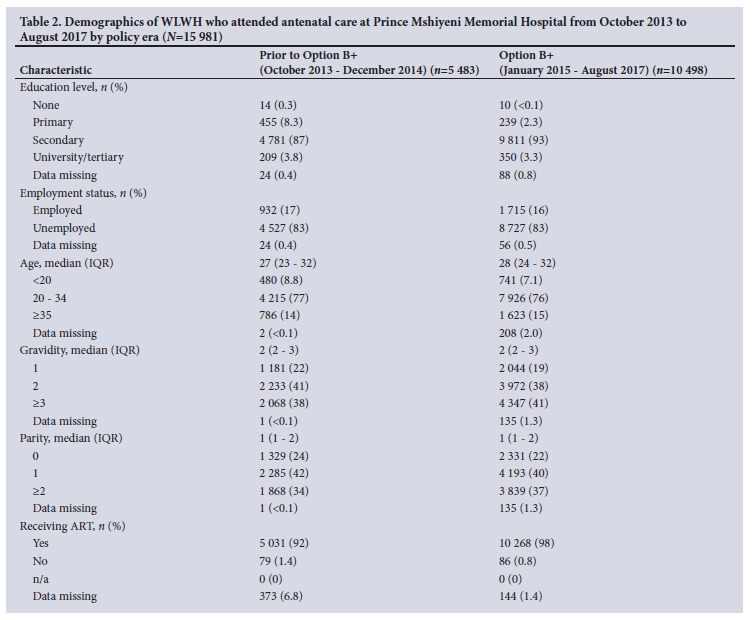
A total of 40 318 HIV-positive and HIV-negative pregnant women with a median (interquartile range) age of 24 (20 - 30) years attended ANC at Prince Mshiyeni Memorial Hospital from October 2013 to August 2017. Of these, 15 988 (39.7%) were WLWH, 17 of whom could not be assigned to a policy era because of missing data collection dates. Table 2 summarises the characteristics of this study population stratified by the PMTCT policy eras under study. There were no meaningful differences between groups in terms of education, employment status, age, gravidity and parity. However, a higher proportion of WLWH received ART during the Option B+ era (98%) than the period before Option B+ (92%).
Uptake and engagement in ANC across policy eras
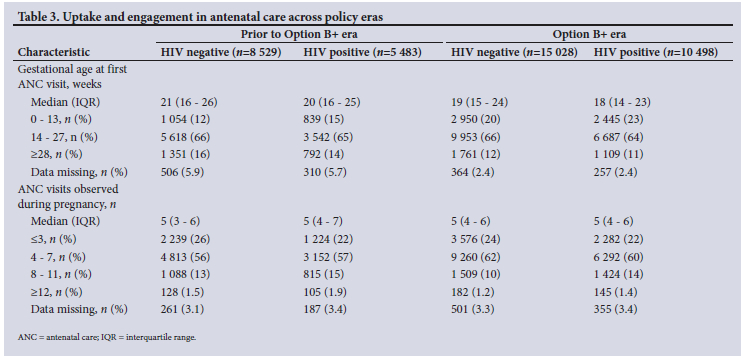
Table 3 reports uptake and engagement in ANC across policy eras. Median gestational age at first ANC visit decreased by 2 weeks during the Option B+ era; for HIV-negative women, the median gestational age at entry to ANC decreased from 21 to 19 weeks, while among HIV-positive pregnant women, gestational age at ANC entry decreased from 20 weeks under Option B to 18 weeks under Option B+. Over 60% of women during both eras, regardless of HIV status, presented for their first ANC visit in their second trimester. The median of five ANC visits during pregnancy was consistent across policy eras and HIV status.
Early presentation for ANC
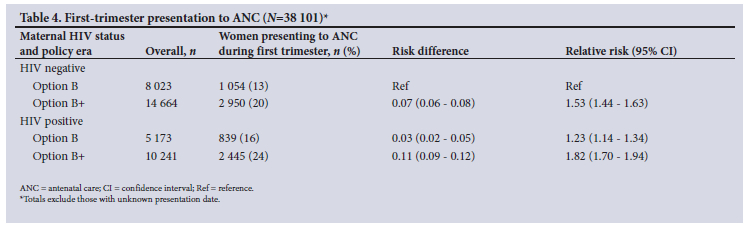
We also assessed the timing of ANC presentation, excluding the 17 women with unknown presentation dates (Table 4). During the Option B era, 13% of women living without HIV and 16% of WLWH presented for ANC in the first trimester, compared with 20% of women living without HIV and 24% of WLWH during the Option B+ era. Compared with women living without HIV in the Option B era, women living without HIV under Option B+ were 53% more likely to present for ANC in the first trimester (RR 1.53, 95% CI 1.44 - 1.63). In both eras, WLWH were more likely to present for ANC in the first trimester compared with women living without HIV (Option B: RR 1.23, 95% CI 1.14 - 1.34; Option B+: RR 1.82, 95% CI 1.70 - 1.94).
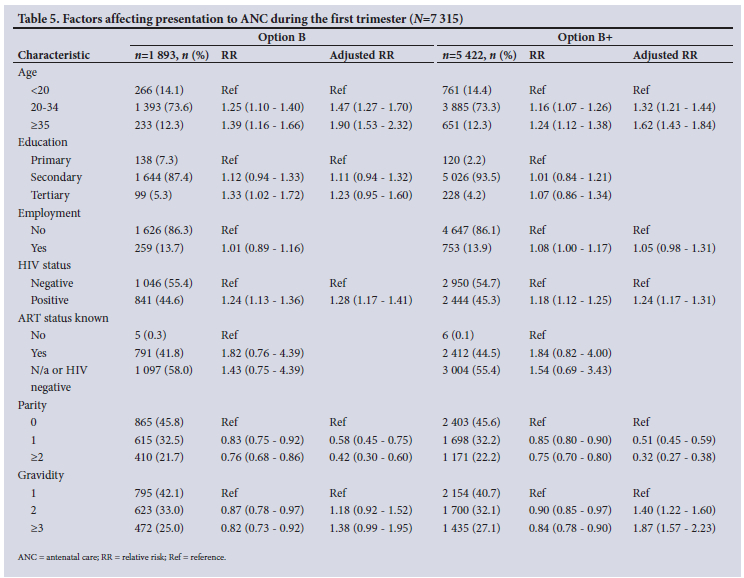
We further assessed the timing of ANC presentation by adjusting factors that may influence the timing of the first ANC visit (Table 5). In both eras older women >35 years were significantly more likely to initiate ANC in the first trimester (Option B: adjusted RR (aRR) 1.93, 95% CI 1.53 - 2.32; Option B+: aRR 1.62, 95% CI 1.43 - 1.84). HIV-positive women had significantly higher odds of early ANC (Option B: aRR 1.28, 95% CI 1.17 - 1.41; Option B+: aRR 1.24, 95% CI 1.17 - 1.31). Higher parity (>2 children) was strongly associated with reduced early ANC attendance (Option B: aRR 0.42, 95% CI 0.30 - 0.60; Option B+: aRR 0.32, 95% CI 0.27 - 0.38). During Option B+, higher gravidity (>3 pregnancies) was associated with early ANC attendance (Option B+: aRR 1.87, 95% CI 1.57 - 2.23).
Timing of ART initiation among pregnant women during the Option B and Option B+ eras
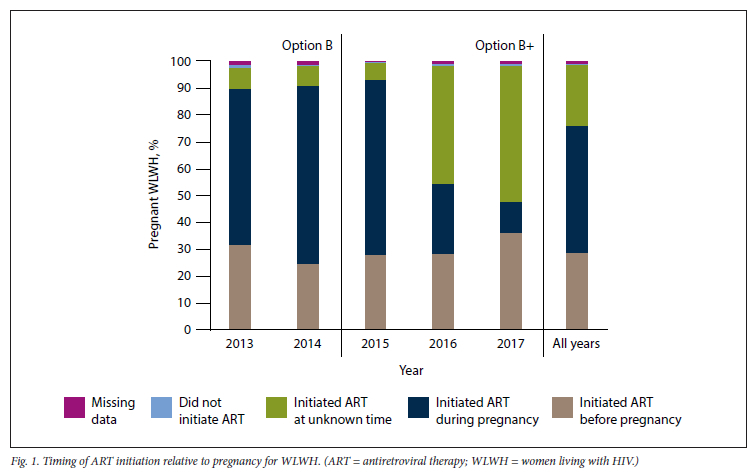
Across all study years, 4 603 (29%) WLWH initiated ART before pregnancy, 7 525 (47%) initiated ART during pregnancy, 3 579 (22%) initiated ART at an unknown date, 99 (1%) never started on ART and 175 (1%) were unknown. Fig. 1 summarises the timing of ART initiation in relation to pregnancy. The proportion initiating ART before or during pregnancy was high across both eras (>90% of those with known ART start dates), with 37% initiating ART prior to pregnancy among those with known ART start dates. Among women with known dates of initiation, 31% of WLWH initiated ART prior to pregnancy in the Option B era, compared with 53% of WLWH in the Option B+ era. In our sensitivity analysis, the best-case scenario, where we assumed that those who initiated ART at an unknown time had initiated ART before pregnancy, approximately half (51%) initiated ART before pregnancy. In the worst-case scenario, where we assumed that those who initiated ART at an unknown date had initiated it during pregnancy, more than two-thirds (69%) initiated ART during pregnancy across all study years.
Discussion
As SA seeks to meet its vertical HIV transmission goals through policies of expanded access to ART, understanding the uptake and timing of engagement in HIV care remains critical. Here, we have estimated engagement in ANC and uptake of HIV care before and after Option B+ implementation in SA between 2013 and 2017. We noted improvements in timing of entry to ANC. While overall, less than one-fifth (19%) presented for care during the recommended period in the first trimester, WLWH presented to ANC on average 2 weeks earlier in their pregnancy in the Option B+ era than the Option B era. In terms of frequency of care, almost 75% of women had >4 ANC visits, which was the minimum number of contacts during pregnancy recommended by the WHO prior to 2016.[9] We note, however, that these improvements in timing of entry to ANC also occurred among HIV-negative women, although overall, HIV-positive women tended to present at earlier gestational age. It is thus likely that factors other than implementation of the Option B+ policy have positively affected the timing of entry to ANC.
Despite this caution, our findings are in keeping with other national estimates from the SA Demographic Health Survey (DHS).[12] DHS results aggregated over 1998 - 2016 noted timing of ANC presentation to be 17% in the first trimester, 72% in the second trimester and 10% in the third trimester, similar to our findings. The DHS results also indicated that 79% of women nationally and 83% of women in KZN attended at least four ANC visits during pregnancy, similar to the 76% of women in our study.[13]
Our findings show that older age, HIV-positive status and higher gravidity are predictors of early ANC. Higher parity is a strong negative predictor, meaning that women with more previous births were less likely to present early. This may indicate that women with previous births delay care, possibly due to perceived familiarity with pregnancy, or competing responsibilities.
Most WLWH in this cohort started on ART prior to delivery. We found that the proportion of WLWH with known ART initiation dates who initiated ART prior to their pregnancy was higher in the Option B+ era than the Option B era. Specifically, in 2017, excluding those with missing data, 76% of WLWH in this cohort were on ART before their current pregnancy. In our results, 98% of WLWH across 2013 - 2017 received ART at some point before or during their pregnancy. This result is similar to what was found in the National Antenatal Sentinel HIV Survey,[14] where 87% of women in 2017 knew their HIV status, and 96% in 2019 were receiving ART at the time they were surveyed during pregnancy.[14] These estimates are still short of the Joint United Nations Programme on HIV/AIDS (UNAIDS) 2025 goal to have 90% of pregnant WLWH already initiated on ART before conception.[10] To ensure that >90% of pregnant WLWH are on ART at conception or prior to pregnancy, vertical transmission prevention programmes should use data to identify gaps in ART coverage among women of childbearing age and adjust programmes accordingly. While SA's PMTCT programme currently enforces universal HIV testing and has significantly expanded ART access among pregnant and postpartum women, healthcare providers can further strengthen these efforts by educating WLWH on the importance of ART before pregnancy.
Study limitations
Our findings should be considered in the context of some limitations in this analysis. First, the large proportion of missing ART initiation dates during the 2016 - 2017 period limits our interpretation of these results. In a sensitivity analysis, in the best-case scenario (assuming all those with unknown ART initiation dates initiated ART before pregnancy), about half of the women initiated ART before pregnancy. In the worst-case scenario (assuming all those with unknown ART initiation dates initiated during pregnancy), less than one-third were already on ART at entry to ANC across all study years.
Second, although a large dataset, the women observed were from one catchment area of Prince Mshiyeni Hospital in KZN Province, which may limit the generalisability of our findings beyond this population. Also, no viral load data were available in this analysis, and therefore we were unable to assess whether the impact of Option B+ implementation extended beyond engagement in HIV care to sustained viral load suppression.
Finally, for many women, breastfeeding continues for months after delivery, and so those on Option B may still have been breastfeeding (and therefore still on ART, according to the Option B guidelines) by the time B+ was implemented in 2015. In this way, the distinction between the policy eras may not have been very clear among breastfeeding women, and to the extent that this occurred, the benefits of the implementation of Option B+ in our estimates would be underestimated.
Despite these limitations, our findings from this large cohort offer valuable evidence of gains made in terms of meeting the UNAIDS 2025 targets. We found that SA has made progress in terms of improving women's engagement in ANC and HIV care. Despite increases in prior ART use at entry to ANC, pregnancy services remain an important portal for access to HIV care. For those women accessing care, most receive antenatal services at the appropriate frequency, although late presentation for ANC persists beyond the recommended gestational age. As a result of this, critical gaps to achieving targets for engagement in HIV care among pregnant women remain.
Conclusion
Engagement in antenatal and HIV care improved after Option B+ implementation. In the Option B+ era, SA has made significant progress toward the goal of eliminating mother-to-child transmission of HIV. There has been an increase in the proportion of pregnant WLWH initiating ART prior to pregnancy and presenting for ANC during the first trimester. The findings suggest improved timing and frequency of ANC visits during pregnancy, moving towards the UNAIDS 2025 targets.
Data availability. The data that support the findings of this study are owned by the KZN Provincial Department of Health, and access is governed by policies and procedures in response to requests made directly to the department. As such, the study teams do not have authority to release the data to the public or other data-sharing repositories. However, these data can be requested by the public through standardised request forms, which are then considered in an internal review procedure.
Declaration. None.
Acknowledgements. None.
Author contributions. CH and MM conceptualised the study and methodology. CH and NJ performed the analysis. CH and NJ wrote the original draft. CH, NJ, MM, MPF, KC, MD, MDH, PP and OM provided interpretation of results and critical review of the manuscript.
Funding. This study was funded by the US National Institutes of Health (NIH) Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institute for Allergy and Infectious Diseases under grant R01 HD103466, as well as the Fogarty International Center and National Institute of Mental Health of the NIH under award number D43 TW010543. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. The funding source had no role in the design of this study nor any role during its execution, analyses, interpretation of the data, or decision to submit results.
Conflicts of interest. None.
References
1. Kuhn L, Goga AE. Moving towards elimination: Findings from the South Africa prevention of mother to child transmission evaluation (SAPMTCTE). BMC Infect Dis 2019;19(1):782. https://doi.org/10.1186/s12879-019-4334-3 [ Links ]
2. South African Medical Research Council. Early mother-to-child transmission of HIV stats plunge. Cape Town: SAMRC, 2015. https://www.samrc.ac.za/media-release/early-mother-child-transmission-hiv-stats-plunge (accessed 6 April 2022). [ Links ]
3. Burton R, Giddy J, Stinson K. Prevention of mother-to-child transmission in South Africa: An ever-changing landscape. Obstet Med 2015;8(1):5-12. https://doi.org/10.1177/1753495x15570994 [ Links ]
4. National Department of Health, South Africa, South African National AIDS Council. Clinical guidelines: PMTCT (prevention of mother-to- child transmission). Pretoria: NDoH, 2010. https://sahivsoc.org/Files/NDOH_PMTCT_Apr_2008.pdf (accessed 17 January 2023). [ Links ]
5. National Department of Health, South Africa. The South African antiretroviral treatment guidelines. Pretoria: NDoH, 2013. https://sahivsoc.org/Files/2013_ART_Treatment_Guidelines_Final_25_March2013_corrected.pdf (accessed 25 July 2024). [ Links ]
6. National Department of Health, South Africa. National consolidated guidelines for the prevention of mother-to-child transmission of HIV (PMTCT) and the management of HIV in children, adolescents and adults. Pretoria: NDoH, 2015. https://knowledgehub.health.gov.za/system/files/elivdownloads/2019-07/National%2520consolidated%2520guidelines%25202015.pdf (accessed 2 August 2021) [ Links ]
7. World Health Organization. Programmatic update: Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Geneva: WHO, 2012. [ Links ]
8. Townsend CL, Cortina-Borja M, Peckham CS, De Ruiter A, Lyall H, Tookey PA. Low rates of mother-to-child transmission of HIV following effective pregnancy interventions in the United Kingdom and Ireland, 2000 - 2006. AIDS 2008;22(8):973-981. https://doi.org/10.1097/QAD.0b013e3282f9b67a [ Links ]
9. Jiwani SS, Amouzou A, Carvajal-Aguirre L, et al. Timing and number of antenatal care contacts in low and middle-income countries: Analysis in the countdown to 2030 priority countries. J Glob Health 2020;10(1):010502. https://doi.org/10.7189/jogh.10.010502 [ Links ]
10. Joint United Nations Programme on HIV/AIDS. Prevailing against pandemics by putting people at the centre. Geneva: UNAIDS, 2020. https://www.unaids.org/en/resources/documents/2020/prevailing-against-pandemics (accessed 10 July 2024) [ Links ]
11. Mehta UC, van Schalkwyk C, Naidoo P, et al. Birth outcomes following antiretroviral exposure during pregnancy: Initial results from a pregnancy exposure registry in South Africa. South Afr J HIV Med 2019;20(1):971. https://doi.org/10.4102/sajhivmed.v20i1.971 [ Links ]
12. Nxiweni PZ, Oladimeji KE, Nanjoh M, et al. Factors influencing the utilisation of antenatal services among women of childbearing age in South Africa. Women 2022;2(3):285-303. https://doi.org/10.3390.women2030027 [ Links ]
13. National Department of Health, South Africa, Statistics South Africa, South African Medical Research Council. South Africa Demographic Health Survey 2016 Key Findings. Pretoria: NDoH, 2018. https://dhsprogram.com/pubs/pdf/SR248/SR248.pdf (accessed 10 July 2024). [ Links ]
14. Woldesenbet S, Cheyip M, Lombard C, et al. Progress towards the UNAIDS 95-95-95 targets among pregnant women in South Africa: Results from the 2017 and 2019 National Antenatal HIV Sentinel Surveys. PLoS ONE 2022;17(7):e0271564. https://doi.org/10.1371/journal.pone.0271564 [ Links ]
 Correspondence:
Correspondence:
N Jinga
njinga@heroza.org
Received 10 June 2025
Accepted 5 August 2025

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}