










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkJournal of the South African Veterinary Association
On-line version ISSN 2224-9435Print version ISSN 1019-9128
J. S. Afr. Vet. Assoc. vol.95 n.1 Pretoria 2024
https://doi.org/10.36303/jsava.634
REVIEW
Immobilisation protocols for wild giraffe (Giraffa spp.) - a review
S FergusonI; RJ HarveyII; S FennessyI; J FennessyI
IGiraffe Conservation Foundation, Namibia
IIIndependent wildlife veterinarian, United Kingdom
ABSTRACT
BACKGROUND: Immobilisation of wild giraffe (Giraffa spp.) is challenging due to their unique anatomy and physiology. Field immobilisations are required for numerous conservation, tourism, and veterinary purposes. Wild giraffe immobilisation techniques have evolved considerably from physical to chemical with ultrapotent drugs
OBJECTIVE: To provide a detailed overview of historic and present protocols used for immobilising giraffe in the wild as a valuable resource tool for future research into best practices
METHODS: A systematic review was undertaken of the published literature on wild giraffe capture and immobilisation techniques with no restrictions on publication date
RESULTS: The review detailed the evolution of capture techniques used for wild giraffe. The trend has moved from purely physical capture in the 1950s to the use of high dose ultrapotent opioids or a combination of opioids and alpha-2 agonists and/or tranquilisers. With a better understanding of giraffe physiology and wild giraffe capture, mortality rates have decreased significantly from ~ 35% to < 1%
CONCLUSION: The advent of ultrapotent opioids has caused a paradigm shift in wildlife immobilisation, especially for wild giraffe. While the use of these drugs, as sole immobilisation agents or in combination with alpha-2 agonists or tranquilisers, has greatly reduced mortality rates associated with wild giraffe immobilisations, there is a startling lack of physiological data evaluating the impact of these drugs on giraffe during and after immobilisation. Future research should focus on measuring physiological variables to determine the impact and best practice of these protocols on wild giraffe immobilisation
Keywords: anaesthesia, Giraffa, giraffe, immobilisation, protocol, techniques, capture
Introduction
Immobilisation of wildlife has been an evolving artform for the past century. Historically, capture of wildlife was limited to the use of physical capture by a variety of means (trapping, from horseback, vehicle, or more recently, helicopter), some of which are still used for both individual and mass capture operations (van Citters et al. 1968; Hirst et al. 1965; Langman 1973; Laubscher et al. 2015). Since the 1960s, chemical immobilisation of wildlife has become a feasible alternative due to the availability of novel agents, coinciding with the development of remote delivery devices e.g. the CapChur dart, an explosively driven dart fired from a shotgun modified to use .22 blank rounds as the propellent (van Niekerk et al. 1963; Langman 1973). Chemical immobilisation opened new avenues for the immobilisation of individual animals. However, it was the advent of the ultrapotent opioids, immobilising agents which induce a neuroleptanalgesia-like state of sedation and analgesia, that further advanced chemical capture of wildlife, particularly for megaherbivores (Kreeger et al. 2023). Highly concentrated etorphine and thiafentanil allowed for smaller volumes that could easily fit into darts, could be reversed (antagonised) and used as the sole immobilising agent or in combination with the other classes of immobilisation drugs (Alford et al. 1965; Haigh 1990). Over the past 60 years chemical immobilisation of wildlife has advanced rapidly, largely through trial and error, although for wildlife veterinarians it remains an ever-evolving field as novel drug combinations, varying doses, and better objective data are collected. While our understanding of agents and capture protocols has improved, many unknowns remain and development and use of protocols often rely on subjective data or anecdotal advice.
Giraffe (Giraffa spp.) are regarded a difficult species to immobilise due to their unique anatomy and physiology (Bush et al. 2002). Their blood pressure (260/160 mm Hg, van Citters et al. 1963), long trachea (large dead space and propensity for ventilation/ perfusion mismatch), rumen (prone to aspiration), mass (7001 400 kg), and awkward body shape all contribute to multiple risks for giraffe during immobilisations including cardiorespiratory compromise, capture myopathy, hyperthermia, trauma, and aspiration secondary to regurgitation of rumen contents (Bush et al. 2022; Kock & Burroughs 2021). It remains unclear why giraffe appear to react differently to immobilisation drugs, especially the ultrapotent opioids, than other mammals. While most herbivores can be dosed to become affected and recumbent usually within approximately 10 minutes, equivalent opioid doses in giraffe cause them to fall into a slow and steady gallop instead, and unless tripped, giraffe will continue to run - ultimately until their death (Langman 1973; Kock & Burroughs 2021). Before the use of ultrapotent opioids for giraffe immobilisation, other immobilisation drugs were often considered too dangerous and not advantageous over physical capture means (Hirst 1966). Today, it is standard practice for wild giraffe immobilisations to give a high dose of opioid(s) to bring them down quickly, necessitating immediate administration of the antagonist to prevent death (Kock & Burroughs 2021; Deacon et al. 2022; Barnes et al. 2023; Kreeger et al. 2023). The threatened conservation status of some giraffe species coupled with increasing interventions e.g. fitting of GPS trackers, translocations, veterinary interventions such as treating wounds caused by illegal hunting (poaching), have revealed the startling gaps in scientific knowledge around giraffe immobilisations.
This review covers the methodologies historically and currently employed to immobilise wild giraffe. While capture protocols have evolved and resulted in decreasing mortality rates from ~ 35% (Kreeger et al. 2023) to now < 1% (Bush et al. 2002; Deacon et al. 2022; Barnes et al. 2023), there is a lack of scientific data to assess the overall physiological and welfare impact and best-practice protocols for wild giraffe immobilisations. By understanding the evolution of wild giraffe immobilisation protocols, we aim to establish a foundation for evaluating the impact of current protocols as well as exploring potential future alternative drug combinations.
Methods
A systematic review of wild giraffe immobilisation protocols was performed. Published literature on giraffe capture and immobilisation was searched using Google, Google Scholar, PubMed, ResearchGate, and Scopus search engines with the following key words in combination with "wild giraffe" immobilisation, anaesthesia, capture, manual capture, chemical capture. No restrictions on publication date were placed and publications that were unrelated but included immobilisation mentioned under methodology, e.g. telemetry device studies, were included. Only protocols used on wild giraffe were included for this review as captive and zoo giraffe immobilisation protocols differ drastically in approach and methodology (Harthoorn 1965).
Results
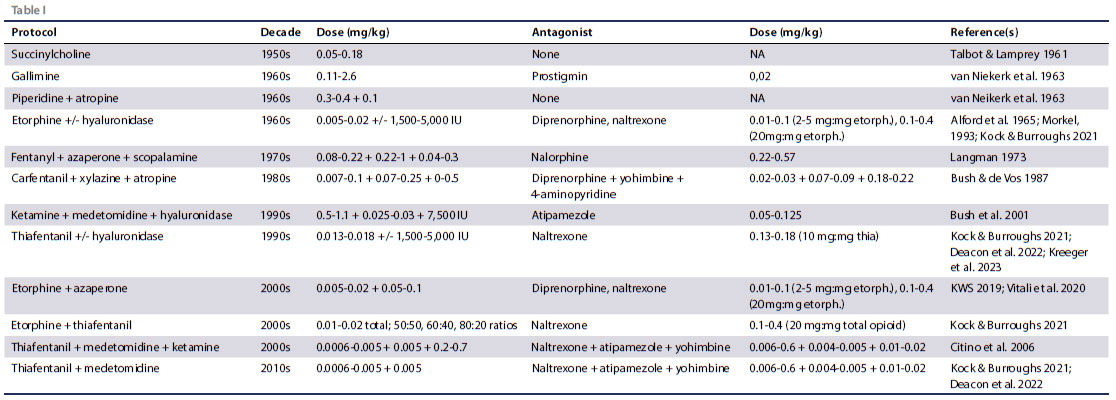
A total of 62 references were found to describe wild giraffe immobilisation techniques. References were narrowed to those including the most comprehensive information on capture/immobilisation techniques or the first documentation of a protocol that was duplicated in multiple papers. In total, 13 protocols for wild giraffe capture and immobilisation (including manual capture techniques) were found in the literature. Chemical protocols (12 combinations in total) are summarised in Table I. No study measured actual body mass in wild giraffe, therefore all doses were estimated based on estimated average body mass.
Manual capture of giraffe is achieved through chasing and roping them either from horseback or vehicle (van Citters et al. 1968; Hirst et al. 1965; Langman 1973). Mass capture of giraffe can be done by herding individuals or groups of animals, usually with a helicopter, into a large pre-established funnel and ultimately channelled into a boma or directly onto a transport crate/truck (Laubscher et al. 2015). The latter is the current method of choice for mass capture of giraffe.
Chemical immobilisation of wild giraffe began with succinylcholine and gallamine (van Niekerk et al. 1963; Langman 1973; Savarie 1976). Succinylcholine at 0.05- 0.18 mg/kg was noted to be effective for immobilisation (Talbot & Lamprey 1961; Langman 1973). Gallamine was used at doses of 0.11-2.6 mg/kg and had an antagonist, prostigmin, at doses of 0.02 mg/kg (van Niekerk et al. 1963; Langman 1973).
Piperidine (better known as phencyclidine or PCP) was used in combination with atropine in wild giraffe, with an optimum combination of 0.3-0.4 mg/kg piperidine and 0.1 mg/kg atropine (van Niekerk et al. 1963). This protocol, like succinylcholine, does not have an antagonist reversal drug. Ketamine in combination with medetomidine and hyaluronidase (hyalase) was another combination used, and in this study doses were determined by estimating giraffe shoulder height (SH) rather than estimated mass; however, for consistency doses were converted to mg/kg for this review (Bush et al. 2001). Immobilisations were achieved with 0.5-1.1 mg/kg ketamine (400-900 mg total dose; 2.13.8 mg/cm SH), 0.025-0.03 mg/kg medetomidine (20-30 mg total dose; 0.12-0.17 mg/cm SH), and 7 500 IU hyaluronidase (Bush et al. 2001). This protocol is partially reversable with atipamezole administered 30 minutes after recumbency at a dose of 0.05-0.125 mg/kg (40-100 mg total dose; 0.34 mg/cm SH) (Bush et al. 2001).
Carfentanil, xylazine, and atropine combined have been trialled for adult wild giraffe at doses of 0.007-0.01 mg/kg carfentanil (7-8 mg total dose), 0.07-0.25 mg/kg xylazine (60-200 mg total dose), and 0-0.5 mg/kg atropine (0-400 mg total dose) by intramuscular (IM) injection (Bush & de Vos 1987). For this protocol, carfentanil was antagonised using 0.02-0.03 mg/kg diprenorphine (M5050) with 2/3 intravenous (IV) and 1/3 IM (1416 mg IM and 7-8 mg IV total dose respectively), and xylazine antagonised with 0.07-0.09 mg/kg yohimbine (75 mg total dose) and 0.18-0.22 mg/kg 4-aminopyridine (180 mg total dose), both given IV. Fentanyl has been used in combination with azaperone and hyoscine (scopolamine), at 0.08-0.22 mg/kg fentanyl (25120 mg total dose), 0.22-1 mg/kg azaperone (120-400 mg total dose), and 0.04-0.3 mg/kg scopolamine (35-50 mg total dose) (Langman 1973). This protocol was reversed with 0.22-0.57 mg/ kg nalorphine IV (65-250 mg total dose) (Langman 1973).
Etorphine (M99) has been used commonly as a sole agent for wild giraffe immobilisation. Estimated doses have ranged from 0.005-0.02 mg/kg (4-24 mg total dose), and has been used with or without hyaluronidase (1 500-5 000 IU) (Alford et al. 1965; Kock & Burroughs 2021; Kreeger et al. 2023). Etorphine at the above dose range has also been used commonly in combination with 0.05-0.1 mg/kg azaperone (20-60 mg total dose) and 1 500-5 000 IU hyaluronidase (KWS 2019; Vitali et al. 2020). Alternatively, etorphine has been used more recently in combination with thiafentanil (Thianil) in 50:50, 40:60, and 20:80 etorphine:thiafentanil combinations estimated 0.01-0.02 mg/kg total opioid (i.e. etorphine plus thiafentanil equalling 7-24 mg total opioid dose), again with or without hyaluronidase (1 5005 000 IU) (Kock & Burroughs 2021). Etorphine-based protocols can be partially reversed with diprenorphine (2-5 mg:mg etorphine) (KWS 2019; Kock & Burroughs 2021; Deacon et al. 2022) or fully reversed with naltrexone (20 mg:mg etorphine) (O'Dell et al. 2017; Kock & Burroughs 2021).
Thiafentanil has also been used as a sole agent for wild giraffe immobilisation with doses ranging from an estimated 0.0130.018 mg/kg (7-18 mg total dose), with or without hyaluronidase added (1 500-5 000 IU) (Kock & Burroughs 2021; Deacon et al. 2022; Kreeger et al. 2023). This protocol is reversed with naltrexone (10 mg:mg thiafentanil) (Wildlife Pharmaceuticals 2010; Kock & Burroughs 2021; Kreeger et al. 2023). Thiafentanil has also been used in combination with medetomidine with doses ranging from 0.0006-0.005 mg/kg thiafentanil (0.5-5 mg total dose) and 0.005 mg/kg medetomidine (2-5 mg total dose) (Kock & Burroughs 2021; Deacon et al. 2022; D. Pretorius pers. comm.). Ketamine has also been trialled in combination with thiafentanil plus medetomidine protocols at doses of 0.2-0 .7 mg/kg (Citino et al. 2006), with the reversal for the effects of thiafentanil and medetomidine achieved with 0.0060.06 mg/kg naltrexone (10 mg:mg thiafentanil), 0.0040.005 mg/kg atipamezole (1 mg:mg medetomidine), and 0.01-0.02 mg/kg yohimbine (6 mg:mg medetomidine) (Kock & Burroughs 2021; D. Pretorius pers. comm.).
Discussion
Wildlife immobilisation, particularly for wild giraffe, has advanced greatly since the 1930s. The primary goal of any wild giraffe immobilisation is to maintain animal and human safety, and utilise a protocol that ideally uses drugs with a high safety margin, are reversable, concentrated enough to fit into one dart, produce rapid induction, have few to no physiological side effects, and are affordable (van Niekerk et al. 1963).
Prior to the 1960s, manual capture of giraffe was the only option and while "relatively" effective for catching juveniles to small subadults/adults, it was extremely dangerous both for the capturers and giraffe (Langman 1973). To reduce injuries and mortalities, Jan Oleofse is credited with developing the method of mass capture, herding groups of animals into a large funnel then ultimately into a boma or directly onto a transport crate or truck, which revolutionised wildlife capture and remains a safe and effective way for wild giraffe capture to this day (Laubscher et al. 2015). However, purely manual techniques for individual capture are largely ineffective and chemical immobilisation protocols achieve superior results.
While chemical immobilisation is preferred for individual wild giraffe, there is still an element of manual capture by any capture team (Kock & Burroughs 2021; Kreeger et al. 2023). For human and giraffe safety, it is invaluable for an experienced capture team to be involved, as it is often required to induce lateral recumbency through tripping the giraffe with ropes once it shows adequate signs of drug effect (unless it trips on its own) (Kock & Burroughs 2021; Kreeger et al. 2023).
Chemical immobilisation of wild giraffe began with trials using the nondepolarising neuromuscular blocking drugs succinylcholine or gallamine that act by paralysing the skeletal muscles (van Niekerk et al. 1963; Langman 1973; Savarie 1976). This class of drugs has no analgesic or sedative effects nor do they induce any level of unconsciousness (Savarie 1976; Kreeger et al. 2023). Succinylcholine had a rapid onset of action in wild giraffe, and depending on the dose administered, animals were recumbent for 20-60 minutes (van Niekerk et al. 1963). Succinylcholine showed a high risk of inducing respiratory paralysis, aspiration, and death (Talbot & Lamprey 1961; Langman 1973). These undesirable side effects were reportedly less when a sedative was administered prior to administering succinylcholine, however, the exact sedation drugs were not mentioned nor were doses given (Langman 1973). Gallamine was initially more widely used for wild giraffe immobilisation and reversible with the antagonist prostigmin (van Niekerk et al. 1963; Langman 1973). However, hypotension and asphyxia were observed as risks (van Niekerk et al. 1963; Langman 1973). Additionally, if they became recumbent in eight minutes or less, the veterinarian had to "make haste" and administer one fourth of the antagonist intravenously to prevent respiratory arrest and death (Harthoorn 1965). Through improved medicine, we now know that neuromuscular blocking drugs have a narrow margin of safety and are inferior to modern immobilising agents and should not be used in wild giraffe capture and immobilisation (Kreeger et al. 2023).
In the early 1960s a suite of drugs were synthesised and trialled for wildlife immobilisation. These included dissociative anaesthetics (piperidine, ketamine, tiletamine), tranquilisers (acepromazine, azaperone, perphenazine), benzodiazepines (diazepam, midazolam, zolazepam), alpha-two agonists (xylazine, medetomidine), and opioid derivatives (etorphine, fentanyl, carfentanil, thiafentanil) (van Niekerk et al. 1963; Alford et al. 1965; Savarie 1976). For wild giraffe, the main drugs used for immobilisation over the years included piperidine, ketamine, azaperone, xylazine, medetomidine, carfentanil, fentanyl, etorphine, and thiafentanil, roughly in chronological order.
The dissociative drugs (piperidine, ketamine) act on N-methyl-D-aspartate (NMDA) receptors in the brain and depending on the amount used can provide pain relief, sedation, and/or anaesthesia (Kreeger et al. 2023). Piperidine, when used in combination with atropine in wild giraffe, resulted in an induction time of 920 minutes (van Niekerk et al. 1963). However, at the reported doses, immobilisation lasted approximately 1.5 hours, which is highly undesirable due to the amount of time required to medically manage them, which is usually limited in field settings, and increased likelihood of secondary complications in the field (van Niekerk et al. 1963; Bush et al. 2002; Kock & Burroughs 2021; Kreeger et al. 2023). Protocols using piperidine were enhanced when combined with a tranquiliser such as perphenazine or triflupromazine (van Niekerk et al. 1963). Ketamine combined with medetomidine also yielded acceptable immobilisations, with induction times ranging from 6-27 minutes, with the variations in induction times attributed to more excitable or taller animals resulting in a lower dose compared to smaller ones (dosing was based on giraffe SH rather than weight estimation) (Bush et al. 2001). Physiological data revealed that all wild giraffe were initially mildly acidotic, which resolved without intervention and were hypoxaemic throughout the immobilisation (Bush et al. 2001). The dissociative class of drugs are considered relatively safe drugs, as they are considered cardio- and cerebro-protective, and have a high therapeutic index. However, when used as sole agents they can result in convulsions and thus are generally combined with other agents (Kreeger et al. 2023). This class of drugs are also not reversible, which is largely undesirable for wild giraffe immobilisations due to the inability to effectively manage anaesthetised animals in the field for prolonged periods of time (Kock & Burroughs 2021; Kreeger et al 2023). The ketamine and medetomidine combination protocols observed induction times longer than what was normally accepted (< 10 minutes), and the wild giraffe were hypoxaemic throughout the procedure (Bush et al. 2001). All doses were based on SH and as such less reliable for larger/taller animals.
The use of potent opioids came with the benefit of specific antagonists and provided the option for partial or fully reversible field protocols (Kock & Burroughs 2021; Kreeger et al. 2023). Etorphine, fentanyl, and carfentanil have all been trialled in wild giraffe immobilisations and while effective, initially resulted in > 10% mortality rate (Pienaar et al. 1966; Langman 1973). Mortality was mainly due to prolonged inductions resulting in hyperthermia and collapse from hypoxaemia, whilst the risk of regurgitation and fatal aspiration also contributed to observed mortalities (Langman 1973; Teferra 1992). Additionally, longer induction times also increased the likelihood of inducing potentially fatal capture myopathy (Kock & Burroughs 2021; Kreeger et al. 2023). Out of the available drugs, etorphine rapidly became preferred for immobilisation of wild giraffe (Harthoorn 1965). In the 1960s, an alternative etorphine formulation to M99 existed which was the acetylated form of etorphine, known as M183 (Pienaar et al. 1966). According to Pienaar et al. (1966), M183 was reportedly safer than M99 for wildlife immobilisations and the preferred immobilisation drug for wild giraffe. However, M183 was only reported to be used during the 1960s and one of the larger trials on wild giraffe in South Africa resulted in a 27% mortality rate (Hirst 1966).
Early doses of etorphine were categorised as "low-dose" compared to modern protocols and dose ranges (< 0.01 mg/ kg; Kock & Burroughs 2021). As more wild giraffe captures were performed with etorphine, veterinarians advised on higher doses to reduce induction times, lessen the chances of "overexertion" and decrease mortality rates (Savarie 1976; Morkel 1993). While higher doses did reduce induction times, to reduce mortality from hypoxaemia and respiratory arrest, veterinarians needed to quickly administer an IV reversal (Morkel 1993; Kock & Burroughs 2021; Kreeger et al. 2023). Current wild giraffe field immobilisation protocols employ a high-dose protocol, recommending 0.012-0.020 mg/kg of etorphine combined with hyaluronidase followed by immediate reversal with naltrexone or diprenorphine IV once the animal is in lateral recumbency, and manually restrained (Kock & Burroughs 2021; Barnes et al. 2023). Higher doses of etorphine also allowed for quicker intervention by the ground capture team using ropes, further reducing the induction time (Kock & Burroughs 2021). The high dose etorphine protocol is believed to have reduced mortality rates to < 1% and proved effective in wild giraffe of all ages (including juveniles) as well as individuals with severe wounds or in poor body condition (Barnes et al. 2023).
Thiafentanil was first trialled in wildlife in the early 1990s, and rapidly started to replace etorphine as the preferred ultrapotent opioid in immobilisations (Lance 2012). In wild giraffe, thiafentanil has been used at doses comparable to the high-dose protocols involving etorphine (Kock & Burroughs 2021; Deacon et al. 2022; Kreeger et al. 2023). However, it is thought that giraffe may be more sensitive to thiafentanil and could require lower doses in thiafentanil-only protocols compared to etorphine-only protocols (P. Morkel per. comm.). The use of high-dose thiafentanil protocols increased the likeliness of wild giraffe tripping without the intervention of a ground capture team, potentially making this protocol superior to etorphine in circumstances where a less experienced capture team is available, or in difficult terrain that could inhibit their approach (Kock & Burroughs 2021). Mortality rates of < 1% are claimed when thiafentanil only protocols are used (Deacon et al. 2022), whilst good success of thiafentanil in combination with etorphine at various ratios has also been observed (Kock & Burroughs 2021; Deacon et al. 2022).
High-dose ultrapotent opioid protocols not only appear more effective for wild giraffe capture and immobilisation, they appear to have reduced mortality rates to a more acceptable level. However, there is concern over the need to use what is considered a lethal overdose of opioid to induce lateral recumbency (M. Jago per. comm.). Additionally, the associated cost of the drugs at high doses, especially thiafentanil, is often inhibitive (U. Tubessing per. comm.). As such, to reduce the amount of ultrapotent opioid used, veterinarians have trialled the combination of thiafentanil with an alpha-two agonist, predominately medetomidine, both with and without the addition of ketamine (Citino et al. 2006; Kock & Burroughs 2021). These protocols use a dramatically reduced dose of thiafentanil which negates the need for immediate opioid reversal (Citino et al. 2006; Kock & Burroughs 2021). It is reported that these protocols, compared to high-dose opioid protocols, induce more variable induction times and as the animals remain reactive to visual stimuli until fully affected, the use of a ground team needs to delayed until the giraffe is unresponsive to avoid inducing the giraffe to run and being kicked during roping (D. Pretorius pers. comm.). There are also reports of re-sedation in wild (and captive) giraffe, resulting in the need to administer additional atipamezole, which is largely impossible to monitor and/or administer in the field (Citino et al. 2006). This could indicate that the doses for alpha-2 antagonists used in giraffe immobilisations are too low, and warrants evaluation of administering higher doses at the time of reversal or studying the pharmacokinetics of these drugs in giraffe.
Another possible drug combination that is normally only advised for use in captive settings, is the combination of butorphanol, azaperone and medetomidine (BAM) (Kock & Burroughs 2021). The BAM combination has only been reported once for wild giraffe (Deacon et al. 2022). Doses for each drug were not listed, however, the induction time was noted as 50 minutes before the animal became recumbent (Deacon et al. 2022). Kock & Burroughs (2021) advised doses of BAM at 0.3mg/kg, 0.12 mg/ kg and 0.12 mg/kg respectively for adult giraffe in captivity only, as often supplemental doses are required, especially if immobilising a larger animal. This protocol is reversable with naltrexone (1 mg:mg butorphanol) and atipamezole (5 mg:mg medetomidine) (Kock & Burroughs 2021). However, due to the very long induction time, and the large volume that would be necessary for immobilising adult giraffe, the use of BAM as a field protocol is not practical and considered dangerous for wild giraffe immobilisation procedures. Should some of the component drugs become available in a more concentrated form, this protocol could be reassessed. However, further research would be necessary in a controlled setting to fully understand the impacts of the protocol on giraffe and the potential risks e.g. likelihood of hyperthermia, capture myopathy, regurgitation and aspiration, etc.
For each of the drug combinations and protocols mentioned in this review there is a distinct lack of physiological data detailing the effects and impacts of the immobilisations and immobilising drugs on giraffe physiological and metabolic processes, both during and after immobilisation and reversal. Ultrapotent opioids are known to cause respiratory and metabolic compromise, hyperthermia, hypertension, and altered gastrointestinal motility (Kock & Burroughs 2021; Kreeger et al. 2023). Alpha-2 agonists cause variable blood pressure changes, cardiovascular and respiratory compromise and decreased gastrointestinal motility (Kock & Burroughs 2021; Kreeger et al. 2023). In addition, alpha-2 antagonists have been associated with profound acute hypotension and insulin secretion leading to derangements of blood glucose and possibly even causing hypoglycaemia (Guillot et al. 1998; Grimsrud et al. 2012; Box et al. 2021). While mortality rates are used to interpret overall 'safety' of an immobilisation protocol, they are likely underreported and only reported for when a giraffe does not recover from the immobilisation event rather than also including post-immobilisation, translocation, and release deaths which could still be caused by or attributed to the physiological disturbances related to immobilising and antagonistic drugs, insufficient doses of antagonistic drugs, or the stress of capture. Capture myopathy - a poorly understood condition that can result in death hours, days, to weeks after the initial immobilisation and capture event - is reported to cause the largest number of mortalities during any capture, immobilisation, or translocation (Breed et al. 2019). To better understand true mortality rates, it is imperative that studies are performed to evaluate physiological variables during immobilisation and capture events, as well as monitor individuals for at least a month following an immobilisation or capture event. Such studies would help to better evaluate animal welfare and safety, guide best practices for giraffe immobilisation techniques, and provide a sound basis for comparison when evaluating new protocols.
Conclusion
Wild giraffe capture and immobilisation has progressed from their initial roping from horseback to current use of ultrapotent opioids and sophisticated darting systems. Mortality rates once ~ 35% have been possibly reduced to < 1% due to the use of highdose ultrapotent opioids resulting in reduced induction times with quick administration of reversal agents, more experience leading to better capture techniques, and more training opportunities (Hirst 1966; Deacon et al. 2022; Barnes et al. 2023; Kreeger et al. 2023). Newer protocols include reduced doses of ultrapotent opioids in combination with alpha-2 agonists to both reduce the risk of using lethal amounts of opioids and to save costs, but their safety needs to be properly assessed. It is important to note that while discussed here, protocols involving the use of succinylcholine, gallamine, and piperidine are no longer considered acceptable as ethical and safe for wild giraffe immobilisation. Current recommended protocols use highdose opioids or the low-dose opioid-alpha-2 combinations. Importantly, this review revealed a startling lack of scientific data to justify the use of one protocol over another. It therefore should be a priority to scientifically evaluate all currently used protocols in a systematic and objective way to guide best practice for wild giraffe immobilisation techniques, as well as to provide a basis of comparison for new protocol evaluations.
Conflict of interest
The authors declare no conflict of interest.
Funding source
Funding for this review manuscript was provided by Giraffe Conservation Foundation.
ORCID
S Ferguson https://orcid.org/0000-0002-8086-6706
RJ Harvey https://orcid.org/0009-0007-3943-9836
S Fennessey https://orcid.org/0000-0002-3365-1075
J Fennessey https://orcid.org/0000-0001-5871-8267
References
Alford, B.T., Burkhart, R.L., Johnson, W.P., 1965, Etorphine and diprenorphine as immobilizing and reversing agents in captive and free-ranging mammals, Journal of American Veterinary Medical Association 164(7), 702-705. [ Links ]
Barnes, S., Lubega, J., Mama, K., et al., 2023, Use of etorphine hydrochloride for immobilisation of Nubian giraffe for wire snare removal: a retrospective study, Journal of South African Veterinary Association 94(1), 83-86. https://doi.org/10.36303/JSAVA.575. [ Links ]
Box, J.R., Karikoski, N.P., Tanskanen, H.E., et al., 2021, The effects of an alpha-2-adrenoceptor agonist, antagonist, and their combination on the blood insulin, glucose, and glucagon concentrations in insulin sensitive and dysregulated horses, The Veterinary Journal 269, 105610. https://doi.org/10.1016/j.tvjl.2021.105610. [ Links ]
Breed, D., Meyer, L.C., Steyl, J.C.A., et al., 2019, Conserving wildlife in a changing world: Understanding capture myopathy - a malignant outcome of stress during capture and translocation, Conservation Physiology 7, 1093. https://doi.org/10.1093/conphys/coz027. [ Links ]
Bush, M., de Vos, V., 1987, Observations on field immobilization of free-ranging giraffe (Giraffa camelopardalis) using carfentanil and xylazine, Journal of Zoo and Animal Medicine 18(4), 135-140. https://doi.org/10.2307/20094823. [ Links ]
Bush, M., Grobler, D.G., Raath, J.P., et al., 2001, Use of medetomidine and ketamine for immobilization of free-ranging giraffes, Journal of the American Veterinary Medicine Association 218(2), 245-249. https://doi.org/10.2460/javma.2001.218.245. [ Links ]
Bush, M., Grobler, D.G., Raath, J.P., 2002, The art and science of giraffe (Giraffa camelopardalis) immobilization/anesthesia, In: Heard D., editor. Zoological Restraint and Anesthesia. International Veterinary Information Service; Ithica, NY, USA: 2002. [ Links ]
Citino, S.B., Bush, M., Lance, W., et al., 2006, Use of thiafentanil (A3080), medetomidine, and ketamine for anethesia of captive and free-ranging giraffa (Giraffa camelopardalis), Proceedings from the American Association of Zoo Veterinarians Conference 2006, 3. [ Links ]
Deacon, F., Daffue, W., Nel, P., et al., 2022, Effective field immobilisation and capture of giraffe (Giraffa camelopardalis), Animals 12(10):1290. https://doi.org/10.3390/ani12101290 [ Links ]
Grimsrud, K.N., Mama, K.R., Steffey, E.P., et al., 2012, Pharmacokinetics and pharmacodynamics of intravenous medetomidine in the horse, Veterinary Anaesthesia and Analgesia 39(1), 38-48. https://doi.org/10.1111/j.1467-2995.2011.00669.x. [ Links ]
Guillot, E., Coste, A., Eon, M.T., et al., 1998, Mechanisms of the hypoglycemic effects of a2-adrenoceptor antagonists SL8.0418 and deriglidole, Life Sciences 62(9), 839-852. https://doi.org/10.1016/S0024-3205(97)01186-7. [ Links ]
Haigh, J.C., 1990, Opioids in zoological medicine, Journal of Zoo and Wildlife Medicine 21(4), 391-413. [ Links ]
Harthoorn, A.M., 1965, Application of pharmacological and physiological principles in restraint of wild animals, Wildlife Monographs 14, 75. [ Links ]
Hirst, S.M., Kettlitz, W.K., Visagie, G.P., 1965, The use of Ro 5-2807 (Roche) as a tranquiliser in wild ungulates, Zoological Africana 1(1), 231-238. https://doi.org/10.1080/00445096.1965.11447315. [ Links ]
Hirst, S.M., 1966, Immobilisation of the Transvaal giraffe (Giraffa camelopardalis giraffa) using an oripavine derivative, Journal of South African Veterinary Medical Association 37(1), 85-89. [ Links ]
Kock, M., Burroughs, R., 2021, Chemical and physical restraint of African wild animals, Third Ed. Greyton, South Africa, 475 pp. [ Links ]
Kreeger, T.J., Arnemo, J.M., Caulkett, N.A., et al., 2023, Handbook of wildlife chemical immobilisation, Sixth Ed., Bovey, Minnesota, USA, 497 pp. [ Links ]
Kenya Wildlife Service (KWS), 2019, Immobilization and translocation protocol for the giraffe, Kenya Wildlife Service Veterinary Services Department, Nairobi, Kenya 9 pp. [ Links ]
Lance, W., 2012, Thiafentanil (A3080): will it replace etorphine and carfentanil? What species does it work or not work in?, Proceedings from the American Association of Zoo Veterinarians Conference 2012, 2. [ Links ]
Langman, V.A., 1973, The immobilization and capture of giraffe, South African Journal of Science 69, 200-203. [ Links ]
Laubscher, L.L., Pitts, N.E., Raath, J.P., et al., 2015, Non-chemical techniques used for the capture and relocation of wildlife in South Africa, African Journal of Wildlife Research 45(3), 275-286. https://doi.org/10.3957/056.045.0275. [ Links ]
Morkel, P., 1993, Chemical capture of the giraffe Giraffa camelopardalis. The Capture and Care Manual, 2nd ed., Mckenzie, AA, Ed. [ Links ]
O'Dell, J.H., Kock, M.D., Thompson, P.N., et al., 2017, Minimum effective naltrexone dose to antagonise etorphine immobilisation and prevent the complications of renarcotisation in domestic goats, Veterinary Record 181(18), 481. https://doi.org/10.1136/vr.104435. [ Links ]
Pienaar, U. de V., van Niekerk, J.W., Young, E., et al., 1966, Neuroleptic narcosis of large wild herbivores in South African national parks with the new potent morphine analogues M-99 and M-183, Journal of South African Veterinary Medical Association 37(3), 277-291. [ Links ]
Savarie, P.J., 1976, Pharmacological review of chemicals used for the capture of animals, U.S. Fish and Wildlife Service, Denver, Colorado, USA 178-184. [ Links ]
Talbot, L.M., Lamprey, H.F., 1961, Immobilization of free-ranging East African ungulates with succinylcholine chloride, Journal of Wildlife Management 25(3), 303-310. https://doi.org/10.2307/3797858. [ Links ]
Teferra, Z., 1992, Chemical immobilisation of wildlife, Ethiopian Wildlife Conservation Organisation, Addis Ababa, Ethiopia 15 pp. [ Links ]
Van Citters, R.L., Kemper W.S., Franklin, D.L., 1968, Blood flow and pressure in the giraffe carotid artery, Comparative Biochemistry and Physiology 24, 1035-1042. https://doi.org/10.1016/0010-406X(68)90816-5. [ Links ]
Van Niekerk, J.W., Pienaar, U. de V., Fairall, N., 1963, Immobilizing drugs used in the capture of wild animals in the Kruger National Park, Journal of South African Veterinary Medical Association 34(3), 403-411. [ Links ]
Vitali, F., Kariuki, E.K., Mijele, D., et al., 2020, Etorphine-azaperone immobilisation for translocation of free-ranging Masai giraffes (Giraffa camelopardalis tippelskirchi): a pilot study, Animals 10, 322. https://doi.org/10.3390/ani10020322. [ Links ]
Wildlife Pharmaceuticals, 2010, Veterinary Medicine Package Insert Trexonil (Injection), Wildlife Pharmaceuticals Ltd. White River, South Africa 2 pp. [ Links ]
 Correspondence:
Correspondence:
S Ferguson
Email: sara@giraffeconservation.org

{kind=link}