










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309Print version ISSN 1681-150X
SA orthop. j. vol.23 n.1 Centurion 2024
https://doi.org/10.17159/2309-8309/2024/v23n1a8
CASE REPORT
ORTHOPAEDIC ONCOLOGY AND INFECTIONS
3D printing in osteosarcoma of the scapula: a unique case
Dheeraj MakkarI, ; Ravi SauhtaII
INC Medical College, Panipat, Haryana, India
IIArtemis Hospital and NC Medical College, Panipat, Haryana, India
ABSTRACT
BACKGROUND: Osteosarcoma is a malignant tumour that typically originates in long bones. We present a case of a subject afflicted by osteosarcoma in the left shoulder, an extremely uncommon location.
CASE REPORT: The subject, a 14-year-old adolescent, presented with a manifestation of osteosarcoma in an atypical location, namely the left shoulder. Radiographic analysis, including scapula plain radiograph, identified a radiodense lesion. Subsequent computed tomography disclosed compromised cortical integrity without medullary tissue involvement. Histological verification confirmed osteosarcoma. The absence of a commercially available suitably sized endoprosthesis for this unique anatomical location prompted the innovative use of a 3D-printed version based on the dimensions of the unaffected right shoulder. Post scapulectomy, a hernia mesh was employed for glenoid capsule reconstruction, ensuring subluxation prevention and yielding excellent postoperative outcomes.
DISCUSSION: This case underscores the complexities and innovations in osteosarcoma treatment when occurring in unconventional anatomical sites, exemplified by its manifestation in the scapula. The integration of 3D-printing technology emerges as a promising avenue for tailoring solutions in orthopaedic oncology, particularly addressing the constraints posed by the absence of commercially available devices for rare anatomical locations.
CONCLUSION: Managing scapular osteosarcoma necessitates innovative approaches. The incorporation of 3D-printing technology and the unconventional use of hernia mesh exemplify a viable strategy for achieving successful outcomes in challenging cases, emphasising the importance of adapting techniques to unique clinical scenarios.
Level of evidence: Level 4
Keywords: osteosarcoma, printing, scapula, endoprosthesis
Introduction
Osteosarcoma is a rare malignant bone tumour, accounting for less than 1% of all cancers. Around 70 000 new cases of invasive cancer are identified annually among 15- to 39-year-old adolescents and young adults (AYAs).1,2 It most commonly affects the long bones of the arms and legs, but can also arise in the flat bones of the body, such as the scapula. Chondrosarcomas constitute the most prevalent primary malignancy of the scapula in adults, whereas Ewing sarcoma is the commonest malignancy of the scapula in children.2 We present the case of a 14-year-old boy who reported with a dorsal surface osteosarcoma inhibiting his shoulder movement along with night pain. We explained the approach to the patient and obtained written consent from his parents and his assent for publication of the case report and accompanying images.
Case presentation
A 14-year-old male presented with a six-month history of left shoulder pain and limited range of motion. He had no significant past medical history or family history, and denied any history of trauma or infection to the left shoulder. The pain was initially mild and intermittent but had progressed to become constant and severe, especially at night. He reported difficulty sleeping and performing his daily activities due to the pain.
Physical examination
On examination, the patient had significant tenderness and warmth over the left scapular region. There was a palpable mass measuring approximately 10 × 4 cm. The skin over the mass was normal in colour and texture but a large number of dilated veins were visible on the left shoulder (Figure 1).The lump was firm in consistency and relatively immovable. There was no evidence of axillary and supraclavicular lymphadenopathy. The range of motion of the shoulder was restricted, and there was no evidence of neurovascular compromise. Around 45° of abduction, 5° of adduction, 40° of flexion and 25° of external and internal rotation were noted in the left shoulder.

Diagnostic interventions
A plain radiograph of the left shoulder revealed a large, irregularly shaped lytic lesion with areas of sclerosis involving the scapula. A computed tomography (CT) scan with contrast was performed, which showed a large destructive lesion involving the scapula with cortical destruction and soft tissue extension (Figure 2). Further evaluation with magnetic resonance imaging (MRI) demonstrated a large, heterogeneous mass involving the scapula with cortical destruction and extension into the adjacent soft tissue. The chest and pelvic CT bone scan did not reveal any metastasis, while the blood alkaline phosphatase and LDH levels were 2 000 and 3 200 IU/ l, respectively.

The patient was staged as T3N0M0 according to the American Joint Committee on Cancer (AJCC) staging system.
The patient was operated on by the senior surgeon and underwent a surgical biopsy that was sent to histopathology. The procedure was performed in a lateral fashion and histopathology revealed a high-grade osteosarcoma with spindle cell and osteoid production. The tumour was positive for the osteoblastic marker, osteocalcin.
Therapeutic interventions
The patient underwent neoadjuvant chemotherapy with cisplatin and doxorubicin. After three cycles of chemotherapy, repeat imaging showed a significant reduction in the size of the tumour.
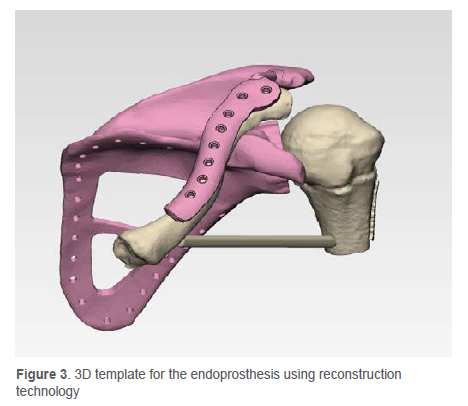
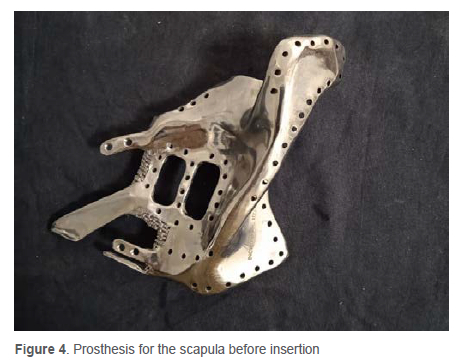
The treatment approach involved a left-side scapular resection and subsequent reconstruction utilising an endoprosthesis. To optimise the surgical outcome and ensure a precise fit, advanced 3D-printing technology was employed to create a customised endoprosthesis that accurately mirrored the unique anatomy of the patient's right scapula (Figures 3 and 4).
Surgery
The right floppy decubitus position was used to do a scapulectomy. The biopsy scar was to be carefully included into the S-shaped technique. A utilitarian incision was made commencing at the lateral margin of the scapula, running superiorly to the acromioclavicular joint, and then proceeding anteriorly to the coracoid. A sizable flap of fascia and skin was established posteriorly. The latissimus dorsi muscle was mobilised without cutting it and the rhomboids and trapezius muscles were freed.
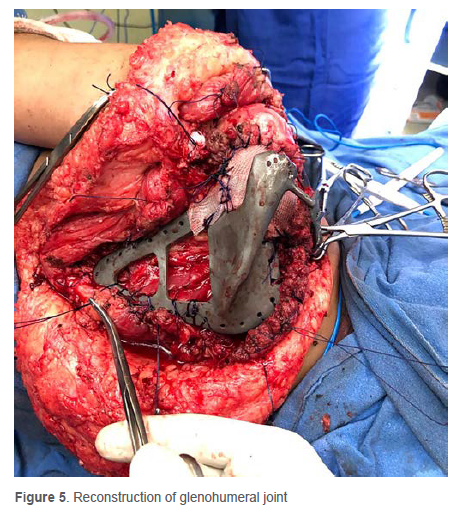
The periscapular muscles were dissected with sufficient margin, en bloc resection, as conservatively as feasible. The glenohumeral joint was opened up after a meticulous dissection of the axillary neurovascular bundle. The scapula was resected intra-articularly after arthrotomy; we attempted to preserve the humeral aspect of the shoulder capsule and the rotator cuff to aid in reconstruction (Malawerscapular resection type 3).3 The humerus was supported from the clavicle by hernia mesh (static suspension) and the conjoint tendon and the rotator cuff (dynamic suspension) (Figure 5). The surgical specimen was sent to the pathology department and the wound closed over the drain.
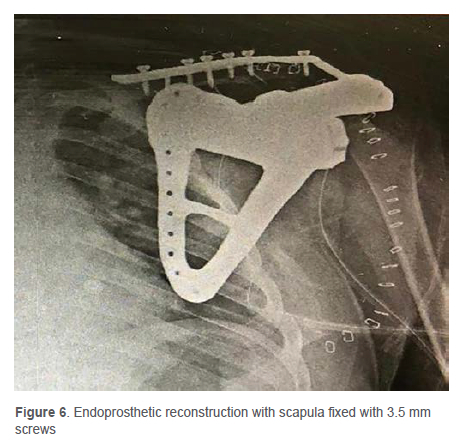
The scapula was reconstructed with a custom-made scapula. The prosthesis was fixed in position with screws to the clavicle (Figure 6). The glenoid was reinforced with a hernia mesh to prevent the destruction of articular cartilage of the humeral head by preventing subluxation of the head.
We anchored the scapular endoprosthesis to the serratus, which served as the implant's bed, along with the trapezius superiorly, rhomboids major and minor on the medial side, and deltoid, teres major and latissimus dorsi on the axillary side, suturing them back through the fenestrations in the endoprosthesis using Polydioxanone number one (PDS 1) thread. The deltoid and trapezius muscles were retained and coupled by tenodesis. The latissimus dorsi muscle was also rotated to cover the prosthesis.
Pathologic examination of the surgical specimen confirmed the diagnosis of osteosarcoma with negative margins. The patient received six cycles of adjuvant chemotherapy with vincristine, doxorubicin, cyclophosphamide and mesna.
Follow-up and postoperative course
The patient's shoulder was immobilised for six weeks with an elbow sling. Early elbow and finger mobilisation was performed. The initial follow-up appointment allowed for confirmation of the resection margins and proper wound healing. After 15 days, the sutures were removed and the site inspected for dehiscence (Figure 7).

The patient was followed up regularly with imaging studies, which showed no evidence of local recurrence or distant metastasis. The patient has been disease-free for the past two years and has resumed his normal activities. The functional and emotional outcomes were measured using the Musculoskeletal Tumor Society (MSTS) and the Toronto Extremity Salvage Score (TESS) scores.
Discussion
Osteosarcoma of the scapula is a rare entity, accounting for less than 1% of all osteosarcomas. It can significantly decrease shoulder joint functionality and reduce a patient's life.4 Numerous variables and situations, such as radiation, chemical carcinogens, metal implants, trauma, viruses, Paget's disease, past benign bone tumours and some congenital skeletal dysplasias have been identified as probable aetiologic agents in the emergence of osteosarcoma.5 In our case it was a sporadic occurrence.
In most instances, limb-sparing removal of scapular tumours involves humeral suspension, allograft transplantation, external deactivation replantation, arthrodesis and prosthesis replacement.6 Most humeral suspensions have been done after total scapulectomy. However, the humerus cannot lift the arm if the shoulder is low and the shoulder joint cannot move well, especially when the upper limb is unable to support its weight properly.4
The results of partial scapulectomy are superior to the total scapulectomy with endoprosthetic reconstruction. This was contrary to our case as we placed an anatomically sized prosthesis after 3D printing from the right side and custom-making a titanium endoprosthesis. The traditional approach suggests the resection of coracoid, distal end clavicle and rotator cuff;7 however, after removing the coracoid, we attempted to maintain the rotator cuff and the conjoint tendon. It resulted in a superb shoulder profile, stability, and functionality both active and passive. In our case, the MSTS and TESS scores were 28/35 and 80/100, respectively, higher than comparable studies. The seven components of MSTS are as follows: discomfort, range of motion, strength, joint stability, joint deformity, emotional acceptance and overall function.8 The excellent score indicates the emotional acceptance of the prosthetic by the patient. The patient contributes to the TESS questionnaire in order to provide a subjective evaluation of the procedure.
Typically, dacron fibre tapes are utilised to repair the shoulder joint; however, we used a hernia mesh with good results.3 Hernia mesh is an inexpensive and widely accessible alternative to dacron fibre tape.
We encountered challenges during the surgery. As a result of the destruction of normal anatomical characteristics by the malignancy, there were no reliable surgical landmarks for scapula removal. The endoprosthesis had to fit securely, so we utilised 3.5 mm cortical screws to secure it to the clavicle and used hernia mesh to reconstruct the glenohumeral joint. We strengthened the glenohumeral area with the conjoint tendon and the remaining rotator cuff using PDS sutures because suspension has been associated with a poor functional outcome. Tenodesis was performed on the muscles, and latissimus dorsi was used to wrap the prosthesis. The tenodesis involved the utilisation of Ethibond sutures to anchor the deltoid muscle to the humerus and the trapezius muscle to the clavicle. Preserving humeral head should take on paramount significance in cases where the tumour does not undermine its structural integrity or the overall survival. It has both functional and aesthetic value.
Conclusion
3D-printing technology can meet the demands of a highly personalised design, demonstrating distinct advantages. For the restoration of the glenohumeral capsule, hernia mesh is a cost-effective and readily available alternative to fibre tape, and conjoint tendon should be preserved if possible as it adds to the stability and contour of the shoulder. Neoadjuvant chemotherapy followed by surgical resection with negative margins along with endoprosthetic reconstruction is the treatment of choice for osteosarcoma. The prognosis is similar to that of osteosarcoma in other extremities.
Ethics statement
Prior to commencement of the study, ethics approval was obtained from the Institutional Ethics Committee NC Medical College & Hospital, Panipat, Haryana, India (ref: IEC/Approval/2023/45).
The procedure was explained to the patient in his native tongue and permission was obtained from his parents to submit the report and accompanying images for publication.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
DM: study conceptualisation, data capture, first draft preparation and manuscript revision
RS: review of manuscript, main surgeon, study design
ORCID
Makkar D https://orcid.org/0000-0002-8498-7935
Sauhta R https://orcid.org/0000-0002-5488-8047
References
1. Close AG, Dreyzin A, Miller KD, et al. Adolescent and young adult oncology-past, present, and future. CA Cancer J Clin.Nov 2019;69(6):485-96.https://doi.org/10.3322/caac.21585 [ Links ]
2. Tabone MD, Terrier P, Pacquement H, et al. Outcome of radiation-related osteosarcoma after treatment of childhood and adolescent cancer: a study of 23 cases. J Clin Oncol. Sep 1999;17(9):2789-95. https://doi.org/10.1200/JCO.1999.179.2789 [ Links ]
3. Bickels JK, Wittig JC, Kollender Y, et al. Limb-sparing resections of the shoulder girdle. J Am Coll Surg. Apr 2002;194(4):422-35. https://doi.org/10.1016/s1072-7515(02)01124-9 [ Links ]
4. Mayil Vahanan N, Mohanlal P, Bose JC, et al. The functional and oncological results after scapulectomy for scapular tumours: 2-16-year results. Int Orthop. Dec 2007;31(6):831-36. https://doi.org/10.1007/s00264-006-0261-1 [ Links ]
5. Bedi HS, Kaufman DV, Choong PF, Slavin JL. Osteosarcoma of the scapula arisingin osteogenesisimperfecta. Pathology. Feb 1999;31(1):52-54.https://doi.org/10.1080/003130299105557 [ Links ]
6. Inoue M, Otsuka K, Shibata H. Circulating tumor cell count as a biomarker of a specific gastric cancer subgroup characterized by bone metastasis and/or disseminated intravascular coagulation - an early indicator of chemotherapeutic response. Oncol Lett. Feb 2016;11(2):1294-98. https://doi.org/10.3892/ol.2015.4056 [ Links ]
7. Malawer MM. Tumors of the shoulder girdle. Technique of resection and description of a surgical classification. Orthop Clin North Am. Jan 1991;22(1):7-35. [ Links ]
8. Bolia IK, Savvidou OD, Kang HP, et al. Cross-cultural adaptation and validation of the Musculoskeletal Tumor Society (MSTS) scoring system and Toronto Extremity Salvage Score (TESS) for musculoskeletal sarcoma patients in Greece. Eur J Orthop Surg Traumatol. 2021;31(8):1631-38. https://doi.org/10.1007/s00590-021-02921-5 [ Links ]
Received: May 2023
Accepted: September 2023
Published: March 2024
Editor: Prof. Theo le Roux, Department of Orthopaedics, University of Pretoria, Pretoria, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research. No form of assistance was received from the implant companies involved in the surgery.
* Corresponding author: makkardheeraj@gmail.com
