










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309Print version ISSN 1681-150X
SA orthop. j. vol.24 n.2 Centurion 2025
https://doi.org/10.17159/2309-8309/2025/v24n2a1
SHOULDER AND ELBOW
Evaluation of surgical management strategies for chronic anterior shoulder dislocations: a retrospective analysis of 34 patients
Pududu A RachueneI, II, ; Mashupse P PhalaI; Thabang T RachoeneI; Chuene S MathibaI; Frederick J du ToitI; Roopam DeyIII, IV, V
IDepartment of Orthopaedic Surgery, Dr George Mukhari Academic Hospital, Sefako Makgatho Health Sciences University, Pretoria, South Africa
IIDepartment of Orthopaedics, Steve Biko Academic Hospital, University of Pretoria, Pretoria, South Africa
IIIDepartment of Human Biology, Division of Biomedical Engineering, University of Cape Town, Cape Town, South Africa
IVBiomedical Engineering Research Centre (BMERC), University of Cape Town, Cape Town, South Africa
VHealth through Physical Activity Lifestyle and Sports (HPALS), University of Cape Town, Cape Town, South Africa
ABSTRACT
BACKGROUND: Chronic anterior shoulder dislocations are uncommon; however, they pose a substantial challenge and necessitate a complex treatment decision-making process. This study aims to contribute to the existing literature by examining the surgical treatment outcomes of chronic anterior shoulder dislocations, focusing on surgical treatment methods and outcome measures.
METHODS: This retrospective study analysed prospectively collected data from 34 patients with chronic anterior shoulder dislocations treated between February 2020 and December 2022. Four surgical procedures were reviewed: open reduction and rotator cuff and/or capsulolabral repair (n = 7); open reduction and Latarjet procedure (n = 7); open reduction and iliac crest autograft (n = 9); and reverse shoulder arthroplasty (RSA) (n = 11).
RESULTS: The mean age of patients was 67 years, with 65% male. Falls were the most common cause of injury (68%). The average time from dislocation to relocation in this cohort was 28 weeks. Preoperative evaluations revealed delayed presentation due to self-neglect and healthcare access issues, with 41% misdiagnosed initially. Surgical interventions varied, with an average follow-up of 14 months (range: 3-52). RSA showed excellent patient-reported outcomes ratings, measured by the Oxford Shoulder Score (OSS) and Constant Shoulder Score (CSS), along with low complication rates observed at 14 months. Bone block procedures demonstrated good to excellent outcomes without recurrent dislocations. Joint preservation procedures had high complication rates.
CONCLUSION: Managing neglected anterior shoulder dislocations is complex, necessitating customised surgical approaches to optimise outcomes and minimise complications. Despite a heterogeneous patient population with significant functional demands, bone block procedures and RSA emerged as effective treatments.
Level of evidence: 4
Keywords: chronic anterior shoulder dislocation, joint preservation surgery, reverse shoulder arthroplasty, surgical outcomes
Introduction
Chronic anterior shoulder dislocations pose a significant difficulty in orthopaedic practice, especially in low-income countries where restricted access to and availability of healthcare resources can result in delayed identification and treatment.1,2 The definition of chronic shoulder dislocation varies in the literature, with treatment delays of seven days, ten days, or three weeks being used. However, it consistently refers to cases with unsuccessful closed reduction due to prolonged duration of dislocation.2-4 Chronic dislocations can result in severe bone loss and joint degeneration, presenting substantial difficulties for orthopaedic treatment. Recent advancements in reverse shoulder arthroplasty (RSA), highlighted by Hyun et al., have increased the utilisation of RSA for managing chronic dislocations.5 While various surgical options exist for these patients, including joint preservation techniques with open reduction and capsulolabral repair, bone block procedures, hemiarthroplasty, and RSA, previous studies have reported suboptimal outcomes. This underscores the need for a deeper understanding of approaches to manage these complex cases effectively.1,2,6-8
The aim of this study was to examine the surgical treatment of chronic anterior shoulder dislocations in a heterogeneous population, and the outcomes of the procedures, as there is a distinct lack of published material on the outcomes of surgical procedures. Our goal is to highlight the challenges associated with the technical surgical procedures, the functional implications, and the decision"making process for diagnosis and treatment.
Methods
This retrospective study utilised prospectively collected data to investigate 34 patients with chronic anterior shoulder dislocations treated between February 2020 and December 2022. Chronic dislocation was defined as a dislocation lasting for more than ten days, where either closed reduction had failed or the likelihood of achieving and maintaining a successful reduction was considered low. All patients underwent surgical intervention by the same surgeon, and four treatment procedures were reviewed: open reduction and soft tissue (rotator cuff repair and/or capsulolabral repair) (n = 7); open reduction and Latarjet procedure (n = 7); open reduction and iliac crest autograft (n = 9); and RSA (n = 11). The decision-making process for each patient was determined based on the chronicity of the dislocation, categorised as early (3-6 weeks), late (6-12 weeks), or ancient (> 12 weeks), as initially proposed by Goga.2 Other considerations included patient demographics (age and sex), functional demands, degree of bone loss, and associated injuries. Exclusion criteria comprised congenital and neurological dislocations, non-surgically treated cases, and those with associated surgical or anatomic neck fractures. Ethical clearance was obtained from the institutional review board. The statistical analysis of intra-cohort correlation and inter-cohort differences was conducted using IBM SPSS v28. The criterion for statistical significance was a p-value less than 0.05.
Results
Clinical data
At the time of surgery, the sample population had a mean age of 67 years (range 23-80), with 65% being male. Approximately 32% of the patients were retirees, while the remainder consisted of young patients with significant functional requirements. Notably, two patients had a history of chronic alcohol use, Ave were HIV-positive, one had intractable epilepsy, and another a psychotic disorder. Falls were the most common cause of injury (68%), with two patients attributing their dislocation to seizures. Of the patients, 17 had late chronic dislocation, followed by 12 with ancient chronic dislocation, and only three with early chronic dislocation.
Preoperative evaluation
Preoperatively, patients were assessed for delayed presentation reasons, associated injuries, functional restrictions, pain and expectations. Most patients (66%) sustained an injury to their dominant arm. The primary causes for delayed presentation were self-neglect and difficulties in accessing healthcare, while in 41% of cases, the regional hospital responsible for initial treatment missed the acute dislocation diagnosis, leading to inappropriate treatment. Clinical examination identified axillary nerve injury in 12% of patients. No other neurological injuries were identified. All patients underwent X-ray imaging, with half (n = 17) also undergoing preoperative CT scans to assess bone loss extent. For patients without preoperative CT scans, the amount of bone loss was assessed intraoperatively, and the final decision regarding the appropriate procedure was determined during surgery. Our preoperative decision making primarily considers patient age. In young patients (< 60 years), we prefer joint preservation surgery with open reduction and anterior bone block procedures. The Latarjet procedure is typically preferred, but for patients with epilepsy, mental health concerns or ancient dislocations with large anterior glenoid bone loss (> 25%), we opt for the Eden-Hybinette procedure. If a Hill-Sachs lesion is significant (20-30%), we consider adding a remplissage. Although we have not encountered cases with > 30% humeral head bone loss, options could include supervised neglect, bone graft, hemiCAP, or hemiarthroplasty in such cases.
For older patients (> 60 years) with early chronic dislocation and minimal bone loss (< 25%), we would perform rotator cuff and capsulolabral repairs; for those with late or ancient dislocations, we perform RSA. Our approach to managing glenoid defects aligns with general literature guidelines on the stability of the baseplate.
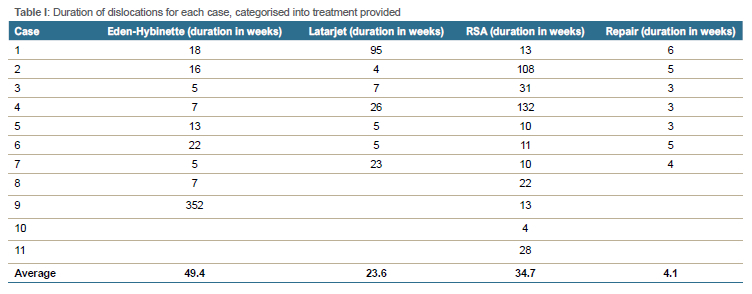
Surgical procedures
Surgical interventions included RSA (n = 11); the Eden-Hybinette technique (autologous iliac crest bone block, double screw fixation) (n = 9); the Latarjet procedure (coracoid transfer, subscapularis split, double screw fixation) (n = 9); and repair treatments (n = 7). The durations of dislocations are presented in Table I. Male patients dominated the Eden-Hybinette (100%), Latarjet (89%), and RSA (72%) groups, while soft tissue repair procedures exhibited a sex disparity (29% male) and a higher mean age (71 years). These findings show the variability in surgical management strategies employed in addressing chronic anterior shoulder dislocations in our study cohort.
Out of the patients who underwent bone block procedures (Latarjet or Eden-Hybinette), 31% of them had open reduction executed with the assistance of lesser tuberosity osteotomy or subscapularis tenotomy. Additionally, 19% of the patients had a greater tuberosity fracture malunion that required corrective osteotomy. Two patients had complete rotator cuff tears, with one tear affecting the infraspinatus and supraspinatus tendons, and the other tear affecting the subscapularis tendon. These tears were surgically repaired using suture anchors. In the Latarjet group, the capsule was repaired to the remaining coracoacromial ligament, while in the Eden-Hybinette group, it was anchored to the glenoid using a single labral repair suture anchor. All patients in a group undergoing soft tissue repair had extensive rotator cuff tears that were repaired using suture anchors. Subsequently, the shoulder was assessed for stability. If instability persists following reduction and rotator cuff repair, the surgeon will proceed with a bone block procedure. In cases where the rotator cuff tear is deemed irreparable, RSA will be performed. Additional surgeries were performed on Ave of these patients, including capsulolabral repair in three cases and remplissage in two cases.
RSA surgery was conducted through a single-staged method using a deltopectoral approach. Delta Xtend prostheses with a 4 mm distalised glenosphere (DePuy Orthopaedics, Warsaw, IN, USA) were used in nine patients, while Aequalis reversed shoulder prostheses (Tornier, Saint-Ismier, France) were used in two patients. Subscapularis repair was conducted on two patients, based on the surgeon's assessment of its reparable condition. Three patients with peripheral glenoid bone loss above 40% of the glenoid surface had a glenoid bone graft using the excised humeral head. A conventional polyethylene cup was utilised in eight individuals, whereas one patient required a constrained cup to ensure stability.
Postoperative follow-up data
The data were carefully examined for specific information on patient-reported outcome measures (PROMs) after surgery, with a minimum follow-up time of three months. Postoperative clinical data collected included rates of redislocation and instability as well as neurovascular complications. Postoperative PROMs and radiographic findings were recorded. In our institution, patients who have joint preservation surgery for shoulder dislocation are assessed using the Subjective Shoulder Value (SSV) and Rowe Score. Patients who undergo arthroplasty are evaluated using the Oxford Shoulder Score (OSS) and Constant Shoulder Score (CSS). These evaluation measures are considered the standard of care in our unit.
The average follow-up period for the patients was 14 months (range: 3-52). Due to acute postoperative problems, two patients were excluded from the follow-up study. Additionally, one patient was lost to follow-up. Consequently, the total follow-up rate was 84%.
Patient-reported outcome measures
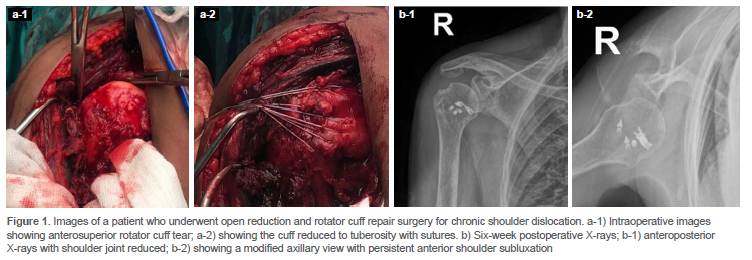
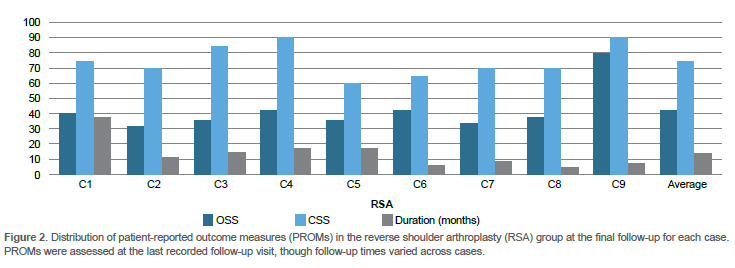
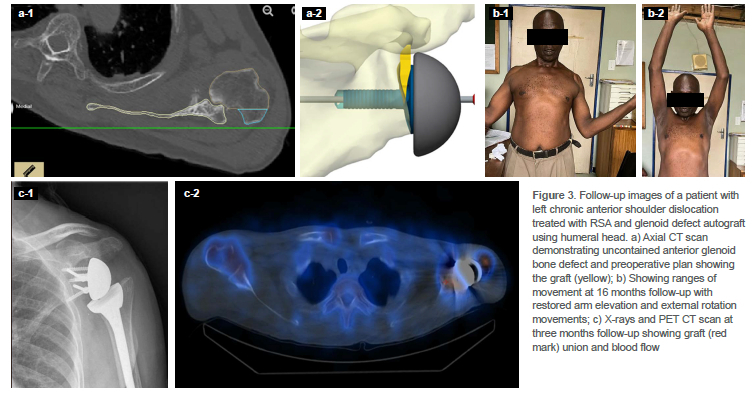
PROMs in joint-preserving procedures are presented in Figure 1. By category, in the Eden-Hybinette group, the SSV averaged 70%, while the Rowe Score reached 75, with a follow-up duration of 14 months. For the Latarjet procedure, the SSV and Rowe Score were 68 and 71, respectively, over a follow-up period of nine months. Soft tissue repair procedures exhibited SSV and Rowe Score values of 66 and 62, respectively, with a follow-up duration of 11 months. The outcomes were categorically good in the Eden-Hybinette group, fair to good in the Latarjet group, and fair in the soft tissue repair group. The mean results for RSA demonstrated an OSS of 42.1 and a CSS of 74.8, with an average follow-up period of 14.1 months. Figure 2 illustrates the distribution of PROMs in this cohort. The PROMs were evaluated at each patient's most recent follow-up appointment, with follow-up durations differing among cases and ranging from 5-28 months. Figure 3 shows clinical photographs, X-rays, and a PET scan taken at the 3-month follow-up of a patient who underwent RSA, demonstrating restored range of motion and evidence of bone graft healing with perfusion.
Complications
In 23 patients who underwent joint-preserving surgery, we observed an overall complication rate of 48%. There was a significant correlation between the length of the dislocation and the probability of complications; 82% of complications were seen in the group with ancient dislocations (p < 0.05). Complications among patients who underwent joint preservation surgery included three cases (13%) of transient axillary nerve injury, nine cases (39%) of persistent glenohumeral joint (GHJ) subluxation, one case (4%) of humeral head collapse, and 11 cases (17%) of glenohumeral joint osteoarthritis (GHJOA). In total, there were 30 complications, and one patient (4%) required reoperation due to recurrent dislocation.
Among the subset of patients scheduled for RSA (n = 10), we observed a 20% incidence of complications. One case, planned for RSA, experienced an axillary artery rupture, necessitating postponement of the procedure. Additionally, a single instance (10%) of humeral calcar periprosthetic fracture was recorded. Notably, there were no cases of periprosthetic joint infection (PJI), instability, or acromial/coracoid fracture.
Discussion
Surgical management of chronic anterior shoulder dislocations remains a significant challenge for orthopaedic surgeons. This study evaluated outcomes of surgery in these patients. The study population was diverse, encompassing individuals of various ages, with the majority (68%) having notable functional demands and occupational obligations. This group may have high expectations regarding recovery time, functional outcomes, and resuming occupational duties. The primary factors contributing to delayed presentation were related to limited access to and insufficient availability of high-quality healthcare. Severe glenoid and humeral bone loss, intrinsic shoulder structural injuries accompanied by excessive fibrosis, are frequently observed in these patients.1 These pose challenges for conventional techniques to achieve open reduction and structural repair, and joint stability maintenance. The severity of these issues frequently corresponds to the length of the dislocation.2 While supervised neglect remains an option for low demand patients despite the risk of persistent pain and poor function, choice of surgery is difficult and a high rate of unsatisfactory results is reported.1 This is guided by duration of dislocation, degree of soft tissue injury and presence of bone loss and/or fractures, patient age and functional requirements. In this study, most of the patients were treated with bone block procedures (free iliac crest = 9; coracoid transfer = 7). Despite conflicting reports in the literature regarding the efficacy of bone blocks in elderly patients and those with neglected dislocations, with some authors advising against their use,6,9,10 we found them to be a feasible option for managing chronic dislocations, achieving favourable outcomes ranging from good to excellent. We observed no recurrent dislocations with this procedure and the PROMs were not affected by the high complication rate observed. In comparison to the series presented by Goga,2 none of the patients in our series needed transarticular K-wire fixation to maintain joint reduction. Li et al. reported a 48% rate of redislocation or subluxation with coracoid transfer performed via subscapularis tenotomy and repair, whereas no redislocation occurred when the procedure was conducted through a subscapularis split.11 In our study, we observed one case of anterior subluxation and one of inferior subluxation.
Among the patients treated with rotator cuff and capsulolabral repair, reduction was achieved in six out of seven cases, with an average dislocation duration of 4.1 weeks (range 3-6). Notably, four patients (67%) in this group experienced persistent joint subluxation, which was associated with poorer PROMs. These findings are consistent with pooled data from Sahu et al.'s systematic review of 53 shoulders across seven studies, in which 30.8% (four of 13) of patients treated with rotator cuff and capsulolabral repair experienced persistent humeral head subluxation. Among these cases, two exhibited anterior instability, and two showed superior instability, indicating potential rotator cuff repair failure.10 Overall, we observed a significant correlation between the duration of dislocation and the risk of complications in the cohort treated with joint preservation procedures.
Patients undergoing RSA were generally older and showed overall better PROMs compared to other treatment groups. Additionally, this group experienced lower complication rates. Three patients required glenoid reconstruction using a structural humeral head bone graft, with follow-up imaging at three, seven and 24 months revealing no significant graft resorption. High revision rates have been attributed to failure in addressing bone defects.12 Notably, no instances of instability were recorded in the RSA group, and our study consistently demonstrated predictable outcomes with good to excellent measures in these patients. Conversely, Werner et al. documented the successful treatment of 21 patients with chronic anterior shoulder dislocation, with an average dislocation duration of six months (range 3-11), utilising RSA combined with bone grafting for significant glenoid defects. Within the initial two years following the procedure, they observed baseplate loosening in two patients, necessitating revision surgery.13 Raiss et al. reported fair outcomes in a series of 22 patients over an average follow-up of 3.5 years.12 One patient in our study with chronic anterior shoulder dislocation of the subclavicular type experienced a major vascular injury during the procedure, highlighting the proximity of the humerus to the axillary artery in dislocated positions. We have since implemented CT angiography as part of the preoperative workup and have been requesting the presence of a vascular surgeon on standby for this subgroup of patients.
When planning for the surgery in these patients it is advisable to obtain a CT scan to plan for bone defects.12 One should also obtain an MRI to assess the soft tissue status when resources are available, as we have observed cases that are associated with significant rotator cuff injuries. Additionally, literature documents age-related incidence of rotator cuff tears associated with dislocations.13,14
Early discussions on surgical processes and considerations date back to 1934, with recent studies exploring the role of arthroscopic release for reduction assistance.2,14 To achieve successful outcomes in neglected anterior shoulder dislocations, our approach incorporates several critical strategies. We emphasise avoiding closed reduction or forceful manoeuvres in dislocations over four weeks, due to high failure rates and potential risks of vascular and neurological injury. Ensuring humeral mobility and clearing fibrous tissues from the joint before reduction is crucial. Accessing the humeral head and glenoid through the rotator cuff interval, identified by the coracoid base, is essential to prevent cuff interference. We retain the long head of the biceps until the reduction and repair stages to aid in glenoid localisation. Early coracoid osteotomy may be considered for Latarjet procedures to enhance exposure. Excising intra-articular fibrous tissue and releasing scarring and the anterior and posterior capsules while safeguarding the inferior capsule to protect the axillary nerve are pivotal steps to concentric reduction. Using a Cobb retractor facilitates removal of extra-articular fibrosis in the subacromial and subdeltoid regions. Partial tenotomy of the upper pectoralis major and cautious subcoracoid release with a finger sweep technique are options when other measures fail. In rare instances, subscapularis tenotomy or lesser tuberosity osteotomy may be necessary to address challenges such as the pseudoglenoid on the scapula, ensuring unrestricted movement of the subscapularis. All patients were immobilised for six weeks, and passive range of motion exercises and pendulum movements were initiated at two weeks.
Despite strengths such as a diverse patient cohort and comprehensive treatment insights, limitations of the study include its retrospective nature, potential biases, and a relatively small sample size affecting statistical power and generalisability. Conducted at a single centre, the findings may not fully reflect practices in other healthcare settings. Furthermore, variability in treatment approaches and a potentially short follow-up period may limit definitive conclusions on long-term outcomes and complications.
Conclusion
The population in our study was heterogeneous, primarily consisting of people with significant functional demands and occupational responsibilities. The surgical strategies for joint preservation were diverse, with a significant preference for bone block procedures, including free iliac crest and coracoid transfer, which demonstrated favourable outcomes and no recurrent dislocations, despite the high rate of complications. RSA, particularly in older patients, yielded satisfactory results. Based on the observation of this current study, we recommend RSA for elderly patients regardless of dislocation duration.
Acknowledgements
Miss Mpho Motlhake for her assistance with research protocol preparation and submission processes.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
Prior to commencement of the study, ethical approval was obtained from the Sefako Makgatho Health Sciences University Research committee (Reference number: SMUREC/M/16/2022: IR). All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed written consent was not obtained nor necessary as the study was retrospective in nature and used data that had been collected in routine clinical care.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
PAR: research ideation, preparation of the manuscript, final approval of the version to be published
MPP: compiled research protocol, data collection and critical editing of the version to be published
TTR: data collection and critical editing of the version to be published
CSM: data collection and critical editing of the version to be published
FJdT: data collection and critical editing of the version to be published
RD: data analysis and interpretation, and final approval of the version to be published
ORCID
Rachuene PA https://orcid.org/0000-0003-4045-5301
Phala MP https://orcid.org/0000-0002-8013-8290
Rachoene TT https://orcid.org/0009-0000-1322-903X
Mathiba CS https://orcid.org/0009-0004-4110-5818
du Toit FJ https://orcid.org/0000-0001-7045-1681
Dey R https://orcid.org/0000-0002-3616-1995
References
1. Sahajpal DT, Zuckerman JD. Chronic glenohumeral dislocation. J Am Acad Orthop Surg. 2008;16(7):385-98. [ Links ]
2. Goga IE. Chronic shoulder dislocations. J Shoulder Elb Surg. 2003;12(5):446-50. [ Links ]
3. Van Tongel A, Claessens T, Verhofste B, De Wilde L. Reversed shoulder arthroplasty as treatment for late or ancient chronic glenohumeral dislocation. Acta Orthop Belg. 2016;82(3):637-42. [ Links ]
4. Babalola OR, Vrgoc G, Idowu O, et al. Chronic unreduced shoulder dislocations: Experience in a developing country trauma centre. Injury. 2015;46:S100-102. [ Links ]
5. Hyun YS, Huri G, Garbis NG, McFarland EG. Uncommon indications for reverse total shoulder arthroplasty. Clin Orthop Surg. 2013;5(4):243-55. [ Links ]
6. Grey B, Ryan P, Bhagwan N. Treatment of chronic anterior shoulder dislocations: Limited goal surgery. SA Orthop J Spring [Internet]. 2016;15(1):68-72. Available from: http://dx.doi.org/10.17159/2309-8309/2016/v15n3a10 [ Links ]
7. Rouhani A, Navali A. Treatment of chronic anterior shoulder dislocation by open reduction and simultaneous Bankart lesion repair. Sport Med Arthrosc Rehabil Ther Technol. 2010;2(1):1-5. [ Links ]
8. Raiss P, Edwards TB, Bruckner T, et al. Reverse arthroplasty for patients with chronic locked dislocation of the shoulder (type 2 fracture sequela). J Shoulder Elb Surg. 2017;26(2):279-87. [ Links ]
9. Du Plessis JP, Lambrechts A, McGuire D, et al. Early and medium-term complications of the modified Latarjet procedure. SA Orthop J. 2014;13(3):50-56. [ Links ]
10. Sahu D, Rathod V, Phadnis A, Shyam A. Results and complications of head-preserving techniques in chronic neglected shoulder dislocation: a systematic review. J Shoulder Elb Surg [Internet]. 2021;30(3):685-94. Available from: https://doi.org/10.1016/jjse.2020.10.010 [ Links ]
11. Li Y, Jiang C. The effectiveness of the latarjet procedure in patients with chronic locked anterior shoulder dislocation a retrospective study. J Bone Jt Surg - Am Vol. [Internet]. 2016 May 18 [cited 2024 Jun 20];98(10):813-23. Available from: https://journals.lww.com/jbjsjournal/fulltext/2016/05180/the_effectiveness_of_the_latarjet_procedure_in.3.aspx [ Links ]
12. Raiss P, Edwards TB, Bruckner T, et al. Reverse arthroplasty for patients with chronic locked dislocation of the shoulder (type 2 fracture sequela). J Shoulder Elb Surg [Internet]. 2017;26(2):279-87. Available from: http://dx.doi.org/10.1016/jjse.2016.05.028 [ Links ]
13. Werner BS, Böhm D, Abdelkawi A, Gohlke F. Glenoid bone grafting in reverse shoulder arthroplasty for long-standing anterior shoulder dislocation. J Shoulder Elb Surg. 2014;23(11):1655-61. [ Links ]
14. Connolly S, Ritchie D, Sinopidis C, et al. Irreducible anterior dislocation of the shoulder due to soft tissue interposition of subscapularis tendon. Skeletal Radiol. 2008;37(1):63-65. [ Links ]
Received: July 2024
Accepted: January 2025
Published: May 2025
* Corresponding author: pududu.rachuene@up.ac.za
Editor: Dr Sean Pretorius, Stellenbosch University, Cape Town, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.

{kind=link}
{kind=link}
{kind=link}
{kind=link}