










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkJournal of Contemporary Management
On-line version ISSN 1815-7440
JCMAN vol.16 n.2 Meyerton 2019
https://doi.org/10.35683/jcm19030.0026
RESEARCH ARTICLES
Lean SPRInT: A management tool for initiating Lean in public hospitals in KwaZulu-Natal
L NaidooI; Z FieldsII,*
IUniversity of Kwa-Zulu-Natal. benzzn@gmail.com
IIUniversity of Johannesburg. ziskaf@uj.ac.za; (https://orcid.org/0000-0001-5353-1807)
ABSTRACT
South African public hospitals are beset with barriers to the realisation of strategic health outcomes owing to operational inefficiency. The Lean SPRInT aids managers with Lean implementation by assessing their hospitals' readiness status for Lean to improve operational efficiency.
An observational descriptive study employing quantitative methods was conducted across 73 public hospitals in KwaZulu-Natal (KZN). Simple random sampling was used to attain a minimum sample size of 218 senior managers who completed semi-structured questionnaires. Exploratory Factor Analysis was used to identify latent constructs. Confirmatory Factor Analysis was used to determine the reliability and validity of factors. Structural Equation Modelling assessed the acceptability of the model.
The participant response rate was 96.8% (n=211). Three Critical Success Factors (strategic leadership and organisational attitude; integration of Lean elements, tools and techniques; and basic stability in operational processes), from which the electronic Lean SPRInT was developed, were derived after several iterations of Exploratory Factor Analysis (EFA). All reliability and validity conditions have been met, thus rendering the model reliable and valid
Lean SPRInT is a management tool for assessing hospitals' readiness status for Lean. A six-step process for the deployment of Lean SPRInT is proposed. A phasic approach for Lean implementation, together with close monitoring using the HLA tool is recommended. Unified efforts and decentralised decision-making are more likely to lead to effective implementation.
Key phrases: Contemporary management tool; healthcare management; healthcare system; lean management and operational efficiency
1. INTRODUCTION
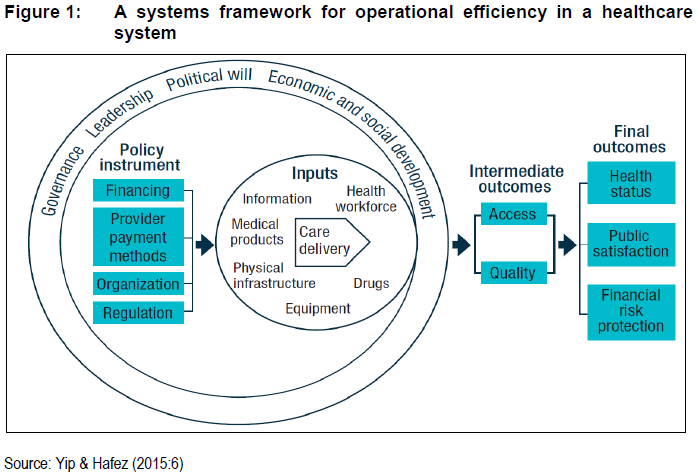
The ultimate goal of a healthcare system is to provide quality and affordable healthcare to society. A healthier nation would enjoy the benefit of financial risk protection and a satisfied population (Yip & Hafez 2015:5-6). Several resources inputs are impelled by policy instruments and form the recipe for quality of and access to healthcare which ultimately leads to the desired health benefit to society (Figure 1). Both healthcare quality and benefit is an important outcome of efficiency in the healthcare system that may lead to the achievement of improved access and quality with the least amount of resource inputs.
Lean thinking (or "Lean") is recognised as a systematic approach to improve efficiency by eliminating waste and pursuing perfection with minimal resources (Omogbai & Salonitis 2016:106; R0vik & Andersen 2015:1; Womack, Jones & Roos 2007:1). The primary focus of Lean is on reducing waste, synchronising flows and managing variability in (process) flows. A critical aspect of Lean is the empowerment of employees to make changes to their work, thereby improving processes from the floor upwards. On an organisational level, mapping the entire process allows management to augment process steps that are value-adding and relevant to the final product or service for the customer, while systematically eradicating those that fail to add value (Dickson, Singh, Cheung, Wyatt & Nugent 2009). Lean methodology is pinned on five tenets (Zidel 2006):
• Specify value by asking oneself what is valuable to the end-user (the patient);
• Identify the value stream using a Value Stream Map (VSM);
• Make the value stream flow by restructuring process steps and eliminating, non-value-adding steps (eliminating bottlenecks);
• Pull : The forerunning process down the value-stream signals when upstream activities can begin in order to stabilize demand on the system; and
• Pursue perfection through continuous improvement.
Wide scale adoption of such a management approach in healthcare facilities would contribute to the attainment of the aforementioned goal. See Figure 1 for a systems framework for operational efficiency in a healthcare system.
2. BACKGROUND
South African public healthcare facilities are beset with vastly apparent barriers to the realisation of strategic health outcomes. The framework depicted in Figure 2 provides a typical roadmap from organisational strategy to strategic outcomes, guided by organisational vision with strategic goals and often laden with barriers and enablers which widen or narrow the intervention-implementation gap, respectively. Failure to recognise and augment these enablers or "critical success factors" conjugately undermines their potential of narrowing the intervention-implementation chasm. This study is anchored on the development of a tool which assesses the status of the critical success factors which have the potential of narrowing the operational efficiency intervention-implementation gap.
Operational inefficiency derives from the sub-optimal processing of resource inputs in the healthcare system and leads to poor performance of the organisation in terms of measurable health care metrics and financial reports. Such inefficiency results from, inter alia, the mismatch between the genuine need (demand) for healthcare services and the supply thereof (over- and under-utilisation); expenditure on items such as drugs, sundries, blood products and laboratory services; inappropriate admissions and prolonged average lengths of stay; deviation from prescribed treatment protocols and medicine formularies; negative incidents and clinical errors and hospital-acquired infections (Madubula, English, Padayachee & Mkhize 2014).
Lean can be viewed as both a catalyst for interventions in an organisation on a continuous improvement journey and as an intervention itself which, through its tools and techniques, maximises service and production output with minimal resource inputs by eliminating waste and "doing better with less" (Improta, Romano, Di Cicco, Ferraro, Borrelli, Verdoliva, Cesarelli 2018:1-2; Mayosi & Benatar 2014:1351; Omogbai & Salonitis 2016:106). The Lean Success Predictor for Rapid Initiation Tool (Lean 'SPRInT') is a tool for healthcare managers to embark on the Lean transformation journey by assessing their hospitals' status of CSFs for Lean initiation.
Lean SPRInT is characteristically different from scrum methodology in that scrum is described as a process framework under the umbrella of Agile with four specific events to optimise the work carried out by small teams: Sprint Planning, Daily Scrum, Sprint Review and Sprint Retrospective (Reddy 2016; Sutherland & Schwaber 2013:3). As indicated by Beck, Beedle, Bennekum, Cockburn, Cunningham, Fowler, Grenning, Highsmith, Hunt, Jeffries, Kern, Marick, Martin, Mellor, Schwaber, Sutherland & Thomas (2001), Agile is a philosophy documented in the Agile Manifesto and espouses specific values that contribute to flexible, change-adaptable and quick manufacturing of products. These values of Agile highlight the importance of team member interactions, collaborations and adaptability to change to produce products incrementally.
Scrum has been used since the early 1990s to manage complex product development such as software. The term "sprint", in terms of the scrum framework is defined as a time period or time-box, usually 2 to 4 weeks, within which a potentially releasable product increment is created (Sutherland & Schwaber 2013:3). A scrum sprint can be regarded as a project with a specific time frame that is not more than a month. Lean SPRInT is accordingly not in any way related to scrum sprint and should not be confused with the methodology used in Agile Lean. Lean SPRInT is an acronym for an assessment tool that can be used by managers to assess the state of readiness for Lean implementation in hospitals.
Lean SPRInT could be used as an innovative means for the rapid but systematic initiation of Lean as a novel operations management approach in public hospitals across KwaZulu-Natal. This could result in widespread adoption of the practice of Lean by healthcare managers both in the public and private sectors nationwide. Successful Lean rollout in turn facilitates the narrowing of the intervention-implementation gap for the realisation of strategic goals. See Figure 2 for the Intervention-implementation gap in the organisational strategy roadmap.
3. LITERATURE REVIEW
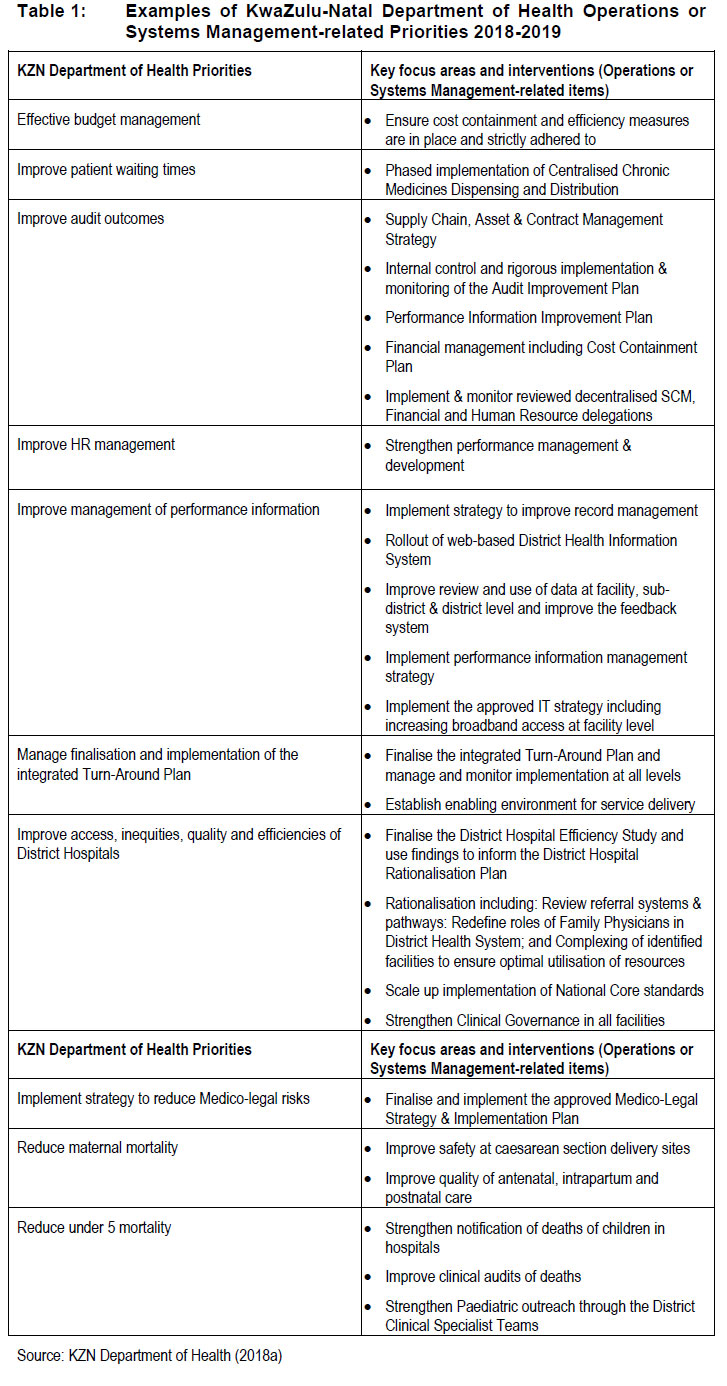
With the need for overhauling the health systems delivery platform in KwaZulu-Natal, the realisation of the strategic priorities in its health transformation agenda has become ever more exigent (KZN Department of Health 2018a, 2018b). Honing in on examples of operations or systems management priorities reflected in the KZN Department of Health's 2018-2019 Annual Performance Plan (Table 1), it is not unreasonable to deduce that a considerable portion of the KZN Department of Health priorities and goals are overtly in need of adroit managers with a sound management approach to be successfully addressed.
Against this backdrop, Lean is proposed as a contemporary approach to efficiently execute these systems management priorities. Research results show both successful and unsuccessful Lean implementation in various industries, indicating that CSFs for its initiation have to be recognised (Kundu 2012:302). There is scarce empirical literature to guide how Lean implementation is operationalized in healthcare (Burgess & Radnor 2013:220). There is limited evidence demonstrating the existence of tools for predicting at the outset the success of Lean initiation.
A seminal structure literature review of 177 research papers dating from 2000 to 2015 was conducted across several elements of health care operations management, including service quality, service operations strategy, service scheduling, service performance and frontline employees (Jha, Sahay & Charan 2016: 259-279). The literature review revealed that a large proportion of empirical studies have been conducted in developed nations (Jha et al. 2016: 271). This necessitates more healthcare operations management research in developing and underdeveloped countries due to the unique challenges experienced in these nations compared to the developed nations.
Evidence on the use of electronic tools for predicting the success of Lean initiation is lacking. It has been argued that existing Lean assessment tools provide qualitative analysis and do not provide any clear direction of where the improvement efforts should be directed (Srinivasaraghavan & Allada 2006:1159). In addition, there is limited research on tools that assist with Lean deployment strategy elements (Machado Guimaräes & Crespo de Carvalho 2014:3-4). The assessment tools identified in reviewed literature do not offer any success predictor instrument for Lean implementation in hospitals.
4. ETHICS
Research ethics approval (HSS/0031/016D) was obtained from the Human Social Sciences Research Ethics Committee (HSSREC) at the University of KwaZulu-Natal (UKZN). Permission was also obtained from the KZN Department of Health's Provincial Health Research and Knowledge Management unit (KZ_2016RP31_475) and Deputy Director General for Specialised Services and Clinical Support. Informed consent was obtained from all participants. Permission was granted by Dr. Danie Vermaak for the use of his research questionnaire elements in the formulation of the data collection tool for this study.
5. METHODOLOGY
The primary aim of this observational descriptive study which employed quantitative methods was to develop a Lean Success Predictor for Rapid Initiation Tool (Lean SPRInT) for the initiation of Lean in public hospitals across KwaZulu-Natal, South Africa.
5.1 Study site and sampling
The research was conducted across 73 public hospitals from a target population of 500 senior managers within the province of KZN. Simple random sampling was used.
For exploratory factor analysis, experts argue that the n:p ratio should be at least 3 to 6 subjects (n) per test item (p), set traditionally to a ratio of 5 to 1 but can be up to 20 to 1 (Kyriazos 2018:2223; MacCallum, Widaman, Zhang & Hong 1999:84-85; Schumacker & Lomax 2015:240). A sample size of at least 192 (based on a subject: item ratio of 6:1) was required. The planned sample size of senior managers, considering a 5% margin of error and 95% confidence interval, was 218. In terms of the proposition by MacCallum et al. (1999:89) that the sample size can be judged acceptable if the communalities are high (squared multiple correlation > 0.6) and factors relatively few in number (3 factors in this study), the sample of 211 is reliable (MacCallum et al. 1999: 89).
5.2 Data collection and analysis
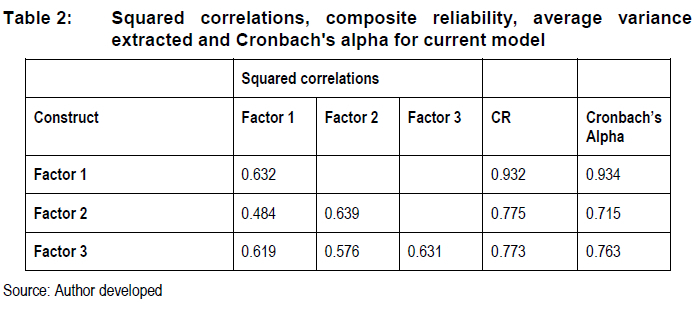
A self-administered, semi-structured questionnaire with mixed categorical, open-ended and variable Likert-scale questions was used for data collection. Cronbach's alpha was used to determine the internal consistency of the test items, looking particularly for homogeneity of items measuring latent constructs (Faith, Kim & Heo 2015:2) . Cronbach's alpha generally >0.7 was considered acceptable (Bujang, Omar & Baharum 2018:88-89; Taber 2018:1278, 1288). Cronbach's alpha for this study is reflected in Table 2. Data was reduced using EFA to identify latent constructs. Confirmatory Factor Analysis (CFA) was used to determine the reliability and validity (both convergent and discriminant) of these factors. Structural Equation Modelling (SEM) fit indices were then applied to assess acceptability of the measurement model.
6. RESULTS
The participant response rate was 96.8% (n=211). The results of the Likert scale ratings were used to identify three CSFs after several iterations of EFA.
6.1 Validity and reliability of model
The following conditions are required for reliability and validity of the model:

For this model, Table 2 shows the values of the indices used to assess for reliability and validity, based on the conditions specified above. Diagonals represent AVE and Alpha represents Cronbach's alpha reliability measure. Off diagonals represent squared correlations (also known as shared variance).
All reliability and validity conditions have been met, thus rendering the model reliable and valid.
6.2. Critical Success Factors for Lean initiation
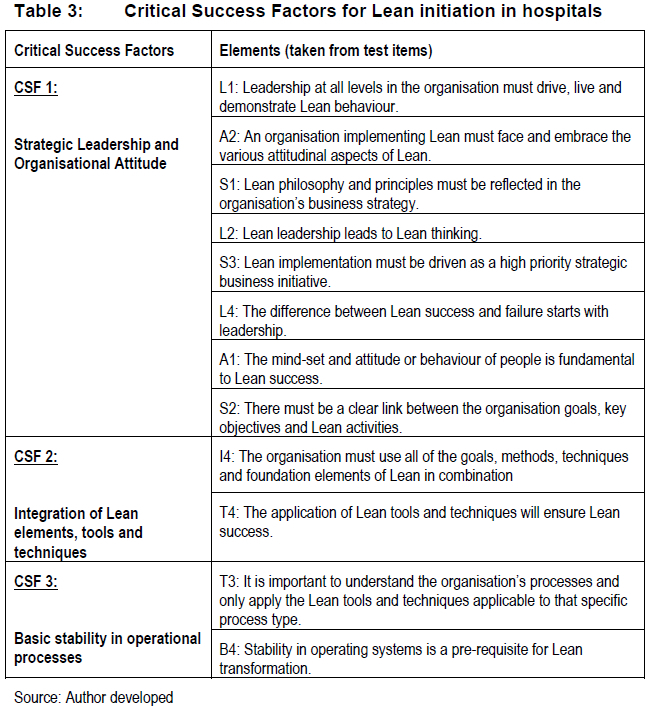
Critical Success Factors (CSF) is defined as "the limited number of areas in which results, if they are satisfactory, will ensure successful competitive performance for the organisation" (Rockart 1979:85). Three CSFs for the successful initiation of Lean in South African public hospitals have been identified. Each CSF consists of elements which itemise the factor (see Table 3). The elements of each factor provide a brief statement of the key requirements for healthcare managers to consider prior to the initiation of Lean in public hospitals, the absence of which may impede successful Lean rollout.
7. DISCUSSION
7.1 Development of the Lean SPRInT
The three CSFs identified through factor analysis and SEM are considered robust predictors of indicating success of Lean initiation in hospitals as all reliability and validity conditions have been met. The Lean SPRInT is a user-friendly success prediction instrument that can be used as a yardstick for healthcare managers to ascertain in advance the state of readiness of public hospitals for Lean initiation. It was developed from the three CSFs which have been integrated into an electronic tool. Lean SPRInT captures managers' inputs and produces readiness ratings and guidance processes for successful Lean initiation.
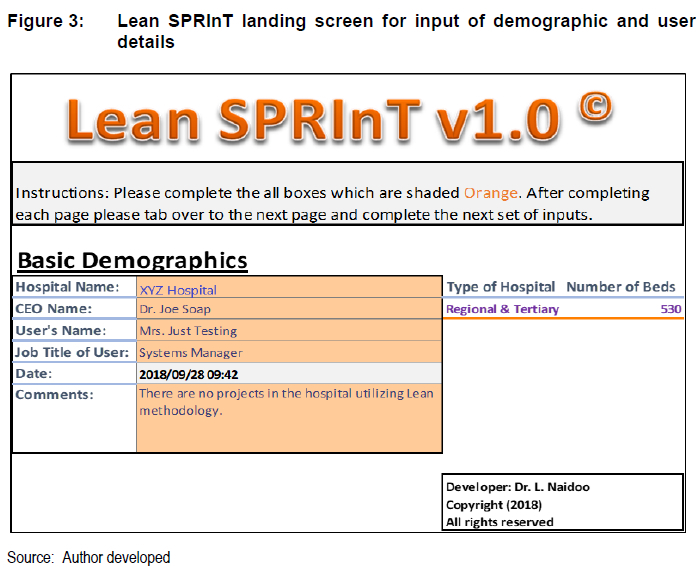
Lean SPRInT version 1.0 currently uses a Microsoft® Excel platform and user interface. Demographics and user details are captured on the landing screen (Figure 3). For public hospitals in KZN, there is a drop-down menu to select a hospital name from and the hospital classification and its number of beds is displayed automatically from a back-end database.
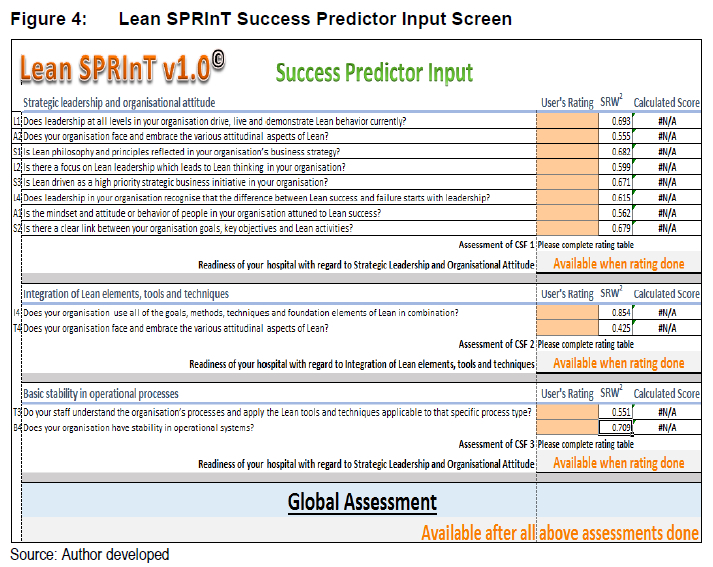
Thereafter the user switches over to the Lean success predictor input screen (Figure 4). Each CSF element formed the backbone of the Lean SPRInT success predictor input interface. The Lean success predictor input screen requires the user to select ratings from a drop-down menu, based on a Likert scale ("strongly agree"=4, "agree"=3, "disagree"=2 and "strongly disagree"=1), for each element as an indication of their degree of existence or applicability to their organisation's current environment in terms of Lean readiness. See Figure 3 for Lean SPRInT landing screen for input of demographic and user details.
See Figure 4 for Lean SPRInT success predictor input screen.
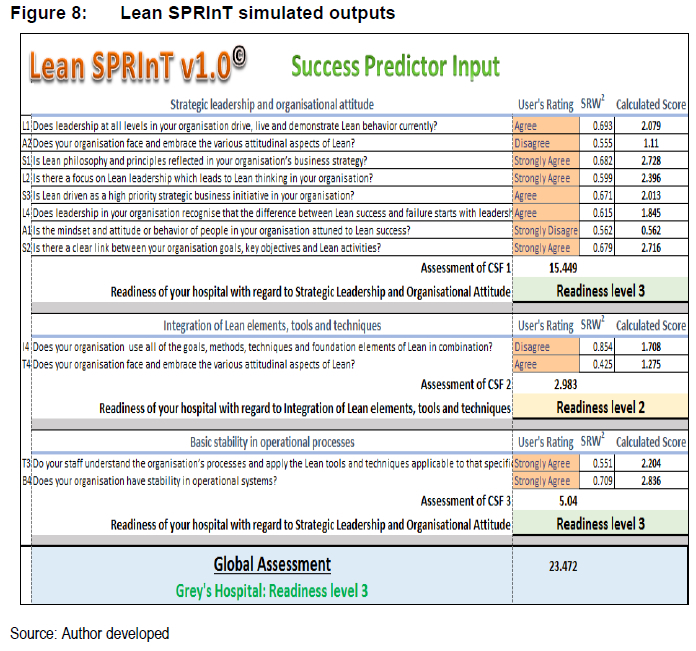
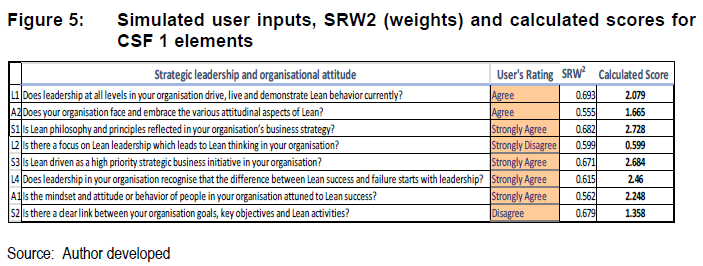
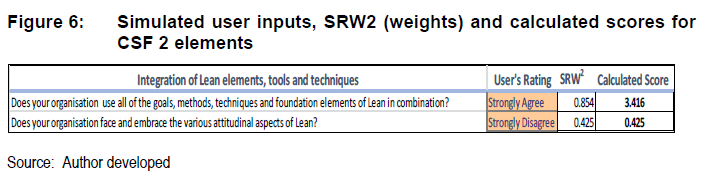
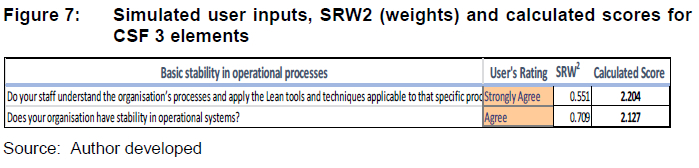
At the back end of Lean SPRInT, the Squared Multiple Correlations (communalities) or squares of the Standardised Regression Weights (SRW2) are used as weights for each of the elements in the input interface. These weights together with the users input ratings (1 to 4) generate products (calculated scores) for each element, i.e. user rating x SRW2. Figure 5, Figure 6 and Figure 7 show examples of simulated user inputs, SRW2 (weights) and calculated scores for CSF 1, CSF 2 and CSF 3 elements respectively.
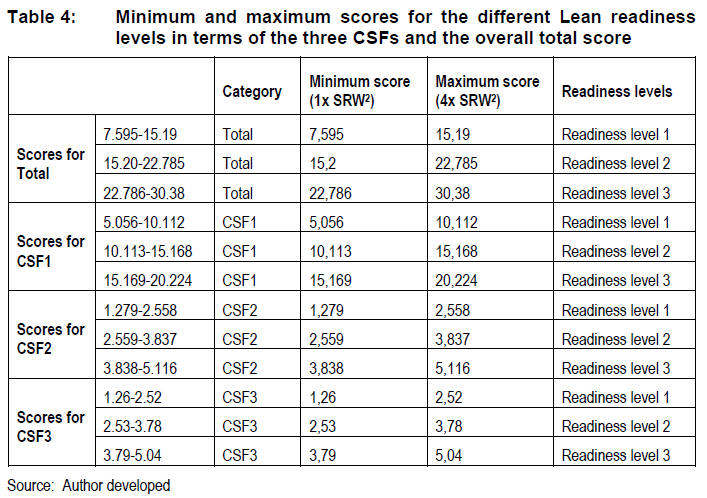
The maximum calculated score for each element is the product of 4 (maximum possible user rating) and the SRW2 for that element, whereas the minimum calculated score is the product of 1 (minimum possible user rating) and the SRW2 for that element. The sum of the maximum calculated scores for the elements of a particular CSF provides the maximum calculated score for that CSF. Likewise, the sum of the minimum calculated scores for the elements of a particular CSF provides the minimum calculated score for that CSF.
The overall range of scores for a CSF is divided equally into three sub-categories or tripartite ranges which correlate with a particular Lean readiness level (1, 2 or 3) for that CSF. The Lean readiness level for a CSF is then determined by placing the total calculated score for a particular CSF within one of the tripartite ranges for that CSF (Table 4). The overall range of scores for the final prediction of Lean readiness for the organisation is also divided equally into three subcategories (Table 4) which correlate with an organisational Lean readiness level (1, 2 or 3).
Lean SPRInT's output screen (Figure 8) with calculated Lean readiness levels, ranging from 1 to 3 (most unfavourable to most favourable prediction of readiness, respectively), is supplemented by commentary and recommendations to the user. These recommendations succinctly provide managers with a practical conduit to deploy resources without having to embark on the Lean journey blindly. This ensures that the ultimate aim of Lean SPRInT to determine upfront the state of Lean readiness is met by managers capturing inputs and the tool producing readiness ratings and recommendations for successful Lean initiation.
The culmination of the research in a tool that is both user-friendly and simple to use by healthcare managers wanting to introduce Lean in their institutions augurs well for the Lean body of knowledge.
7.2 Rollout of the Lean SPRInT
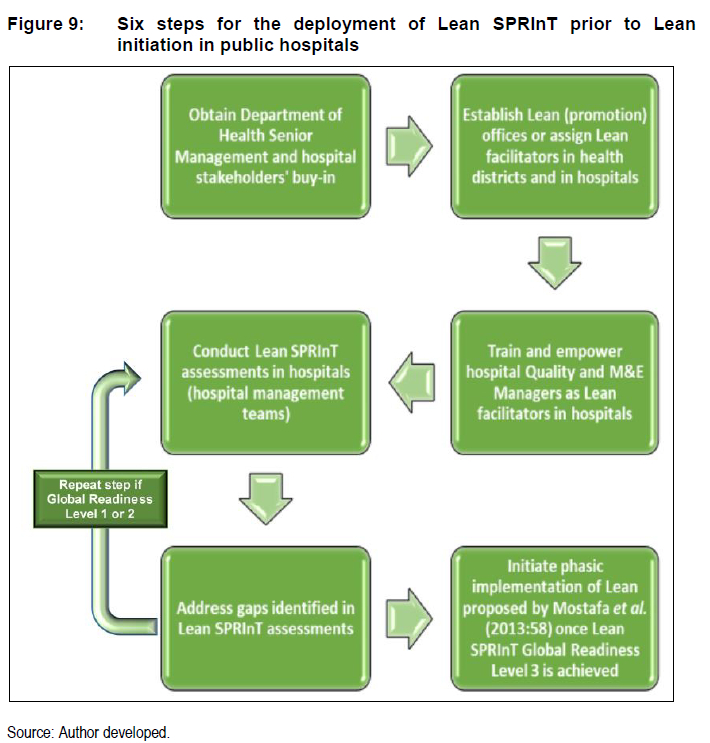
It is envisaged that Lean SPRInT could be adopted by the South African Department of Health, starting with the provincial hospitals in KZN, to assess the state of readiness for Lean initiation. The proposed 6 steps for the deployment of Lean SPRInT prior to the initiation of Lean in public hospitals are represented in Figure 9.
The foremost step involves obtaining buy-in from the KZN Head of Health and top management, and subsequently meeting with the district and hospital managers to introduce the tool and its purpose.
As the second step, the possibility of allocating a Lean (promotion) office as a Lean "helpdesk" in every health district should be considered. This office would be responsible for guiding hospitals within their jurisdiction with the use of Lean SPRInT. This office must place focus on "how to stay" rather than "how to be" Lean in order to avoid hospitals returning to their previous comfort zones after Lean rollout (Freitas, Freitas, Gomes de Menezes & Odorczyk 2018; Machado Guimarães & Crespo de Carvalho 2014:7). Lean (promotion) offices in health districts can be a shared resource for hospitals rolling out Lean and could be incorporated into existing district Monitoring and Evaluation (M&E) Management or Quality Management offices (Freitas et al. 2018; Goehnera, Mello & Bandeira 2016:39).
The third step is training of key staff, such as Quality and M&E Managers at hospital level, on the Lean SPRInT. This is a crucial step as it supports the maintenance and promotion of Lean at the coalface. According to the World Health Organisation (2007), "good leadership and management are about providing direction to, and gaining commitment from, partners and staff, facilitating change and achieving better health services through efficient, creative and responsible deployment of people and other health resources" (Doherty 2013:7; World Health Organisation 2007:1). Doherty (2013:9) cites the theory of "street-level bureaucrats", who, in health facilities, are the front-line workers such as doctors and nurses with direct patient and family contact, and make decisions on a daily basis at the 'coalface' on resource deployment and healthcare options which affects the performance of the institution. The degree of clinical leadership demonstrated in these "street-level bureaucrats" inevitably influences the operational efficiency at which the organisation performs.
Considering the above, training on the deployment of Lean SPRInT must target key stakeholders from hospitals, including Quality and M&E Managers and frontline clinician leaders. Hospital Quality or M&E Managers could be assigned as Lean facilitators within the hospitals. The training could include serial workshops on the functional and technical aspects of Lean SPRInT, interpretation of the outputs of Lean SPRInT and the possible options to consider as next steps for achieving Lean readiness. Lean experts from the Lean Institute of Africa could be invited to facilitate these workshops jointly with the developer of Lean SPRInT.
The fourth step is the actual application of the Lean SPRInT. It is proposed that the tool be completed by a joint sitting of top management of the hospital. It is imperative that the key managers assign, through consensus, ratings for each of the CSF elements in the tool. In step 5, gaps identified in terms of not meeting the CSF criteria for readiness of Lean initiation must be addressed, preferably through a formal action plan with activities and responsible persons for carrying out these activities with strict timeframes. The Lean SPRInT must then be applied iteratively and periodically in a follow up sitting of top management to assess progress made in addressing the initial gaps identified. Only once a Global Readiness Level of 3 is achieved should the initiation of Lean be considered (Step 6).
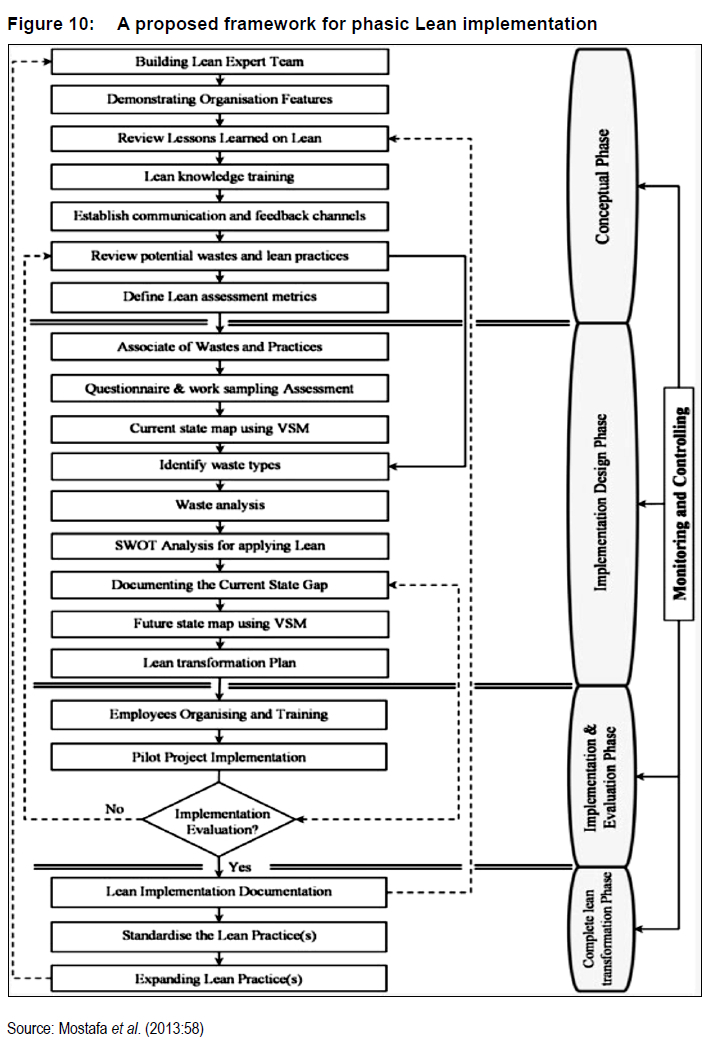
It is posited that implementation frameworks have highest success rates for Lean initiation (Mostafa, Dumrak & Soltan 2013:60). Although the output of Lean SPRInT doesn't consider sequenced Lean implementation, it is advisable that a phasic approach for Lean initiation is followed in Step 6 (Mostafa et al. 2013:54-60). A useful model is depicted in Figure 10, where Lean implementation commences with a Conceptual Phase, then moves to an Implementation Design Phase, an Implementation and Evaluation Phase, and finally a Complete Lean Transformation Phase.
It has been suggested that unified efforts of clinical and non-clinical services in healthcare facilities, decentralised clinical and managerial decision-making and culture transformation are more likely to lead to better outcomes (Doherty 2013:35). Lean fosters these characteristics, and if effectively inculcated in and practised by leaders at all levels within healthcare institutions, it is likely to lead to improvement in operational efficiency, thus narrowing the strategy intervention-implementation gap depicted in Figure 2.
See Figure 10 for the proposed framework for phasic Lean implementation.
7.3 Monitoring the implementation of Lean
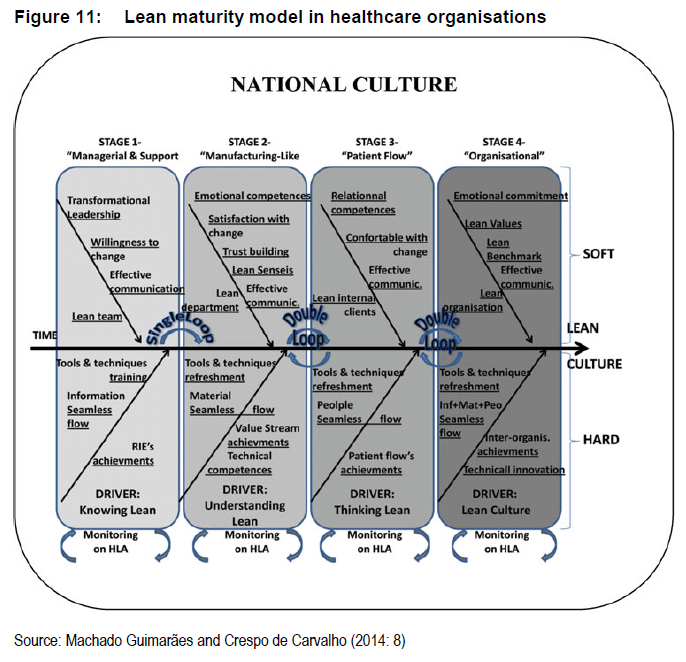
The success of Lean implementation is also determined by its monitoring and controls to prevent slippage. Lean SPRInT is not a monitoring tool, as it does not assess the degree of improvements made nor the pitfalls during Lean implementation. The Healthcare Lean Assessment tool (HLA) has been proposed as a useful monitoring instrument for providing a current-state diagnosis of the implementation process along the different Lean maturity levels thus guiding the Lean journey (Machado Guimaräes & Crespo de Carvalho 2014:1521). As Lean transformation matures from Lean initiation, with intertwining training on soft (human aspects) and hard skills (Lean tools and techniques), the hospital would proceed through four stages as depicted in Figure 11. Lean SPRInT would precede Stage 1.
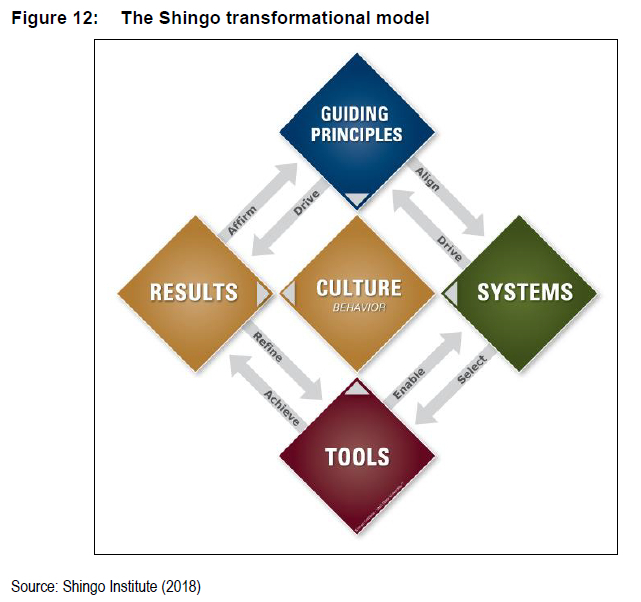
The HLA tool is based on the Shingo transformational model known as the Shingo diamond (Figure 12), which reinforces a systematic approach to ongoing improvement (Machado Guimaräes & Crespo de Carvalho 2014:14). The Shingo diamond demonstrates the interrelationship amongst guiding principles, systems, tools and results, all of which effectively influence the culture of the organisation. The HLA tool assesses whether each process in the maturity model (Figure 11) should be improved disrupted or eliminated and can be used as an ongoing implementation assessment, providing control measures and corrective actions.
8. MANAGEMENT IMPLICATIONS
Lean SPRInT's output of calculated Lean readiness levels for each of the CSF elements allow managers to gauge the deficiencies in their institution, which once improved, would portend for a more favourable prediction of success. Lean SPRInT as a success predictor instrument is by no means the panacea for Lean implementation in hospitals, but prepares managers embarking on a Lean journey by providing them with a current-state assessment of their organisation in terms of the elements of the 3 CSFs. The use of Lean SPRInT should be integrated in a phasic Lean implementation framework such that the assessment outputs will facilitate appropriate resource deployment as the Lean journey progress from one phase to the next.
9. AREAS FOR FUTURE RESEARCH
Future research to evaluate the effectiveness and practicality of Lean SPRInT is recommended. Research on the utilization or uptake of Lean SPRInT in public hospitals, and correlation of the findings with the successful initiation of Lean will be very useful to determine the value of the tool. A survey on the attitudes and perceptions of senior managers with regard to Lean SPRInT will provide useful information for the developer to consider in refining the tool.
10. LIMITATIONS OF THE STUDY
The researcher experienced difficulty in reaching the target population and delayed response times due to the geographical spread of the public hospitals, some with information technology and network difficulties. There were also some management posts that were vacant with the high staff turnover rate, often with people erratically acting in those positions. Most of these limitations were addressed by close follow up with the local health district offices and district quality and information managers, which support respective hospitals. A research assistant was also used to distribute and collect questionnaires, and follow up responses from participants.
11. CONCLUSIONS
The organisational strategy roadmap is guided by strategic vision and goals and is often laden with barriers and enablers which widen or narrow the intervention-implementation gap, respectively. Lean is both a catalyst for interventions and an intervention itself which maximises output with minimal resource inputs by "doing better with less" (Omogbai & Salonitis 2016:106; R0vik & Andersen 2015:1; Womack et al. 2007:1). The Lean SPRInT is proposed as a management tool for assessing hospitals' readiness status for Lean initiation prior to embarking on a Lean transformation journey.
Lean SPRInT utilizes a scoring system for assessing the degree of readiness for Lean initiation in accordance with three critical success factors (CSFs): (1) Strategic leadership and organisational attitude; (2) Integration of Lean elements, tools and techniques, and (3) Basic stability in operational processes. The culmination of this study in a tool that is both user-friendly and simple to use by managers wanting to initiate Lean in their hospitals augurs well for the Lean body of knowledge.
A six-step process for the deployment of Lean SPRInT in public hospitals is proposed in this article. Top management buy-in precedes the establishment of Lean promotion offices and/or facilitators using existing resources such as Quality and M&E Managers as shared resources within health districts. Empowerment of these officials through training is essential. Lean SPRInT assessments of hospitals must be carried out by hospital management teams, facilitated by Quality and M&E Managers, and identified gaps addressed through a structured approach. Lean SPRInT assessments and addressing shortfalls are repeated in an iterative process until the tool predicts a Global Readiness Level of 1, heralding the readiness to proceed with Lean initiation. A phasic approach for Lean implementation, together with close monitoring to prevent slippage using the HLA tool is recommended.
It is suggested that unified efforts of clinical and non-clinical services in healthcare facilities, decentralised clinical and managerial decision-making and culture transformation are more likely to lead to better outcomes of Lean initiation (Doherty 2013:35). Such an approach is likely to sustainably improve operational efficiency and narrow the strategic interventionimplementation gap for successfully achieving targeted health outcomes.
COMPETING INTERESTS
None.
AUTHORS' CONTRIBUTIONS
Logandran Naidoo conducted the research and produced the report. Ziska Fields supervised the research.
ACKNOWLEDGEMENTS
The authors wish to express their heartfelt gratitude to the managers and supervisors at the KZN Department of Health for their participation and for permitting the study to take place. The assistance received from Dr. Zane Farina in the basic development of Lean SPRInT is highly appreciated. The authors also wish to thank Dr Danie Vermaak for granting permission to use his data collection questionnaire elements in the formulation of the data collection tool for this study.
REFERENCES
BECK K, BEEDLE M, BENNEKUM A, COCKBURN A, CUNNINGHAM W, FOWLER M, GRENNING J, HIGHSMITH J, HUNT A, JEFFRIES R, KERN J, MARICK B, MARTIN R, MELLOR S, SCHWABER K, SUTHERLAND J & THOMAS D. 2001. Manifesto for Agile Software Development. Corryton: Agile Alliance. [Internet:http://www.agilemanifesto.org/; downloaded on 03 July 2019. [ Links ]]
BURGESS N & RADNOR Z. 2013. Evaluating Lean in healthcare. International Journal of Health Care Quality Assurance 26:220-235. [ Links ]
BUJANG MA, OMAR ED & BAHARUM NA. 2018. A Review on Sample Size Determination for Cronbach's Alpha Test: A Simple Guide for Researchers. The Malaysian Journal of Medical Sciences : MJMS 25(6):85-99. [Internet:https://www.ncbi.nlm.nih.gov/pubmed/30914882; downloaded on 28 April 2019]. (DOI:10.21315/mjms2018.25.6.9. [ Links ])
DICKSON EW, SINGH S, CHEUNG DS, WYATT CC & NUGENT AS. 2009. Application of lean manufacturing techniques in the emergency department. Journal of emergency medicine 37:177-182. [ Links ]
DOHERTY J. 2013. Strengthening clinical leadership in hospitals: A review of the international and South African literature. Johannesburg: The Municipal Services Project, School of Government, University of the Western Cape. [ Links ]
FAITH M, KIM N & HEO M. 2015. Statistical power as a function of Cronbach alpha of instrument questionnaire items. BMC Medical Research Methodology 15(1):1-9. (DOI:10.1186/s12874-015-0070-6. [ Links ])
FREITAS RDC, FREITAS MDCD, GOMES DE MENEZES G & ODORCZYK RS. 2018. Lean Office contributions for organizational learning. Journal of Organizational Change Management 31(5):1027-1039. (DOI:10.1108/JOCM-06-2017-0221. [ Links ])
GOEHNERA L, MELLO LCBB & BANDEIRA RAM. 2016. Lean Manufacturing Implementation for Multinational Companies with Production Subsidiary in Brazil: Development of A Roadmap. International Journal of Lean Thinking 7(1):26-46. [ Links ]
IMPROTA G, ROMANO M, DI CICCO MV, FERRARO A, BORRELLI A, VERDOLIVA C & CESARELLI M. 2018. Lean thinking to improve emergency department throughput at AORN Cardarelli hospital. BMC Health Services Research 18(1):1-9. (DOI:10.1186/s12913-018-3654-0. [ Links ])
JHA RK, SAHAY BS & CHARAN P. 2016. Healthcare operations management: a structured literature review. DECISION 43:259-279. [ Links ]
KUNDU G & MANOHAR BM. 2012. Critical success factors for implementing lean practices in I.T. support services. International Journal for Quality research 6:301 -312. [ Links ]
KZN DEPARTMENT OF HEALTH. 2018a. KwaZulu-Natal Department of Health Annual Report 2017/18 - Vote 7. Pietermaritzburg: KZN Department of Health. [ Links ]
KZN DEPARTMENT OF HEALTH. 2018b. KwaZulu-Natal Department of Health Annual Performance Plan 2018/19 - 2020/21. Pietermaritzburg: KZN Department of Health. [ Links ]
KYRIAZOS TA. 2018. Applied Psychometrics: Sample Size and Sample Power Considerations in Factor Analysis (EFA, CFA) and SEM in General. Psychology 09:2207-2230. [ Links ]
MACCALLUM RC, WIDAMAN KF, ZHANG S & HONG S. 1999. Sample size in factor analysis. Psychological Methods 4(1):84-99. [ Links ]
MACHADO GUIMARÃES C & CRESPO DE CARVALHO J. 2014. Assessing Lean Deployment in Healthcare-A Critical Review and Framework. Journal of Enterprise Transformation 4(1):3-27. [Internet:https://doi.org/10.1080/19488289.2013.869277; downloaded on 24 March 2019]. (DOI:10.1080/19488289.2013.869277. [ Links ])
MADUBULA N, ENGLISH RG, PADAYACHEE T & MKHIZE M. 2014. Adequacy and Efficiency in Primary Health Care Financing. Technical Report: Submission for the Division of Revenue 2015/2016. Midrand: Financial and Fiscal Commission. [ Links ]
MAYOSI BM & BENATAR SR. 2014. Health and Healthcare in South Africa - 20 Years after Mandela. New England Journal of Medicine 371(14):1344-1353. [Internet:http://www.nejm.org/doi/full/10.1056/NEJMsr1405012; downloaded on 14 March 2019]. (DOI:doi:10.1056/NEJMsr1405012. [ Links ])
MOSTAFA S, DUMRAK J & SOLTAN H. 2013. A framework for lean manufacturing implementation. Production & Manufacturing Research 1(1):44-64. [Internet:http://dx.doi.org/10.1080/21693277.2013.862159; downloaded on 28 February 2019]. (DOI:10.1080/21693277.2013.862159. [ Links ])
OMOGBAI O & SALONITIS K. 2016. A Lean Assessment Tool Based on Systems Dynamics. Procedia CIRP 50:106-111. [Internet:http://www.sciencedirect.com/science/article/pii/S2212827116304097; downloaded on 19 August 2018]. (DOI:https://doi.org/10.1016/j.procir.2016.04.169. [ Links ])
REDDY A. 2016. The Scrumban [r]evolution: Getting the most out of Agile, Scrum and Lean kanban. New York City: Pearson Education Inc. [ Links ]
ROCKART JF. 1979. Chief executives define their own data needs. Harvard Business Review 57(2):81-93. (March-April. [ Links ])
R0VIK K & ANDERSEN H. 2015. Lost in translation: a case-study of the travel of lean thinking in a hospital. BMC Health Services Research 15(1):1-9. (DOI:10.1186/s12913-015-1081-z. [ Links ])
SCHUMACKER RE & LOMAX RG. 2015. A Beginner's Guide to Structural Equation Modeling. 4th ed. New York: Routledge. [ Links ]
SHINGO INSTITUTE. 2018. The Shingo model. [Internet:https://shingo.org/model; downloaded on 24 March 2019. [ Links ]]
SRINIVASARAGHAVAN J & ALLADA V. 2006. Application of mahalanobis distance as a lean assessment metric. Int J Adv Manuf Technol The International Journal of Advanced Manufacturing Technology 29:11591168. [ Links ]
SUTHERLAND J & SCHWABER K. 2013. The Scrum Guide: The Definitive Guide to Scrum: The Rules of the Game. Boston: Scrum.org. [ Links ]
TABER KS. 2018. The Use of Cronbach's Alpha When Developing and Reporting Research Instruments in Science Education. Research in Science Education 48(6):1273-1296. [Internet:https://doi.org/10.1007/s11165-016-9602-2; downloaded on 28 April 2019]. (DOI:10.1007/s11165-016-9602-2. [ Links ])
WOMACK JP, JONES DT & ROOS D. 2007. The machine that changed the world. New York: Simon & Schuster. [ Links ]
WORLD HEALTH ORGANISATION. 2007. Building leadership and management capacity in health. Geneva: World Health Organisation. [ Links ]
YIP W & HAFEZ R. 2015. Reforms for improving the efficiency of health systems: lessons from 10 country cases. Geneva: WHO Press. [ Links ]
ZIDEL TG. 2006. A lean toolbox-using lean principles and techniques in healthcare. Journal for Healthcare Quality 28:W1-7. [ Links ]
* corresponding author

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}