










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671Print version ISSN 1994-3032
S. Afr. j. child health vol.19 n.1 Pretoria Mar. 2025
https://doi.org/10.7196/SAJCH.2025.v19i1.2637
RESEARCH
Diagnostic utility of lung ultrasound in preterm neonates with respiratory distress at a tertiary neonatal intensive care unit in South Africa
F Mpisane-JamaI; W BaseraII; A R HornIII
IMPhil (Neonatology); Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
IIPhD; School of Public Health, Faculty of Health Sciences, University of Cape Town, South Africa
IIIPhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: Accumulating data suggest the potential for lung ultrasound (LUS) to diagnose pathology in preterm babies, but there are no published data from South Africa (SA
OBJECTIVES: To describe LUS diagnoses, respiratory pathology and outcomes in preterm babies receiving non-invasive respiratory support in a tertiary SA neonatal unit, and to compare LUS with clinical diagnoses and surfactant administration
METHODS: We conducted a prospective, observational study of babies at 27 - 34 weeks' gestation, with birthweight >800 g, receiving non-invasive respiratory support and who had LUS at age <3 hours. Surfactant was administered at a fraction of inspired oxygen (FiO2) of 0.35 - 0.45 and was not influenced by LUS findings
RESULTS: Fifty-one neonates were included, of whom 16% received surfactant, all with respiratory distress syndrome (RDS) as their only clinical diagnosis, compared with multiple diagnoses in the non-surfactant group, including RDS (93%), transient tachypnoea of the newborn (TTN) (16%) and pneumonia (14%). Lung ultrasound indicated less RDS in the non-surfactant group than the surfactant group (42% v. 88%; p=0.02), and more TTN (61% v. 13%; p=0.01). The LUS score (LUSS) predicted surfactant administration (area under the curve 0.8 (95% confidence interval 0.67 - 0.94)). A LUSS of 7 had the best combined sensitivity (75%) and specificity (72%) but a low positive-predictive value (33%). A LUSS of 8 identified 8 (19%; n=8/43) additional babies for surfactant who did not need treatment
CONCLUSION: LUS suggested more diagnoses than clinical assessment, particularly TTN, but did not accurately predict surfactant administration at an FiO2 of 0.35 - 0.45
Keywords: neonate; newborn; neonatal intensive care; point-of-care ultrasound; lung ultrasound; respiratory distress syndrome; surfactant
Respiratory distress syndrome (RDS) is a major cause of death among preterm neonates, with a mortality rate in low-income countries ~10-fold higher than in high-income countries. [1,2] Meta-analyses from over 10 years ago show reduced neonatal mortality, and chronic lung disease when surfactant is administered early to intubated neonates.[3] More recently, optimal management to reduce bronchopulmonary dysplasia (BPD) and death includes early surfactant administration to neonates receiving nasal continuous positive airway pressure (nCPAP).[1]
The severity of RDS may be indicated by inspired oxygen (FiO2) requirements. While X-rays convey useful information, they are not routinely performed owing to associated delays, radiation exposure and resource implications.[4] Lung ultrasound (LUS) is a quick and radiation-free bedside tool with the potential to diagnose RDS, transient tachypnoea of the newborn (TTN), meconium aspiration syndrome, pneumothorax and pneumonia.[5-7] Mounting evidence suggests a role for LUS to predict surfactant requirement.[7-9] Brat et al.[8] described a LUS score (LUSS) which correlated well with oxygenation status and predicted surfactant treatment; a LUSS >4 was associated with increased surfactant treatment of neonates with a gestational age (GA) <34 weeks, from 25% to 75%. A prospective cohort study showed LUS scores >6 and >8 had sensitivities and specificities of 90% and 80% v. 82% and 92%, respectively, for predicting surfactant treatment.[7] A more recent randomised controlled trial (RCT) comparing a LUSS >8 within the first 3 hours of life with FiO2 threshold of 0.3 - 0.4 as indications for surfactant, showed that the LUSS indicator was associated with earlier treatment at lower FiO2.[9]
At the time of writing the present manuscript, there were no published data or guidelines on the use of neonatal LUS in South Africa (SA) - LUS was used at the discretion of the senior clinician in Groote Schuur Hospital (GSH) neonatal intensive care unit (NICU) and high care unit (HCU), often in the first 3 hours, similar to other centres.[10,11] The primary objective of the present study was to evaluate the use of LUS in diagnosing respiratory pathology among surfactant-naïve preterm neonates treated with nCPAP, or high-flow humidified nasal canula (HFHNC) in a public, tertiary neonatal unit in SA. The secondary objective was to explore the association between LUS findings and surfactant administration in this population.
Methods
Study design and population
We carried out an exploratory, prospective, observational cohort study of preterm neonates admitted to the GSH NICU and HCU during a 4-month convenience period based on feasibility of data collection, anticipating recruitment of ~50 neonates. The GSH neonatal unit has ~2 000 admissions per annum and is the major tertiary referral centre for the Metro West Area of Cape Town.
The study conformed to the principles of the 2013 Declaration of Helsinki and was approved by the University of Cape Town Health Sciences Faculty of Health Sciences Human Research Ethics Committee (ref. no. 335/2022) and GSH management.
The inclusion criteria identified preterm neonates with suspected RDS, who were eligible for intubation and surfactant administration by provincial guidelines: inborn neonates; 27 - 34 weeks' GA at birth; birthweight >800 g; respiratory support at recruitment with nCPAP or HFHNC; and LUS at age <3 hours. Neonates with the following exclusion criteria were not recruited: received surfactant or intubated before LUS; or congenital/chromosomal abnormalities.
Standard care and gestational age assessment
Clinical management was according to GSH protocols, irrespective of recruitment. Gestational age was assigned based on early obstetric ultrasound scan (EUS) if performed <20 weeks GA. In the absence of EUS, the Ballard score was used if birthweight was >1 000 g,[12] and foot length measured with Vernier callipers was used when birthweight was <1 000 g.[13] Infants with infection risk factors were managed according to the 2021 National Institute for Health and Care Excellence (NICE) guidelines.[14] If antibiotics were commenced, they were stopped after 36 - 48 hours if blood cultures were negative and C-reactive protein (CRP) levels were <10 mg/L.
Respiratory management was based on the 2019 European guidelines.[1] Surfactant was not administered in the delivery room. Neonates with respiratory distress after birth and who did not require intubation were commenced on mask CPAP and transferred to nCPAP at 5 - 7 cm water. Oxygen saturation was monitored continuously and FiO2 adjusted to maintain pre-ductal saturation at 90 - 95%. If the FiO2 was persistently >0.35 - 0.45, Beractant was administered (100 mg/kg) via the less invasive surfactant administration (LISA) or intubation-surfactant-extubation (INSURE) methods.[1] A chest X-ray was not routinely performed prior to surfactant administration via LISA or INSURE. Repeat dosing was considered if FiO2 remained above 0.45 after 6 to 12 hours. Indications for intubation and mechanical ventilation were apnoea or respiratory acidosis with a pH <7.25 and/ or FiO2 >0.6 after surfactant.
Recruitment and informed consent
Participants were identified by daily review by a clinician (FM-J), of admissions, during normal attending hours from August to November 2022. After obtaining informed consent, the following data were entered into a case record form (CRF): maternal and infant demographic data; maternal medical and obstetric history; labour and delivery data; respiratory pathologies and major morbidities; treatment; LUS findings; and outcomes.
Lung ultrasound procedures
For the duration of the study, LUS was performed by a single clinician (FM-J), who had received training at an international congress on LUS in neonates and children in France. The LUS was performed using a Vivid-IQ (GE Healthcare, USA) with a wideband linear array probe (4 - 15 MHz) over anterior, lateral and posterior axillary areas per hemi-thorax.[8] De-identified images were exported to an external hard drive for later blinded assessment by ARH - only the blinded interpretation was used for analysis.
Ultrasonographic findings were described based on standard definitions: lung sliding, movement between lung and pleura; A-lines, artefacts resulting from pleural reflections; B-lines, artefacts from reflections of lung fluid; and pleural lines, echogenic lines formed by the chest wall and aerated lung interface. A LUSS was derived by allocating a score of 0 to 3 to each lung area: A-pattern (A-lines only), score = 0; B-pattern ( >3 well-spaced B-lines), score = 1; severe B-pattern (crowded and coalescent B-lines with or without consolidation confined to the subpleural space), score = 2; and extended consolidations, score = 3. A total score was calculated by adding the individual scores from each lung zone to a maximum score of 0 to 18.[8,15] The LUS findings were not used to influence the decision to administer surfactant.
The LUS was also assessed for features of TTN, pneumonia and pneumothorax, where each feature was assigned a point. Features of TTN included: a double lung point (two patterns in one view, including normal A-pattern/B-pattern or B/severe B pattern); a gradient of echogenicity between inferior and superior areas with lower echogenicity in superior areas, including areas with non-compact B-lines but no area with extended consolidation; or a LUSS of 1 to 6 with normal lung/non-compact B-lines.[6,16,17] Features of pneumonia included one or more of: absent lung sliding with B-lines in the same view; absent lung sliding with absent B-lines but lung pulse present and no lung point in same view; LUSS <6 with pleural line abnormalities (disappearance/irregularity/coarse) or any lung consolidation/air bronchograms; large (>1 cm) areas of lung consolidation with irregular margins without a B/severe B pattern.[18] Features of pneumothorax included the presence of a lung point -the transition between an area of lung sliding and absence of lung sliding and absent B-lines, or absent lung pulse without B-lines or lung pulse.[18,19] A LUS respiratory diagnosis was assigned and these data were entered into a separate LUS report form.
Data management
The data from the CRF and the LUS report form were de-identified and entered into a UCT hosted REDCap data base. A power calculation was not performed as our study was exploratory and descriptive. Stata Version 15 (Stata Corp., USA) was used for statistical analysis. Data were grouped according to surfactant treatment. The chi-square or Fisher's exact tests were used for categorical comparisons. Student's t-test or Wilcoxon-Mann-Whitney rank-sum tests were used for comparison of parametric and non-parametric continuous variables, respectively.
Receiver operating characteristic (ROC) analysis was used to evaluate the ability of the LUSS to predict surfactant administration; area under the curve (AUC) and cut-off values showing sensitivity, specificity, predictive values, and likelihood ratios (LR) were reported. A logistic regression model was used to predict the probability of surfactant administration. Statistical significance was denoted by a p-value <0.05.
Results
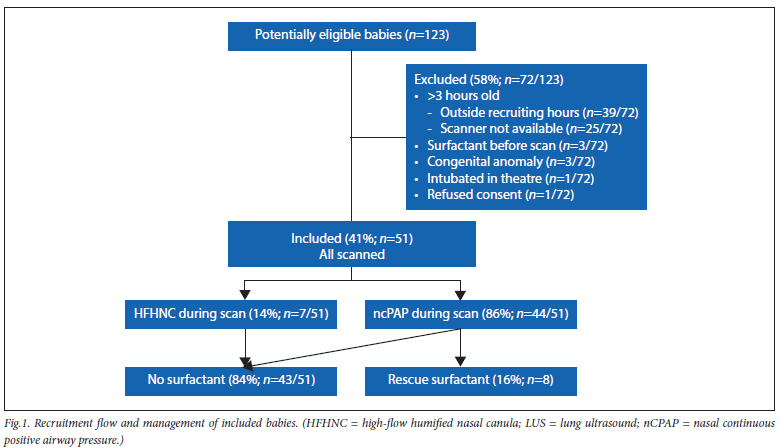
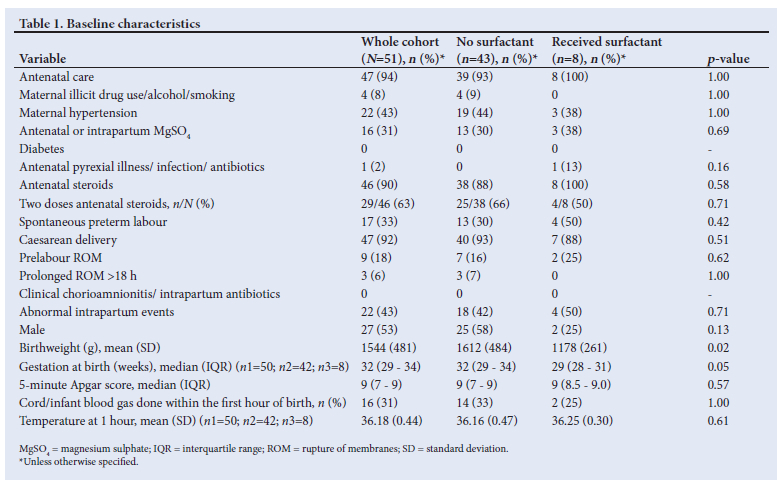
A total of 51 neonates were included and 8 (16%) received surfactant, all during nCPAP (Fig. 1). The baseline characteristics, grouped according to surfactant administration are shown in Table 1. Most of the mothers received antenatal care and antenatal steroids, and were delivered by caesarean section. Risk factors for infection were infrequent and no mother received intrapartum antibiotics. The birthweights and GA were lower in the surfactant group (median weight 1 178 g v. 1 612 g (p=0.02) and median GA 29 v. 32 weeks; p=0.05).
Respiratory pathologies and lung ultrasound
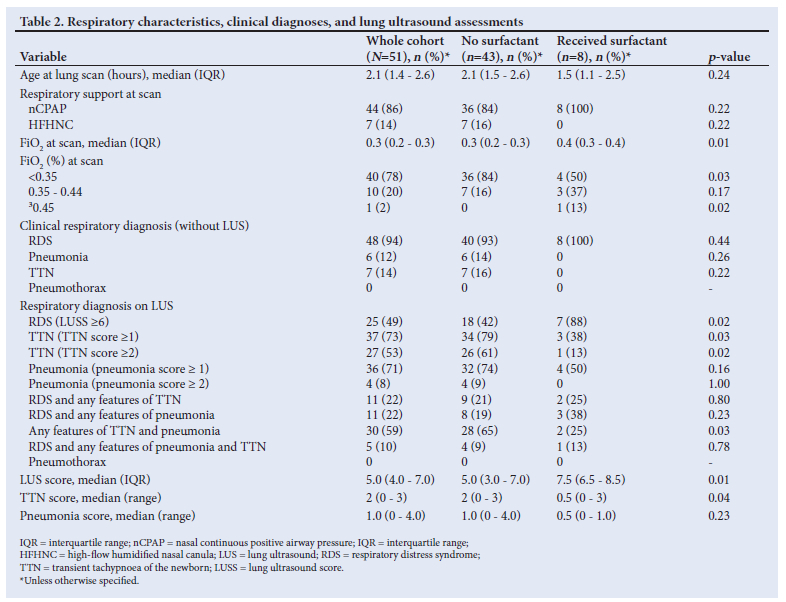
The respiratory characteristics and LUS features are shown in Table 2. There were no differences in respiratory support or age at LUS between treatment groups. However, all neonates who received surfactant were receiving nCPAP and none of the neonates on (HFHNC) required surfactant. At the time of LUS, the FiO2 was lower in the non-surfactant group (FiO2 <0.35 in 50% v. 84% of surfactant group; p=0.03). The FiO2 increased to 0.45 during LUS in one neonate who received surfactant immediately after LUS.
There were no differences in diagnoses between treatment groups without LUS; however, TTN and pneumonia were not diagnosed at all in the surfactant group, compared with 16% and 14%, respectively, in the non-surfactant group. In contrast, LUS indicated features of multiple overlapping diagnoses; more RDS in the surfactant group compared with the non-surfactant group (88% v. 42%; p=0.02) and less TTN, particularly in those with a TTN score >2 (13% v. 61%; p=0.02). The neonates who received surfactant had higher LUS scores (7.5 (1.6) v. 5.0 (2.4); p=0.01) and lower TTN scores (0.75 (1.16) v. 1.74 (1.16); p=0.03).
Comparison of clinical diagnoses compared with LUS in the whole cohort, showed more RDS (94% v. 49% with LUS; p<0.001), less TTN with score >1 (14% v.73%; p<0.001) or > 2 (14% v.53%; p<0.001), and less pneumonia with a score >1 (12% v. 71%; p<0.001), but no difference with a score >2.
Lung ultrasound score prediction model
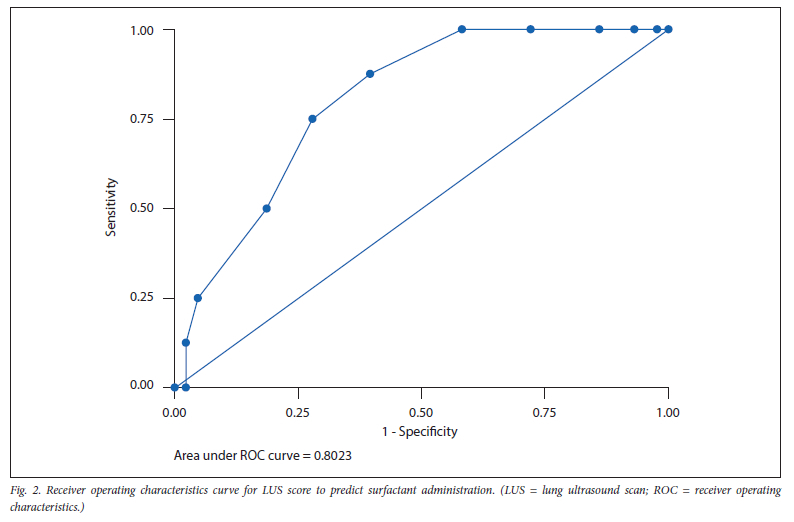
The receiver operating characteristic (ROC) curve for the LUSS to predict surfactant administration, is shown in Fig. 2. The area under the curve (AUC) was 0.8 (95% confidence interval (CI) 0.67 - 0.94) with adequate fit and acceptable discrimination (Hosmer and Lemeshow p=0.92). Logistic regression analysis showed that LUSS was a significant predictor of surfactant administration with increasing odds ratio (OR) of 1.68 (CI 1.10 - 2.57), for every 1-unit increase in LUSS (p=0.02).
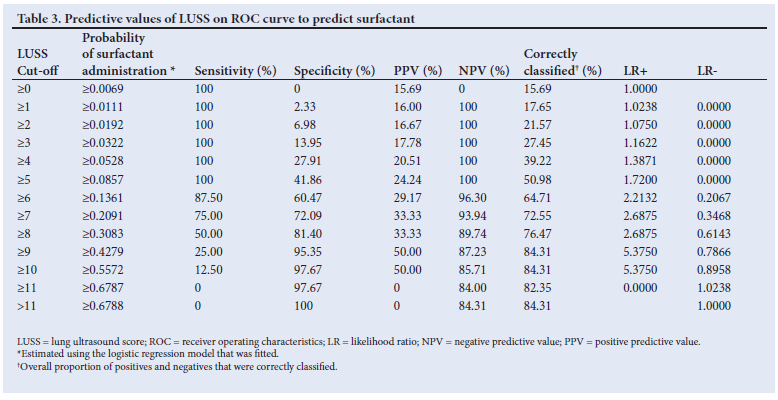
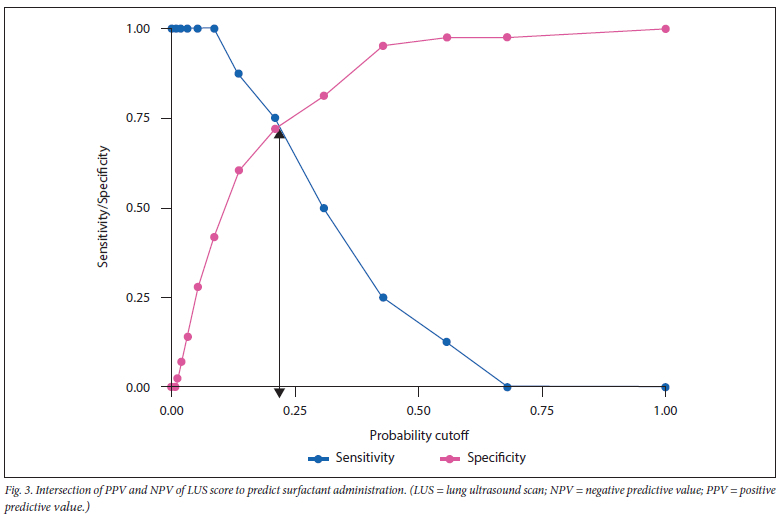
The predictive values of LUS scores are shown in Table 3. A LUSS >6 had a high negative-predictive value (NPV) (96%), but only 14% probability of surfactant administration. The LUSS giving the most correct classification (73%) with the highest sensitivity (75%) was LUSS >7, which coincided with the probability cut-off of 21% at the intersection of positive predictive value (PPV) and NPV (Fig. 3). However, at this value the PPV (33%) and specificity (72%) were low. A LUSS >10 had high specificity (98%), correct classification (84%) and a positive LR (5.4), but its sensitivity (13%) was very low.
Morbidity and mortality
The mean maximum FiO2 and the duration of respiratory support during the first week were higher (0.57 (0.2) v. 0.29 (0.06); p=0.01) and longer (median (IQR) days 8 (4.5 - 13) v. 3 (2 - 6); p=0.01) in the surfactant group. The surfactant group had higher maximum CRP levels (median mg/L (IQR): 10 (1 - 39) v. 1 (1 - 2); p=0.02), more necrotising enterocolitis (NEC) (25% v. 0; p=0.01); and more blood transfusions (38% v. 2%; p=0.01). No neonates were treated with inotropes, had early infection, or had severe periventricular intracranial haemorrhage or periventricular leukomalacia. One neonate developed BPD. One death was recorded in the non-surfactant group and was due to septicaemia.
Discussion
The present study of early LUS in surfactant-naïve neonates at 27 - 34 weeks' GA, during non-invasive ventilation, found that a wider range of diagnoses were suggested by LUS compared with clinical assessment. A LUSS of 7 predicted surfactant administration, but with a low PPV and only 16% required surfactant.
A LUSS of 8 was proposed by De Martino et al.;[7] their score of 8 had higher predictive values (82% sensitivity, 92% specificity and 92% PPV) than our score of 7; however, their cohort only included neonates <30 weeks' GA, and their threshold FiO2 for surfactant administration was lower at >0.3 or >0.4 for neonates <28 and >28 weeks' GA, respectively. A RCT including neonates <32 weeks' GA, comparing a LUSS of 8 with the same FiO2 thresholds for surfactant administration used by De Martino et al., [7] showed that the LUSS of 8 was associated with earlier treatment than FiO2 thresholds (1 hour v. 6 hours; p<0.001), at lower FiO2 (0.25 v. 0.3; p=0.016) and increased SpO2/FiO2 ratio after treatment.[9] Both these studies had lower GA inclusion limits and lower FiO2 administration thresholds than our study, and both were conducted in high-income countries. In contrast to their findings, the LUSS of 8 in our study had lower sensitivity (50%) and PPV (33%); although the specificity was high (81%), the use of this score would have indicated surfactant treatment in 8 (19%) additional neonates, none of whom ultimately required or received surfactant.
Our findings differ from a recent observational study in India.[20] Singh et al.[20] enrolled 100 neonates <34 weeks GA, similar to our study, but with lower FiO2 at the time of surfactant administration, of 0.3 - more neonates received surfactant (40% v. 16%), and the age at LUS was earlier than our study (mean 1.37 hours in their study v. median 2.1 hours in our study). The LUSS of 7 was the best predictor of surfactant administration in their study, but with higher predictive values (sensitivity 92.5%, specificity 96.7%, and PPV 94.9%) than in our study.
The benefit of LUS in identifying alternative diagnoses to RDS and the high concordance with X-ray and interobserver agreement is well described.[10,11] Our study demonstrated that LUS more frequently indicated diagnoses other than RDS compared with clinical assessment alone, particularly in the non-surfactant group. Individual LUS diagnostic features for both TTN and neonatal pneumonia are established, but predictive values of individual and collective features vary between studies, and overlap between the LUS features.[21] While several studies show high diagnostic sensitivity and specificity of LUS features of TTN, these studies frequently included term and/ or near-term neonates, late presentations, ventilated neonates and/ or asymptomatic controls.[22] In order to address the overlap of features, we developed TTN and pneumonia scores. The TTN score of >2, in 61% of neonates in the non-surfactant group compared with 13% of the surfactant group (p=0.02), was in keeping with their benign clinical course (median 3 days respiratory support, with no intubation). The high frequency of LUS pneumonia score >1 (74%), compared with clinical diagnosis of pneumonia in 14%, and the low frequency of sepsis indicators (<16% pre-labour/prolonged ruptured membranes, no chorioamnionitis, no intrapartum antibiotics, and median highest CRP 1 mg/L), in the non-surfactant group, suggests the LUS pneumonia score >2 may be a more appropriate indicator of pneumonia, than a score >1. Liu et al.[23] reported that a large area of lung consolidation with irregular margins on LUS, had 100% sensitivity and specificity for neonatal pneumonia. However, their study was based on a non-consecutive convenience sample of neonates with suspected pneumonia, compared with a control group admitted for non-pulmonary reasons. Our sample was not designed to establish diagnostic criteria for pneumonia, as it contained a group at low risk; however, the high frequency of LUS features of pneumonia in our setting where pulmonary infection was unlikely, indicates the need for caution when interpreting LUS findings.
The increased morbidity in the surfactant-treated group in our study may be related to lower birthweights and lower GA. Early surfactant administration is associated with decreased morbidity in intubated neonates;[3] however, surfactant administration may contribute to morbidity if it is not indicated. The benign course of the untreated neonates suggests that surfactant was not indicated. The low incidence of sepsis (2%) and NEC (4%), and the low mortality rate (1.9%) in our cohort relative to the higher rates reported in both high- and low-income countries, suggests that our management protocols are reasonable.[1,2] If a LUSS of 7 was used instead of an FiO2 of 0.35 - 0.45, 25% of the neonates who received surfactant would not have been treated, which may have led to later invasive intervention, while 28% of those who did not receive surfactant, would have been treated, with potentially increased morbidity.
Study limitations and strengths
Firstly, despite the small sample size employed in the present study, ROC analysis can still yield valuable insights, in exploratory or pilot studies (with small samples).[24] It is worth mentioning most descriptive elements in this study were based on proportions, which are less affected by sample size than continuous variables. Secondly, 14% of neonates were receiving HFHNC, and LUS may appear different with HFHNC compared with nCPAP. Third, inclusion of neonates >32 weeks' GA led to low surfactant requirements. Despite these limitations, this is the first study to contribute neonatal LUS data from an SA centre. Uniformity was promoted by single-centre data-collection by one clinician performing LUS scans, and bias was limited with LUS interpretation by a blinded clinician. Additionally, while sample size constraints limit generalisability, it does not invalidate the trends observed.
Conclusion
Early LUS of surfactant-naïve preterm neonates, receiving HFHNC or nCPAP, identified a wider range of diagnoses than clinical assessment alone, but the predictive values of LUS scores for surfactant administration at FiO2 thresholds 0.35 - 0.45, were low. The high frequency of TTN features in the non-surfactant group, and the associated benign clinical course, highlights TTN as an alternative diagnosis. Our findings do not preclude potential predictive value of LUSS for surfactant administration, at lower GA or lower FiO2 thresholds. The present exploratory study provides foundational data in an SA neonatal population, but larger, gestation-stratified studies in similar settings are needed to robustly determine the validity of our findings.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for MPhil (Neonatology), University of Cape Town.
Acknowledgements. We thank and acknowledge Susan Perkins for assistance with proofreading and editing. We acknowledge and thank the Department of Neonatology at Groote Schuur Hospital for administrative assistance.
Author contributions. Conceptualisation: FM-J and ARH; methodology: FMJ, ARH and WB; software: FMJ, ARH and WB; validation: FMJ and ARH; formal analysis: WB; investigation: FMJ; resources: ARH; data curation: FMJ, ARH and WB; writing - original draft preparation: FMJ and ARH; writing - review and editing: FMJ, ARH, and WB; visualization: FMJ and ARH; supervision: ARH; project administration: FMJ and ARH; funding acquisition: FMJ. All authors have read and agreed to the published version of the manuscript.
Funding. This study was funded in part by a research award from the Department of Paediatrics and Child Health in the Faculty of Health Sciences at the University of Cape Town.
Conflics of interest. None.
References
1. Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology 2019;115(4):432-450. https://doi.org/10.1159/000499361 [ Links ]
2. Hubbard RM, Choudhury KM, Lim G. Treatment patterns and clinical outcomes in neonates diagnosed with respiratory distress syndrome in a low-income country: A report from Bangladesh. Obstetric Anesthesia Digest 2018:38(4):216-217. https://doi.org/10.1097/01.aoa.0000547316.94472.45 [ Links ]
3. Bahadue FL, Soll R. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database Syst Rev 2012;11(11):CD001456. https://doi.org/10.1002/14651858.CD001456.pub2 [ Links ]
4. Aly H. Respiratory disorders in the newborn: Identification and diagnosis. Pediatr Rev 2004;25(6):201-208. https://doi.org/10.1542/pir.25-6-201 [ Links ]
5. Capasso L, Pacella D, Migliaro F, De Luca D, Raimondi F. Can lung ultrasound score accurately predict the need for surfactant replacement in preterm neonates? A systematic review and meta-analysis protocol. PLoS ONE 2021;16(7):e0255332. https://doi.org/10.1371/journal.pone.0255332 [ Links ]
6. Raimondi F, Yousef N, Migliaro F, Capasso L, De Luca D. Point-of-care lung ultrasound in neonatology: Classification into descriptive and functional applications. Pediatric Res 2021;90:524-531. https://doi.org/10.1038/s41390-018-0114-9 [ Links ]
7. De Martino L, Yousef N, Ben-Ammar R, Raimondi F, Shankar-Aguilera S, De Luca D. Lung ultrasound score predicts surfactant need in extremely preterm neonates. Pediatrics 2018;142(3):e20180463. https://doi.org/10.1542/peds.2018-0463 [ Links ]
8. Brat R, Yousef N, Klifa R, Reynaud S, Aguilera SS, De Luca D. Lung ultrasonography score to evaluate oxygenation and surfactant need in neonates treated with continuous positive airway pressure. JAMA Pediatr 2015;169(8):e151797. https://doi.org/10.1001/jamapediatrics.2015.1797 [ Links ]
9. Rodriguez-Fanjul J, Jordan I, Balaguer M, Batista-Muñoz A, Ramon M, Bobillo-Perez S. Early surfactant replacement guided by lung ultrasound in preterm newborns with RDS: The ULTRASURF randomised controlled trial. Eur J Pediatr 2020;179(12):1913-1920. https://doi.org/10.1007/s00431-020-03744-y [ Links ]
10. Gomond-Le Goff C, Vivalda L, Foligno S, Loi B, Yousef N, De Luca D. Effect of different probes and expertise on the interpretation reliability of point-of-care lung ultrasound. Chest 2020;157(4):924-931. https://doi.org/10.1016/j.chest.2019.11.013 [ Links ]
11. Corsini I, Parri N, Gozzini E, et al. Lung ultrasound for the differential diagnosis of respiratory distress in neonates. Neonatology 2019;115(1):77-84. https://doi.org/10.1159/000493001. [ Links ]
12. Ballard J, Khoury J, Wedig K, Wang L, Eilers-Walsman BL, Lipp R. New Ballard Score, expanded to include extremely premature infants. J Pediatr 1991;119(3):417-423. https://doi.org/10.1016/s0022-3476(05)82056-6 [ Links ]
13. Van Wyk L, Smith J. Postnatal Foot Length to Determine Gestational Age: A pilot study. J Trop Pediatr 2016;62(2):144-151. https://doi.org/10.1093/tropej/fmv093 [ Links ]
14. Paul SP, Khattak H, Kini PK, Heaton PA, Goel N. NICE guideline review: neonatal infection: antibiotics for prevention and treatment (NG195). Arch Dis Child Educ Pract Ed 2022;107(4):292-297. https://doi.org/10.1136/archdischild-2021-322349 [ Links ]
15. Migliaro F, Salome S, Corsini I, et al.; NeoLUS Collaborative Study Group. Neonatal lung ultrasound: From paradox to diagnosis... and beyond. Early Hum Dev 2020;150:105184. https://doi.org/10.1016/j.earlhumdev.2020.105184 [ Links ]
16. Copetti R, Cattarossi L. The 'double lung point': An ultrasound sign diagnostic of transient tachypnea of the newborn. Neonatology 2007;91(3):203-209. https://doi.org/10.1159/000097454 [ Links ]
17. Liu J, Wang Y, Fu W, Yang CS, Huang JJ. Diagnosis of neonatal transient tachypnea and its differentiation from respiratory distress syndrome using lung ultrasound. Medicine 2014;93(27):e197. https://doi.org/10.1097/md.0000000000000197 [ Links ]
18. Rath C, Suryawanshi P. Point-of-care neonatal ultrasound in neonatology. J Neonatol2018;32(1):27-37. https://doi.org/10.1177/0973217918766994 [ Links ]
19. Lichtenstein D, Mezière G, Biderman P, Gepner A. The 'lung point': An ultrasound sign specific to pneumothorax. Intensive Care Med 2000;26(10):1434-1440. https://doi.org/10.1007/s001340000627 [ Links ]
20. Singh P, Patnaik S, Verma A, Garegrat R, Maheshwari R, Suryawanshi P. Diagnostic utility of lung ultrasound in predicting the need for surfactant therapy in preterm neonates with respiratory distress. Front Pediatr 2023;11:1307761. https://doi.org/10.3389/fped.2023.1307761 [ Links ]
21. Wang J, Wei H, Chen H, et al. Application of ultrasonography in neonatal lung disease: An updated review. Front Pediatr 2022;10:1020437. https://doi.org/10.3389/fped.2022.1020437 [ Links ]
22. Wang Y, Li N, Qu Y. Diagnostic accuracy of lung ultrasound for transient tachypnea: A meta-analysis. J Pediatr 2022;98(4):329-337. https://doi.org/10.1016/j.jped.2021.10.003 [ Links ]
23. Liu J, Liu F, Liu Y, Wang HW, Feng ZC. Lung Ultrasonography for the diagnosis of severe neonatal pneumonia. Chest 2014;146(2):383-388. https://doi.org/10.1378/chest.13-2852 [ Links ]
24. Obuchowski NA, Bullen JA. Receiver operating characteristic (ROC) curves: Review of methods with applications in diagnostic medicine. Phys Med Biol 2018;63(7):07TR01. http://doi.org/10.1088/1361-6560/aab4b1 [ Links ]
 Correspondence:
Correspondence:
A R Horn
alan.horn@uct.ac.za
Received 14 September 2024
Accepted 21 January 2025

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}