










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671Print version ISSN 1994-3032
S. Afr. j. child health vol.19 n.3 Pretoria Sep. 2025
https://doi.org/10.7196/SAJCH.2025.v19i3.3002
ARTICLE
Profile of paediatric patients with appendicitis at an academic hospital after admission criteria change
E SteinI; D BenjaminII; K PillayI; M SyedIII; L MoleleIII; K JohannesI; T GablerIV
IBHSc Hons; School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMBA; School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIBPharm; School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVFC Paed Surg (SA) Department of Paediatric Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Appendicitis is the most common surgical emergency in children. During the COVID-19 pandemic, Chris Hani Baragwanath Academic Hospital (CHBAH) raised the cut-off age for paediatric surgery admission from 10 to 14 years owing to constraints placed on preexisting systems. This change resulted in a new profile of appendicitis cases within the department.
OBJECTIVES. To describe the profile of paediatric patients with appendicitis at CHBAH following the implementation of an age limit change in admission criteria.
METHODS. This retrospective descriptive study reviewed all patients aged <14 years who were managed for appendicitis in the Department of Paediatric Surgery at CHBAH between July 2020 and June 2023.
RESULTS. A total of 308 patients was included in the study. The mean age at presentation was 9.4 years, with a male-to-female ratio of 1.6:1. Almost half (45.1%) of the patients were >10 years of age. Of the total patients, over two-thirds (69.5%) presented with complicated appendicitis, and almost all (95.1%) underwent surgical management. Compared with patients with uncomplicated appendicitis, those with complicated appendicitis had significantly more postoperative complications (p<0.001), a higher re-admission rate (p=0.004), required more re-look procedures (p<0.001), had longer hospital stays (p<0.001), and had a higher mortality rate (p<0.001).
CONCLUSIONS. This study reveals a concerning prevalence of complicated appendicitis in paediatric patients, highlighting the necessity for prompt diagnosis and intervention. An increased patient load strained paediatric surgery hospital resources, while the COVID-19 pandemic likely worsened treatment delays. Ongoing research is essential for optimising management strategies and improving surgical outcomes.
Appendicitis is the most common surgical emergency affecting the abdomen in children, with an estimated lifetime risk of about 7%.[1,2] In South Africa, appendicitis occurs at an approximate rate of 15 per 100 000 person-years.[3] However, this is probably underestimated owing to the scarcity of epidemiological data, which may be ascribed to limited access to healthcare and inaccurate reporting. These factors may contribute to both underdiagnosis and delayed diagnosis, resulting in a higher proportion of patients presenting with complications such as perforation, gangrene, and abscess formation.[1,4] Diagnosing appendicitis in children can be challenging owing to non-specific symptoms such as nausea, vomiting, and abdominal pain, which can mimic other conditions such as gastroenteritis, urinary tract infections or respiratory tract infections.[2,5,6] Poor communication skills in younger children further increase the risk of misdiagnosis or delayed diagnosis, leading to a higher likelihood of complicated or perforated appendicitis. Perforation rates are higher in males,[3,4] in children younger than five years old,[5] and in those from lower socioeconomic backgrounds.[7,8]
Appendicectomy is considered the treatment of choice for acute appendicitis, with laparoscopic surgery being the preferred approach owing to its benefits of less pain, shorter hospital stays, and faster postoperative recovery compared with an open approach. [6,9] Despite this, open appendicectomies are still widely performed, especially in resource-constrained settings, owing to reduced cost, shorter operative times, and lower intra-abdominal abscess risk. [9] Nonoperative antibiotic treatment has been suggested as an alternative to surgery in uncomplicated cases, despite its reduced treatment efficacy and increased readmission rate compared with surgical treatment.[1,10]
The COVID-19 pandemic significantly exacerbated challenges faced by healthcare systems, including the diagnosis and management of appendicitis. A pre-pandemic review - conducted between June 2010 and September 2015 - studied 234 paediatric patients with appendicitis at Chris Hani Baragwanath Academic Hospital (CHBAH), a tertiary hospital in Johannesburg, South Africa. At the time of this study, the cut-off age for admission to the paediatric surgery department was 10 years. The mean age was 7.3 years, and 55.8% of the patients had complicated appendicitis.[4] However, owing to constraints placed on pre-existing systems during the COVID-19 pandemic, the admission criteria for patients to the paediatric surgical ward at CHBAH increased from an age limit of 10 years to 14 years. The pandemic may have inadvertently further burdened the paediatric surgical unit and a public health system with already limited availability of resources, and disparities in access to healthcare. The sustained change in the age limit, together with the changes induced by the pandemic, may have contributed to a change in the profile of paediatric patients with appendicitis at CHBAH.
Aims and objectives
The present study aimed to describe the profile of paediatric patients with appendicitis at CHBAH between 1 July 2020 and 30 June 2023 following the implementation of an age limit change in admission criteria.
The objectives of this study were to describe:
• the demographic profile regarding age and sex
• the nature of appendicitis
• the nature of the intervention for appendicitis
• the number, type and management of complications and corrective surgery performed.
Methods
Study design, population and setting
This retrospective descriptive study reviewed all patients aged 14 years and younger who were managed for appendicitis in the Department of Paediatric Surgery at CHBAH. Located in Soweto, South Africa, it is the third-largest hospital in the world and has a rapidly expanding paediatric surgical unit that serves almost 12 000 patients a year. The study period was from 1 July 2020 to 30 June 2023. The study period commenced on the day that the age limit change at CHBAH was implemented. Patients were excluded from the study if they were diagnosed with a condition other than appendicitis or if they went to theatre with suspected appendicitis and had a negative operation. Incomplete records were also excluded from the study.
Data collection and definitions
A consecutive convenience sampling method was used. Patient records were identified from the hospital's Healthspace database using the International Classification of Diseases (ICD-10) codes for appendicitis. De-identified data from records within the study period were collected and managed using a data collection instrument on REDCap (Research Electronic Data Capture). The variables included were patient demographics (age and sex), type of appendicitis, management received, the surgical approach used for appendicectomy, intra-operative findings, postoperative complications, number of re-admissions, intensive care unit (ICU) admission, length of hospital stay, number of re-looks performed, and mortality rate.
Patients were categorised as having either uncomplicated or complicated appendicitis based on imaging and/or intra-operative findings: patients with an inflamed, unperforated appendix were regarded as having uncomplicated appendicitis, while those who had a perforation, gangrene, faecolith and/or appendiceal abscess/ mass were considered to have complicated appendicitis.'11 The type of management received was either non-surgical or surgical. Non-surgical management was determined to be the use of antibiotics only. The surgical approaches were either open, laparoscopic or laparoscopic converted to open. Postoperative complications were graded according to the Clavien Dindo classification,'111 and grouped as less severe (Clavien Dindo I-II) or severe (Clavien Dindo III-IV) complications.
Data analysis
All data were recorded in Microsoft Excel, and statistical analysis was performed using GraphPad Prism v. 10.2.3 (GraphPad Software, California, USA). Continuous, parametric data are presented as mean (standard deviation, SD), and non-parametric data are presented as median (interquartile range (IQR)). Categorical variables are expressed as numbers and percentages. Student's t-test was used to compare mean values for continuous, parametric data, and the Mann-Whitney U test was used to compare differences between continuous, non-parametric variables. The chi-squared or Fisher's exact test was used to compare categorical variables, as appropriate. Statistical significance was defined as p<0.05.
Permission to conduct this study was obtained from the Human Research Ethics Committee at the University of the Witwatersrand (ethics no. M230941). No study-specific consent and assent from the caregivers and patients was necessary, as consent for using clinical data for research was obtained upon admission to the Department of Paediatric Surgery at CHBAH.
Results
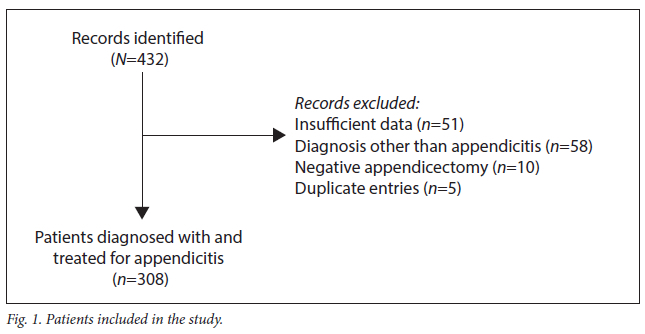
During the study period, 432 records were identified, of which 124 were excluded owing to insufficient data, a diagnosis other than appendicitis, or a negative appendicectomy. Duplicate entries were also excluded. In total, 308 paediatric patients were diagnosed with and treated for appendicitis at CHBAH (Fig. 1).
Patient demographics and clinical characteristics
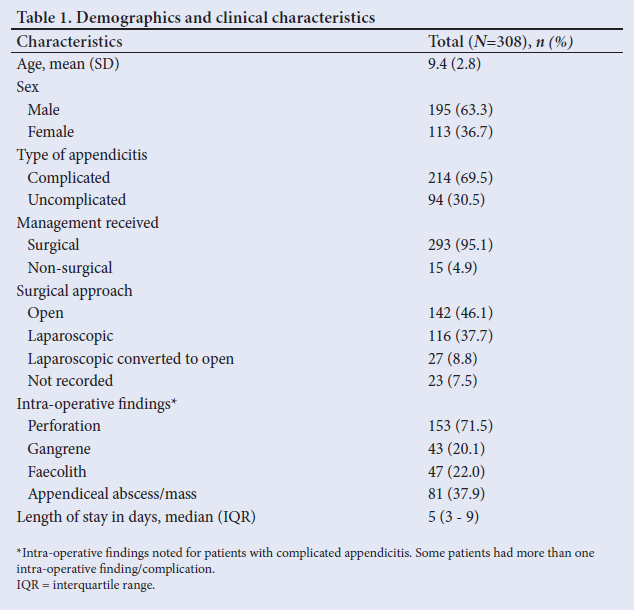
Patient demographics and clinical characteristics are presented in Table 1.
The mean (SD) age was 9.4 (2.8) years, and the male-to-female ratio was 1.6:1. Complicated appendicitis was diagnosed in 214 (69.5%) patients. Almost all patients (95.1%) underwent surgical management, of whom 142 (46.1%) had an open appendicectomy, 116 (37.7%) had a laparoscopic appendicectomy, and 27 (8.8%) required conversion to an open approach. A perforated appendix was the most common finding in patients with complicated appendicitis, occurring in 153 (71.5%) cases, followed by an appendiceal abscess/ mass which was observed in 81 (37.9%) cases. The median (IQR) length of hospital stay, including readmissions, was 5 (3 - 9) days, with the longest duration of admission being 68 days.
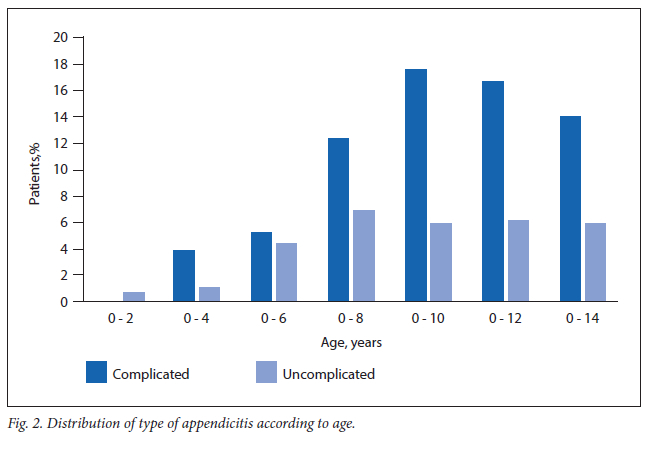
The prevalence of complicated appendicitis was notably higher than that of uncomplicated appendicitis across all age groups, except for those under 2 years of age, with a marked increase in children above the age of 7 years. The prevalence of uncomplicated appendicitis was nearly equal in children between the ages of 9 and 14 years (Fig. 2).
Comparisons of complicated and uncomplicated appendicitis
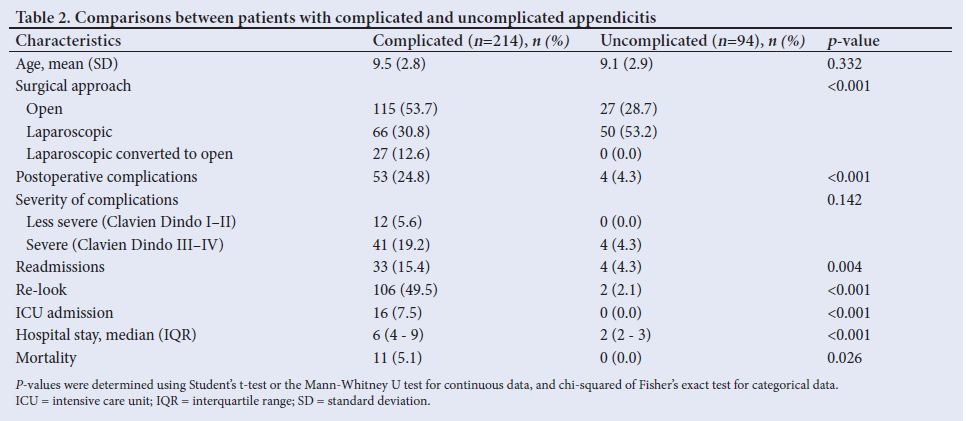
The initial surgical approach differed significantly in patients with complicated and uncomplicated appendicitis. In patients with complicated appendicitis, 115 (53.7%) underwent an open appendicectomy, 66 (30.8%) had a laparoscopic appendicectomy, and 27 (12.6%) required conversion to an open approach. In contrast, in patients with uncomplicated appendicitis, 27 (28.7%) had an open appendicectomy, 50 (53.2%) had a laparoscopic appendicectomy, and none required conversion to an open approach (p<0.001). Postoperative complications were significantly more prevalent in patients with complicated appendicitis compared with those with uncomplicated appendicitis (p<0.001). However, there was no significant difference between the two groups in terms of the severity of complications (p=0.142). Patients with complicated appendicitis had a significantly higher rate of readmissions and re-look procedures than those with uncomplicated appendicitis (p=0.004 and p<0.001, respectively). All intensive care unit (ICU) admissions were for patients with complicated appendicitis, with 14 of the 16 admissions being for patients who underwent an open appendicectomy as their index procedure. The median length of hospital stay was significantly longer in patients with complicated appendicitis compared with those with uncomplicated appendicitis (6 v. 2 days, p<0.001). Lastly, there was a total of 11 (3.6%) mortalities, all of which occurred in patients with complicated appendicitis and those who had undergone a laparotomy as their index procedure (Table 2).
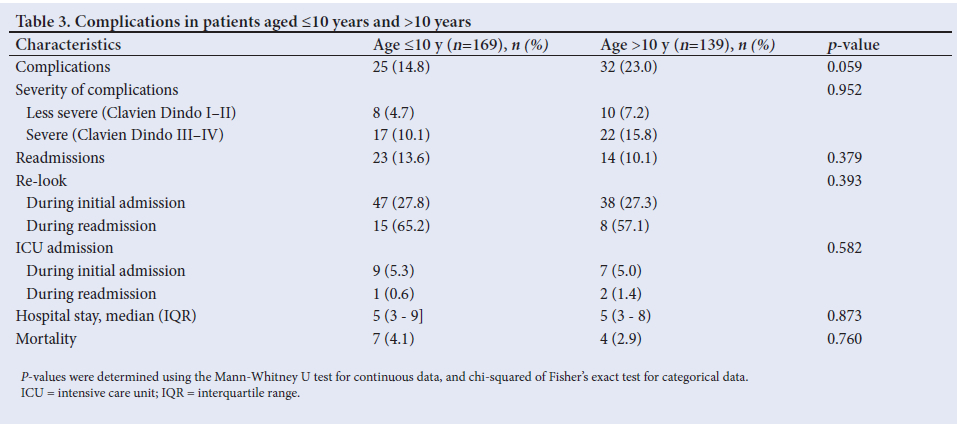
Comparisons of complications in patients aged <10 years and >10 years
There were no significant differences among patients aged <10 years and >10 years in terms of the number of postoperative complications, severity of complications, number of readmissions, number of re-look operations, ICU admissions, total length of hospital stay, or number of mortalities (Table 3)
Discussion
Our study described the profile of paediatric patients with appendicitis at a tertiary hospital following a change in admission criteria as a result of the COVID-19 pandemic. Acute appendicitis remains one of the most common surgical emergencies in the paediatric population, with its incidence typically peaking during the teenage years. [1] The mean age of patients in our sample was 9.4 years, which was higher than the average age of 7.3 years in children with appendicitis at our institution prior to the age change,[4] but younger than the globally reported peak age of between 12 and 18 years.[12] In terms of sex distribution, the male-to-female ratio of 1.6:1 in our study is consistent with global trends that typically indicate a male predominance in appendicitis cases.[1,3]
Complicated appendicitis is diagnosed when there is evidence of a perforated or gangrenous appendix, or the presence of an appendiceal abscess or mass.[1,13] The rate of complicated appendicitis at our institution increased from 55% in a pre-pandemic study[4] to 69% during our study. Complicated appendicitis accounts for up to 30% of cases in children.[14] Although our prevalence of complicated appendicitis cases is significantly higher than this reported rate, our findings are consistent with those of other institutions that have also found an increased incidence of complicated appendicitis during the pandemic. For instance, a retrospective study based on cases from three medical centres in Israel found an increase in complicated appendicitis rates from 11% before the pandemic to 22% during the pandemic.[15] Similarly, another study in 281 patients admitted with acute appendicitis to an academic medical centre in the United States found a 21% increase in the number of perforated appendicitis cases and a 29% increase in the number of patients with a gangrenous appendix during the pandemic.[16]
Several factors may have contributed to the elevated rates of complicated appendicitis in our cohort. The COVID-19 pandemic led to significant disruptions in access to healthcare, particularly in South Africa, where stringent lockdown measures and fear of contracting the virus likely contributed to delays in seeking medical care.[17] Consequently, many children with acute appendicitis may have presented later in the disease course when perforation or gangrene had already occurred. Additionally, strained healthcare resources, such as limited operating theatres, hospital beds and medical staff, may have further prolonged the time to treatment, increasing the risk for complications in these patients. Accordingly, over 70% of patients in our cohort with complicated appendicitis were found to have a perforated appendix.
Almost all patients in our study underwent surgical management, with more patients receiving an open appendicectomy than a laparoscopic appendicectomy. This approach is in contrast with recent global trends favouring laparoscopic appendicectomies as the preferred approach for appendicitis owing to their minimally invasive nature, quicker postoperative recovery times, shorter hospital stays, and reduced rates of postoperative complications.[6,9] However, in our setting, the preference for open procedures may have been driven by the prohibitive costs of, and decreased access to, laparoscopic equipment.
Specifically, open appendicectomies were favoured, particularly early in the pandemic, owing to their lower aerosol production and reduced risk of viral transmission.[12-18] As a result, access to laparoscopic surgery was restricted in many institutions, including ours. In addition, open procedures may have been preferred owing to a quicker surgical time, which was advantageous given the high surgical demand owing to a high patient load. The high rate of open appendicectomies in our cohort, along with the decreased use of non-surgical treatment with antibiotics alone, may have also reflected the complexity of the cases, with complicated appendicitis often necessitating open surgery owing to extensive intra-abdominal contamination or difficulty visualising the appendix laparoscopically.
Postoperative outcomes in our study were closely linked to the severity of appendicitis, as patients with complicated appendicitis experienced higher rates of postoperative complications, readmission rates, re-look operations, prolonged hospital stays, and increased mortality rates. This is consistent with studies which have shown complicated appendicitis to be a strong predictor of adverse outcomes, particularly in patients with a perforated appendix.[13,15,17] These adverse outcomes ultimately reduced the time and resources available to treat other paediatric cases in the department. Furthermore, perforated appendicitis carries a mortality rate of around 5% globally.[6] Our mortality rate of 5.1% closely aligns with this figure but remains significantly higher than the rates observed solely in higher-income countries, where paediatric appendicitis mortality rates are typically less than 1%.[1] These findings demonstrate the significant risk associated with more complicated cases, as all of our mortalities occurred in patients with complicated appendicitis.
Lastly, the age-related change in admission criteria had a notable impact on the Department of Paediatric Surgery at CHBAH. Firstly, in the previous study conducted at our institution before the pandemic, the total sample size was 234 over five years.[4] In comparison, we had a sample size of 308 over three years, resulting in the department managing more patients in a shorter period. Notably, although we found no significant differences in complications between children younger and older than 10 years, the children over the age of 10 years comprised almost half (n=139 out of 308) of the study population, leading to a marked increase in the overall patient load. Of the patients above the age of 10 years, 46 required re-look procedures, which reduced available theatre time for other patients in the department. Additionally, the patients in this group collectively spent a total of 800 days in the hospital, reducing the time and resources available for treating other paediatric cases. Despite the increased demand during this period, the department received no additional resources, including increased staff or bed capacity. This lack of support and the heightened patient volume placed considerable strain on existing resources and clinical staff, potentially impacting workflow and compromising the efficiency of overall patient management and care.
There were several limitations to this study. Firstly, its retrospective nature may have lent itselfto all biases associated with retrospective data collection. Additionally, this study was conducted at a single institution, which may limit the generalisability of our findings to other settings. Our institution's healthcare infrastructure, patient population, and surgical practices may not reflect those in different regions of South Africa or globally, introducing potential selection and sampling biases. Lastly, the timing of our data collection coincided with the COVID-19 pandemic, which has been linked to a global rise in complicated appendicitis cases. As we did not control for confounding variables such as acute COVID-19 infections or comorbidities, our sample may have been biased towards more severe cases, potentially limiting the generalisability of our findings to non-pandemic conditions.
Conclusion
Our study highlights a concerning prevalence of complicated appendicitis among paediatric patients, underscoring the need for timely diagnosis and intervention to reduce morbidity and mortality. The increased patient load placed considerable strain on the Department ofPaediatric Surgery at CHBAH, and the impact ofthe COVID-19 pandemic on healthcare access likely exacerbated delays in diagnosis and treatment, revealing potential systemic vulnerabilities in managing acute surgical conditions. Continued research and prospective data collection will allow for refined management strategies, help advocate for improved distribution of staffing and clinical resources, and ultimately enhance patient care and surgical outcomes in paediatric patients with appendicitis.
Declaration. None.
Acknowledgements. We would like to thank Steven Mutangwa Mulalo and Yola Nomfula for their assistance with data collection.
Author contributions. ES conceptualised the study, collected and analysed the data, and wrote the final manuscript. DB designed the data collection instrument, assisted with data collection, and reviewed and revised the manuscript. KP, MS, LM and KJ assisted with data collection, and contributed to and edited the final manuscript. TG conceptualised and supervised the study, and edited and revised the final manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Bhangu A, Søreide K, Saverio S Di, Assarsson JH, Drake FT. Acute appendicitis: Modern understanding of pathogenesis, diagnosis, and management. Lancet 2015;386(10000): 1278-1287. https://doi.org/10.1016/S0140-6736(15)00275-5 [ Links ]
2. Aneiros B, Cano I, García A, Yuste P, Ferrero E, Gómez A. Pediatric appendicitis: Age does make a difference. Rev Paul Pediatr 2019;37:318-324. https://doi.org/10.1590/1984-0462/;2019;37;3;00019 [ Links ]
3. Ferris M, Quan S, Kaplan BS, et al. The global incidence of appendicitis: A systematic review of population-based studies. Ann Surg 2017;266(2):237-241. https://doi.org/10.1097/SLA.0000000000002188 [ Links ]
4. Withers A, Loveland J. Demographics of paediatric patients presenting with acute appendicitis: A 5-year retrospective review of hospitals served by the Department of Paediatric Surgery at the University of the Witwatersrand. S Afr J Child Health 2019;13(2):69-72. https://doi.org/10.7196/SAJCH.2019.v13i2.1557 [ Links ]
5. Almaramhy HH. Acute appendicitis in young children less than 5 years: Review article. Ital J Pediatr 2017;43(1):15. https://doi.org/10.1186/s13052-017-0335-2 [ Links ]
6. Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines.World J Emerg Surg 2020;15(1):27. https://doi.org/10.1186/s13017-020-00306-3 [ Links ]
7. Goyal MK, Chamberlain JM, Webb M, et al. Racial and ethnic disparities in the delayed diagnosis of appendicitis among children. Acad Emerg Med 2021;28(9):949-956. https://doi.org/10.1111/acem.14142 [ Links ]
8. Wang L, Haberland C, Thurm C, Bhattacharya J, Park KT, Abe T. Health outcomes in US children with abdominal pain at major emergency departments associated with race and socioeconomic status. PLoS One 2015;10(8):e0132758. https://doi.org/10.1371/journal. pone.0132758 [ Links ]
9. Sartelli M, Baiocchi GL, Di Saverio S, et al. Prospective observational study on acute appendicitis worldwide (POSAW). World J Emerg Surg 2018;13:19. https://doi.org/10.1186/s13017-018-0179-0 [ Links ]
10. Kessler U, Mosbahi S, Walker B, et al. Conservative treatment versus surgery for uncomplicated appendicitis in children: A systematic review and meta-analysis. Arch Dis Child 2017;102(12):1118-1124. https://doi.org/10.1136/archdischild-2017-313127 [ Links ]
11. Pogorelic Z, Anand S, Zuvela T, Singh A, Krizanac Z, Krishnan N. Incidence of complicated appendicitis during the COVID-19 pandemic versus the pre-pandemic period: A systematic review and meta-analysis of 2782 pediatric appendectomies. Diagnostics 2022;12(1):127. https://doi.org/10.3390/diagnostics12010127 [ Links ]
12. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications. Ann Surg 2009;250(2):187-196. https://doi.org/10.1097/SLA.0b013e3181b13ca2 [ Links ]
13. Schäfer FM, Meyer J, Kellnar S, et al. Increased Incidence of perforated appendicitis in children during COVID-19 pandemic in a Bavarian multicenter study. Front Pediatr 2021;9:683607. https://doi.org/10.3389/fped.2021.683607 [ Links ]
14. Pham XBD, Sullins VF, Kim DY, et al. Factors predictive of complicated appendicitis in children. J Surg Res 2016;206(1):62-66. https://doi.org/10.1016/j.jss.2016.07.023 [ Links ]
15. Snapiri O, Rosenberg Danziger C, et al. Delayed diagnosis of paediatric appendicitis during the COVID-19 pandemic. Acta Paediatr2020;109(8):1672-1676. https://doi.org/10.1111/apa.15376 [ Links ]
16. Orthopoulos G, Santone E, Izzo F, et al. Increasing incidence of complicated appendicitis during COVID-19 pandemic. Am J Surg 2021;221(5):1056-1060. https://doi.org/10.1016/j.amjsurg.2020.09.026 [ Links ]
17. Gerall CD, DeFazio JR, Kahan AM, et al. Delayed presentation and sub-optimal outcomes of pediatric patients with acute appendicitis during the COVID-19 pandemic. J Pediatr Surg 2021;56(5):905-910. https://doi.org/10.1016/j.jpedsurg.2020.10.008 [ Links ]
18. Antakia R, Xanthis A, Georgiades F, et al. Acute appendicitis management during the COVID-19 pandemic: A prospective cohort study from a large UK centre. Int J Surg 2021;86:32-37. https://doi.org/10.1016/j.ijsu.2020.12.009 [ Links ]
 Correspondence:
Correspondence:
E Stein
emma.steinl@outlook.com
Received 10 January 2025
Accepted 4 June 2025

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}