










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671Print version ISSN 1994-3032
S. Afr. j. child health vol.19 n.4 Pretoria Dec. 2025
https://doi.org/10.7196/SAJCH.2025.v19i4.2893
RESEARCH
Impact of the COVID-19 pandemic on neonatal services and outcomes in a tertiary hospital in Tshwane, South Africa
M CoetzeeI; R M TshehlaI; H NaidooII; H MulolIII, IV, V; U FeuchtVI, VII, VIII
IMB ChB, DCH (SA), FCPaed (SA), MMed (Paeds), Cert Neonatol (SA); Department of Paediatrics and Child Health, University of Pretoria, South Africa
IIMB ChB, FCPaed (SA), MMed (Paeds), Cert Neonatol (SA); Department of Paediatrics and Child Health, University of Pretoria, South Africa
IIIPhD; Department of Paediatrics and Child Health, University of Pretoria, South Africa
IVPhD; Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies, University of Pretoria, South Africa
VPhD; Maternal and Infant Health Care Strategies Research Unit, South African Medical Research Council, Pretoria, South Africa
VIMB ChB, FCPaed (SA), MMed (Paeds), Dipl HIV Man (SA), CAHM, PhD; Department of Paediatrics and Child Health, University of Pretoria, South Africa
VIIMB ChB, FCPaed (SA), MMed (Paeds), Dipl HIV Man (SA), CAHM, PhD; Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies, University of Pretoria, South Africa
VIIIMB ChB, FCPaed (SA), MMed (Paeds), Dipl HIV Man (SA), CAHM, PhD; Maternal and Infant Health Care Strategies Research Unit, South African Medical Research Council, Pretoria, South Africa
ABSTRACT
BACKGROUND. The COVID-19 pandemic's collateral damage has severely impacted global child health services. This study investigates its effects on neonatal services and outcomes at a tertiary hospital in Tshwane, South Africa.
OBJECTIVE. The main aim was to assess if decreased breastfeeding, coupled with increased infant formula use owing to COVID-19-related visitation disruptions, was associated with higher incidences of healthcare-associated infections (HAI) and necrotising enterocolitis (NEC) in the hospital's neonatal unit.
METHODS. As part of the Tshwane Maternal-Child COVID-19 study, we collected relevant data from three periods: pre-COVID-19, COVID-year-1 (COVID-Y1) and COVID-year-2 (COVID-Y2).
RESULTS. Exclusive breastfeeding at discharge decreased from 72.9% pre-COVID-19 to 47.0% during COVID-19. Preterm formula purchases rose by 37.5% in COVID-Y1 and 25.0% in COVID-Y2, and term formula purchases increased by 77.8% in COVID-Y1. HAI incidence increased in both COVID-Y1 and COVID-Y2 compared with pre-COVID-19 (11.6% v. 8.1% and 12.0% v. 8.1%). NEC incidence significantly increased in COVID-Y2 for infants >1 500 g (1.8% v. 0.7%).
CONCLUSION. This study underscores the indirect consequences of COVID-19 parental visitation restrictions, leading to infringements of breastfeeding rights and coinciding with increased HAI and NEC incidences in the hospital's neonatal unit.
Keywords: Breast feeding; COVID-19; healthcare-associated infections; necrotising enterocolitis; neonatal outcomes.
The collateral damage from the COVID-19 pandemic has been devastating to many healthcare facilities, especially to child health services. The present study examines the indirect impact on neonatal services and outcomes at a tertiary hospital in Tshwane, South Africa, by comparing neonatal care before and during the pandemic.
All infants should have the right to breastfeed, and benefit from it. For hospitalised infants, benefits include reduced rates of healthcare-associated infections (HAI) and necrotising enterocolitis (NEC).[1,2] Neonatal sepsis, which encompasses HAI, is among the top three causes of neonatal mortality worldwide.[3] HAI also impacts morbidity, length of stay and cost of care.[1] Acquiring a balanced microbiome from the mother during breastfeeding and skin-to-skin contact, supported by bioactive factors in breast milk, is crucial in preventing HAI.[2,4]
To support breastfeeding, many hospitals have implemented the 10 steps to successful breastfeeding outlined by the mother-baby-friendly hospital initiative (MBFHI). These steps include policies aligned with the International Code of Marketing of Breast Milk Substitutes, a written infant feeding policy, staff training to support breastfeeding, immediate skin-to-skin, promoting 'rooming-in, teaching mothers to recognise feeding cues, and avoiding breastmilk substitutes unless medically indicated.[5] Research from the World Health Organization indicates that mortality risk in the first 28 days of life is 33% higher if breastfeeding starts 2 - 23 hours post delivery, compared to within the first hour. This risk more than doubles if initiated after the first day.[5] Unfortunately, COVID-19 visitation restrictions resulted in decreased breast milk feeding during some periods, particularly across the four COVID-19 waves in South Africa, namely 7 June - 22 August 2020, 15 November 2020 - 6 February 2021, 9 May - 18 September 2021 and 28 November 2021 - 5 February 2022, respectively.
Mother-baby-pairs faced separation for various COVID-19-related reasons. Direct separation occurred when COVID-positive mothers were too ill to care for their babies, or when babies born to COVID-positive mothers required admission. Indirect reasons included the no/limited visitation policies adopted by the hospital on 26 March 2020, closure of the kangaroo-mother-care (KMC) facility at a neighbouring hospital on 28 March 2020 and closure of the mother lodger facility on 1 July 2020. The KMC facility was closed as this neighbouring hospital closed because the hospital was designated solely for COVID-19 care; it was re-opened in September 2022 after being closed for two-and-a-half years. The mother lodger facility, closed after a COVID-19 outbreak, was re-opened on 6 October 2020, with limited capacity. These visitation restrictions and facility closures contravened MBFHI recommendations.
During the COVID-19 pandemic, the unit's visitation policy underwent multiple changes in accordance with the South African COVID-19 lockdown, five-level alert system, and COVID-19 waves. The alert level system was based on COVID-19 spread (epidemiological trends) and health system readiness to respond to the burden of disease. A complete ban on visitation was implemented in March 2020, coinciding with South Africa's strictest lockdown, along with a halt on expressing mothers' breast milk owing to contamination fears. As positive cases decreased, visitation increased but, during the second wave in December 2020, restrictions tightened again. Although expressing breast milk was encouraged, formula and donor-expressed breast milk (DEBM) were used when necessary. Restrictions eased after the second wave, but returned during the third wave. The unit reopened to visitors from home in August 2021.
The primary objective of the present study was to assess whether decreased breast milk feeding, accompanied by increased formula use, was associated with increased culture-positive HAI and NEC in this unit during the COVID-19 pandemic. Secondary objectives included examining the impact on antenatal care (ANC), deliveries, bed occupancy, neonatal deaths and outpatient services.
Methods
Study design and setting
This research formed part of the Tshwane Maternal-Child COVID-19 study. All neonates admitted to the Steve Biko Academic Hospital neonatal unit were included in this study. This tertiary neonatal unit provides medical and surgical care to neonates from Tshwane and surrounding provinces. The neonatal unit consists of 39 beds, which include 10 neonatal intensive care beds; however, this unit is usually full to above capacity. For this study, 'pre-COVID-19' refers to April 2019 - March 2020, 'COVID-year-1' (COVID-Y1) to April 2020 - March 2021, and 'COVID-year-2' (COVID-Y2) to April 2021 - March 2022. Data for the neonatal unit were extracted from its database, while outpatient information was obtained from the outpatient register.
Variables
Formula purchases data were acquired from the dietetics department. Culture results (blood, urine, cerebral spinal fluid) for diagnosing bacterial and fungal HAI were confirmed using the National Health Laboratory Service database. Abdominal radiographs for diagnosing NEC (modified Bell's criteria grade 2 and 3) were reviewed by three resident neonatologists, with uncertain cases confirmed by reviewing the file. Infants with NEC from other facilities or with additional risk factors, such as congenital cyanotic heart disease, were excluded from the analysis (n=9). The hospital's Perinatal Problem Identification Programme (PPIP) analysed neonatal deaths, deliveries and ANC attendance. [6] Feeding practices were extracted from the Vermont Oxford Network (VON) database.[7] Ethics approval was obtained from the Research Ethics Committee of the Faculty of Health Sciences, University of Pretoria (ref: 822/2020), and the National Health Research Database (ref: GP_202011_076).
Statistical analysis
For statistical analysis, proportions for COVID-Y1 and COVID-Y2 were compared with pre-COVID-19 statistics using a 2-sided z-test. Continuous data were tested for normality using the Shapiro-Wilk test. As the data were not normally distributed, the Mann-Whitney U-test was used to compare birthweight between years. A p-value <0.05 indicated statistical significance.
Results
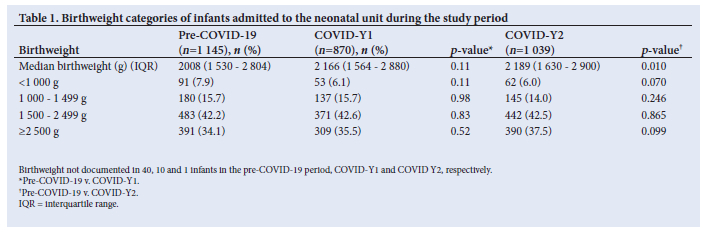
The median birthweight of admitted infants pre-COVID-19 was 2 008 g (interquartile range (IQR) 1 530 - 2 804 g), compared with 2 166 g (IQR 1 564 - 2 880 g) in COVID-Y1 (p=0.110) and 2 189 g (IQR 1 630 - 2 900 g) in COVID-Y2 (p=0.010). No significant differences were found between birthweight categories (Table 1).
Infant feeding
Separation of mother-baby pairs led to failure of exclusive breastfeeding, with increased formula use. VON data comparing pre-COVID-19 (2016) with COVID-19 (2021) indicates that breastfeeding decreased, while exclusive formula feeding increased. From 2016 to 2021, exclusive breastfeeding decreased from 72.9% to 47.0% (p<0.001), mixed feeding increased from 5.5% to 17.6% (p<0.001) and exclusive formula feeding increased from 5.1% to 25.4% (p<0.001) at discharge. This increase in formula feeding is supported by the dietetics department stock report for formula milk purchases (an indirect indicator of formula use). The use of preterm ready-to-use formula increased by 37.5% in COVID-Y1 and 25% in COVID-Y2 compared with pre-COVID-19 (both p<0.001). The use of preterm formula in tins in the dietetics outpatient service increased by 26.3% in COVID-Y1 and 84.2% in COVID-Y2 (both p<0.0001), while for term formula in tins the increase was 77.8% in COVID-Y1 (p<0.001) but returned to pre-COVID-19 levels in COVID-Y2. This was accompanied by an increase in DEBM use during the pandemic; although only infants weighing <1 300 g qualified owing to limited supply. The number of infants receiving DEBM per year pre-COVID-19 was 93 (7.8% of admissions), which increased to 102 (11.6% of admissions, p=0.003) in COVID-Y1 and 108 (10.4% of admissions, p=0.032) in COVID-Y2.
HAI and NEC incidence
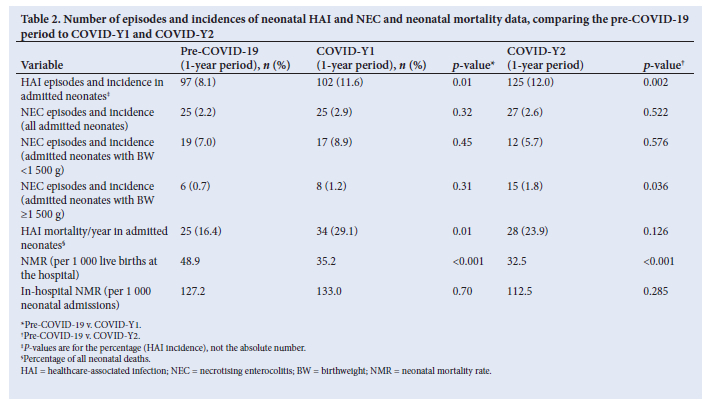
The HAI incidence per year, influenced by the number of admissions, significantly increased in COVID-Y1 and COVID-Y2 when compared with pre-COVID-19 (8.1% pre-COVID-19; 11.6% in COVID-Y1 (p=0.008); and 12.0% in COVID-Y2 (p=0.002) (Table 2).
For NEC incidence, the overall percentages of neonates diagnosed with NEC per year was not significantly different between pre-COVID-19, COVID-Y1 and COVID-Y2 (2.2%, 2.9% and 2.6%, respectively). In very low-birthweight (VLBW) infants (<1 500 g), NEC incidence rose from 7.0% pre-COVID-19 to 8.9% during COVID-Y1 (p=0.447) and down to 5.7% during COVID-Y2 (p=0.576). In infants >1 500 g, NEC incidence increased from 0.7% pre-COVID-19 to 1.2% in COVID-Y1 (p=0.313) and significantly to 1.8% in COVID-Y2 (p=0.036) (Table 2).
Neonatal mortality
PPIP data indicated that neonatal mortality related directly to HAI increased during the pandemic; significantly in COVID-Y1 (16.4% v. 29.1%, p=0.013), but not in COVID-Y2 (16.4% v. 23.9%, p=0.126). Conversely, the overall neonatal mortality rate (NMR) decreased significantly from 48.9 deaths per 1 000 live births pre-COVID-19 to 35.2 in COVID-Y1 and 32.5 in COVID-Y2 (both p<0.001). However, there was no significant difference in in-hospital neonatal mortality rate per 1 000 admissions between pre-COVID-19, COVID-Y1 and COVID-Y2 (127.2 v. 133.0, p=0.697 and 127.2 v. 112.5, p=0.285, respectively).
Admissions, bed occupancy and outpatient services
The strictest lockdown (26 March - 31 May 2020) led to decreased admissions and bed occupancy during COVID-Y1. Average bed occupancy, calculated as a percentage of the approved neonatal beds, dropped from 115% pre-COVID-19 to 103% in COVID-Y1 (p=0.048); with the lowest occupancy from April to August 2020 (72% - 97%). However, bed occupancy returned to baseline (118%) in COVID-Y2. Monthly admissions fell from an average of 100 pre-COVID-19 to 73 in COVID-Y1 (p<0.001) and 87 in COVID-Y2 (p=0.001). The proportion of neonates (of the total deliveries) admitted per year also decreased during COVID-Y1 and COVID-Y2 compared with pre-COVID-19 (24.9%, 27.3% and 35.8%, respectively; both p<0.001). Access to neonatal follow-up services was restricted, in keeping with hospital policy. Monthly outpatient follow-ups dropped from an average of 151 pre-COVID-19 to 62 in COVID-Y1 and 60 in COVID-Y2, (both p<0.001), representing an approximately 60% decrease in services.
Deliveries
Despite multiple COVID-19 lockdowns, the number of deliveries at the hospital increased significantly in both COVID-Y1 (n=3 541) and COVID-Y2 (n=3 810) compared with pre-COVID-19 (n=3 339, p=0.003 and p<0.001, respectively). Deliveries by caesarean section (CS) decreased during the pandemic, notably in COVID-Y2 (52.9% v. 57.2%, p<0.001) while changes from pre-COVID-19 to COVID-Y1 were not significant (56.3% v. 57.2%, p=0.453). The number of infants born outside the health facility (born before arrival (BBA)) per year increased from 36 pre-COVID-19 to 51 in COVID-Y1 and 76 in COVID-Y2. The BBA incidence, determined by the number of births at the hospital, increased significantly in COVID-Y2 (1.1% pre-COVID-19 v. 1.4% COVID-Y1, p=0.180 and 1.1% pre-COVID-19 v. 2.0% COVID-Y2, p=0.002). Mothers who did not attend ANC increased from 178 (pre-COVID-19) to 205 (COVID-Y1) to 229 (COVID-Y2) per year. However, when considering the number of deliveries, the non-attendance of ANC increased only slightly per year (5.7% v. 6.0%, p=0.516 and 5.7% v. 6.3%, p=0.289, respectively).
Discussion
To our knowledge, this is the first study to report on neonatal outcomes in South Africa during the COVID-19 pandemic, highlighting its negative indirect impact. The neonatal unit adhered to the National Department of Health's COVID-19 response framework and guidelines for maternal and neonatal care during a crisis, which restricted mothers from visiting or breastfeeding admitted babies,[8] despite limited evidence supporting this policy. These types of visitation restrictions were observed globally, with disruptions in family-centred care, including breastfeeding and skin-to-skin.[9] However, some argued that parents should not be considered as visitors, emphasising that preventing parental visitation violates children's rights, and that separation should be minimised.[10,11]
Effect on breastfeeding
In a bi-national survey performed in the United Kingdom (UK) and the United States of America between May and August 2020, it was found that 62% of parents reported that visitation restrictions during the COVID-19 pandemic limited time with their baby, with 36% noting adverse effects on breastfeeding. Additionally, 41% felt the restrictions hindered bonding with their baby. [12] Another UK survey stated that 69% of parents indicated that their mental health had deteriorated owing to their experience during the admission.[11] This highlights that visitation restrictions during the pandemic harmed both infants and parents, with indirect effects surpassing the direct effect of COVID-19 infections.
Breastfeeding failure was implied by increased purchases and use of preterm and term formula during the pandemic. This trend persisted post discharge, as evidenced by increased use of preterm formula tins for outpatient management of poor growth in discharged infants in this period.
Effect on HAI and NEC
The significant increase in HAI incidence from pre-COVID-19 to both COVID-Y1 (8.1% v. 11.6%) and COVID-Y2 (8.1% v. 12.0%) is likely related to reduced breast milk use, as indicated by the VON, and increased purchase of term and preterm formula. The risks for HAI are multifactorial, and mother-infant separation and changes in the infant microbiome likely contributed.[2,4] The increase in the HAI incidence was an unexpected finding as increased hand hygiene and less overcrowding should have resulted in a decrease in HAI. However, this was likely offset by the concomitant increase in formula use. Dutta et al. reported a significant decrease in neonatal sepsis during the pandemic (2.5% pre-lockdown v. 1.5% during lockdown, p=0.038) attributed to increased vigilance in hand-washing and wiping of surfaces.[13] In Italy, Indrio et al. found no significant change in the overall incidence of late-onset sepsis in VLBW infants when comparing pre-COVID-19 (2019) with the pandemic (2020) (22.4% v. 17.9%, p=0.177); however, one unit with a high baseline incidence of late-onset sepsis in VLBW infants saw a significant reduction (43.6% v. 26.6%, p=0.030) owing to COVID-19 hygiene measures.[14]
The overall incidence of NEC did not change significantly between pre-COVID-19 and COVID-pandemic periods, which was unexpected. Notably, the incidence of NEC in VLBW infants did not increase significantly during COVID-19, despite the overall increased use of preterm formula compared with pre-COVID-19. An explanation is that infants weighing <1 300 g were preferentially fed DEBM when the mother's own milk was insufficient. However, NEC occurred more often in infants weighing >1 500 g at birth during COVID-Y2 as compared with pre-COVID-19, likely related to increased formula use in this population (infants >1 300 g did not qualify for DEBM). Indrio et al. showed no significant difference in NEC incidence in VLBW infants when comparing pre-COVID-19 with the pandemic (4.6% v. 4.5%, p>0.999).[14] In Indonesia, a study on newborn infants born to COVID-19-positive mothers, found that a higher proportion of infants who developed NEC tested positive for COVID-19 themselves, compared with those who did not develop NEC (40% v. 4.2%, p=0.007).[15] The numbers in this study were small, and more data from larger studies are required to confirm this finding, although other case reports suggesting this association are available. In contrast, all inborn infants in our study born to COVID-19-positive mothers tested negative for COVID-19 after delivery. Other authors have suggested that in-utero COVID-19 exposure is a risk for developing NEC,[16,17] a finding which the current study can neither prove nor disprove.
Effect on admissions and bed occupancy
The decrease in the NMR during COVID-Y1 (35.2 per 1 000 live births) and COVID-Y2 (32.5 per 1 000 live births), compared with pre-COVID-19 (48.9 per 1 000 live births), may partly be attributed to the limited transfer of outborn infants into the unit during the pandemic, which typically includes critically ill infants with higher mortality risk. This contrasts with a study in Nepal that reported a significant increase in the NMR from 13 to 40 deaths per 1 000 live births pre-lockdown and during lockdown, respectively (p=0.002). [18] However, the in-hospital neonatal mortality rate in our study was not significantly different from pre-COVID-19 to COVID-Y1 and COVID-Y2 (127.2 v. 133.0 v. 112.5 per 1 000 neonatal unit admissions, respectively), suggesting that the quality of care did not deteriorate during the pandemic.
The decrease in admissions from 1 195 per year pre-COVID-19 to 880 and 1 040 in COVID-Y1 and COVID-Y2, respectively, was likely secondary to decreased movement across the international and inter-provincial borders during lockdown, as well as the repurposing of the neighbouring hospital as a COVID-19-dedicated hospital with reduced routine maternity services. Outborn infant admissions were also restricted under the hospital's COVID-19 policy, adversely affecting access to tertiary neonatal services and potentially increasing adverse outcomes in the district and surrounding areas. This contrasts with the Indian study that reported a significantly increased proportion of infants admitted during lockdown compared with pre-lockdown (29.2% v. 18.1%, p<0.001), although total admissions decreased slightly (497 admissions v. 474 admissions).[13] Although bed occupancy in our study decreased significantly from pre-COVID-19 to COVID-Y1 (115% v. 103%), it returned to baseline in COVID-Y2 (115% v. 118%). It is important to note that bed occupancy is not only influenced by the number of admissions, but also by the infant's length of stay. This suggests infants were admitted longer in COVID-Y2, possibly owing to healthcare workers discharging infants more readily in COVID-Y1 to reduce mother-infant separation, whereas restrictions on parental visitation were less stringent in COVID-Y2.
Effect on deliveries
The increase in deliveries likely resulted from the closure of the neighbouring hospital's obstetric unit owing to COVID-19 repurposing, highlighting the interdependence of health facilities. This contrasts with other studies which reported a sharp decrease in institutional deliveries by 40% and 52.4% during the COVID-19 lockdown. This was attributed to restricted public transport, movement and the fear of COVID-19 transmission at healthcare facilities.[13,18] The decrease in CS rates in our study may stem from the requirement of a negative COVID-19 test before elective surgery, delaying delivery and possibly resulting in more vaginal births. Additionally, there was an increased risk for theatre staff when performing a CS on COVID-19-positive mothers, hence a preference for vaginal births, where possible. This aligns with a survey from June 2020 that reported a decrease in elective CS among healthy maternity patients in both high- and low-and-middle income countries.[19] Conversely, Ashish et al. reported a significantly higher proportion of women receiving CS during lockdown (24.5% pre-lockdown v. 26.2% during lockdown, p=0.008). [18] The increase in the number of babies born outside the health facility during the pandemic indicates limited access to transport and ambulance services. Ahmed et al. also reported more home births, attributed to fears of leaving home during lockdown, leading to decreased healthcare facility births.[20] This study also showed a reduction in mothers attending ANC during the pandemic,[20] similar to our study.
Study limitations
The present study's retrospective design limited data availability, such as gestational age and feed type for each infant, which were not routinely recorded pre-COVID-19. Additionally, limited administrative staff during the pandemic may have led to underreporting of DEBM use. The study was observational in design, with observed patterns not necessarily implying causation.
Conclusion
Evidence confirms the protective effects of breastfeeding,[21] and the separation of mothers and infants during the pandemic undermined nearly all of the MBFHI recommendations, compromising the protection, promotion and support of breastfeeding in the neonatal unit.
Interruption of breastfeeding and attachment early after delivery can have long-lasting devastating effects. This study highlights the indirect impact of the COVID-19 restrictions, showing increased incidences of HAI, NEC and related deaths in the neonatal unit.
Declaration. During the preparation of this work, the authors used GPT-4o mini in order to edit the manuscript (decrease the word count). After using this tool, the authors reviewed and edited the content and take full responsibility for the content of the article.
Acknowledgements. We thank Mrs I Heyneke and Mrs W Mosana, Department of Dietetics, SBAH, for the stock report for formula purchases and donor milk use, respectively. We are grateful to Ms E Lewis, Department Infection Prevention and Control, for providing bed occupancy data.
Author contributions. MC and UF conceived and designed the research project. MC, RMT, HM and HN acquired relevant data. HM performed data analysis. MC, UF, RMT and HN contributed to drafting the manuscript. All authors approve the final version to be published.
Funding. Funding was received as per the statement below.
Conflicts of interest. UF received a Discovery Foundation grant for the Child PIP mortality audit programme and support from the SAMRC for the Maternal and Infant Health Care Strategies Unit. All funds were paid to the University of Pretoria. UF received payment from the Foundation for Professional Development for participating in the Child Health Module within the Masters of Public Health course. MC, RMT, HN and HM declare no conflict of interest.
References
1. Ramasethu J. Prevention and treatment of neonatal nosocomial infections. Mater Health, Neonatol Perinatol 2017;3 Art. 5. https://doi.org/10.1186/s40748-017-0043-3 [ Links ]
2. Brune K, Donn SM. Enteral feeding of the preterm infant. Neo Reviews 2018;19(11):e645-e653. https://doi.org/10.1542/neo.19-11-e645 [ Links ]
3. Rhoda NR, Velaphi S, Gebhardt GS, Kauchali S, Barron P. Reducing neonatal deaths in South Africa. Progress and challenges. S Afr Med J 2018;108(3a):s9-s16. https://doi.org/10.7196/SAMJ.2017.v108i3b.12804 [ Links ]
4. Rautava S, Luoto R, Salminen S, Isolauri E. Microbial contact during pregnancy, intestinal colonisation and human disease. Nat Rev Gastroenterol Hepatol 2012;9(10):565-576. https://doi.org/10.1038/nrgastro.2012.144 [ Links ]
5. World Health Organization (WHO), United Nations Children's Fund (UNICEF). Implementation guidance: Protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services: The revised baby-friendly hospital initiative 2018. Geneva: World Health Organization (WHO) and the United Nations Children's Fund (UNICEF), 2018. Licence: CC BY-NC-SA 3.0 IGO. https://www.who.int/publications/i/item/9789241513807 [ Links ]
6. The Perinatal Problem Identification Programme (PPIP), version 3.0, Mortality audit data, Tshwane District, Gauteng Province, South Africa. Unpublished data. No URL available. Accessed 8 December 2023. [ Links ]
7. The Vermont Oxford Network (VON), quality improvement database, 2014 - 2024. Unpublished data. https://public.vtoxford.org/. Accessed 3 January 2024. [ Links ]
8. Framework and guidelines for maternal and neonatal care during a crisis: Covid-19 response. Produced by SAMRC and UP Maternal and Infant Health Care Strategies Unit. 22 April 2020. https://knowledgehub.health.gov.za. Accessed 22 January 2024. [ Links ]
9. Ryan L, Plötz FB, van den Hoogen A, et al. Neonates and COVID-19: State of the art. Pediatric Research 2022;91(2):432-439. https://doi.org/10.1038/s41390-021-01875-y [ Links ]
10. Goga A, Feucht U, Pillay S, et al. Parental access to hospitalised children during infectious disease pandemics such as COVID-19. S Afr Med J 2021;111(2):100-105. https://doi.org/10.7196/SAMJ.2021.v111i2.15388 [ Links ]
11. McCleverty. Locked out: The impact of COVID-19 on neonatal care. https://bliss.org.za. Accessed 22 January 2024. [ Links ]
12. Muniraman H, Ali M, Cawley P, et al. Parental perceptions of the impact of neonatal unit visitation policies during COVID-19 pandemic. BMJ Paediatrics Open 2020;4:e000899. https://doi.org/10.1136/bmjpo-2020-000899 [ Links ]
13. Dutta S, Kumar P, Paulpandian R, et al. Relationship between COVID-19 lockdown and epidemiology of neonatal sepsis. Pediatr Infect Dis J 2022;41(6):482-489. https://doi.org/10.1097/INF.0000000000003489 [ Links ]
14. Indrio F, Salatto A, Amato O, et al. COVID-19 pandemic in the neonatal intensive care unit: Any effect on late-onset sepsis and necrotising enterocolitis? Euro J Pediatrics 2022;181:853-857. https://doi.org/10.1007/s00431-021-04254-1 [ Links ]
15. Angelika D, Etika R, Kusumawaedani NN, Mithra S, Ugrasena IDG. Observational study on necrotising enterocolitis in neonates born to SARS-CoV-2-positive mothers. Ann Med Surg 2022;78:10377. https://doi.org/10.1016/j.amsu.2022.103711 [ Links ]
16. Rita R, Aryati, Matulatan. Necrotising enterocolitis in preterm newborn with a history of maternal COVID-19: A case report. Radiol Case Rep 2022;17(8):2630-2634. https://doi.org/10.1016/j.radcr.2022.04.056 [ Links ]
17. Gupta, K, Thakur A, Kler N, Garg P. Gastric perforation and necrotising enterocolitis associated with COVID antibodies. Indian J Pediatrics 2022;89(1):93. http://doi.org/10.1007/s12098-021-03945-9 [ Links ]
18. Ashish KC, Gurung R, Kinney MV, et al. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: A prospective observational study. Lancet Global Health 2020;8(10):e1273-1282. https://doi.org/10.1016/S2214-109X(20)30345-4 [ Links ]
19. Semaan A, Audet C, Huysmans E, et al. Voices from the frontline: Findings from a thematic analysis of a rapid online global survey of maternal and newborn health professionals facing the COVID-19 pandemic. BMJ Global Health 2020;5(6):e002967. https://doi.org/10.1136/bmjgh-2020-002967 [ Links ]
20. Ahmed T, Rahman AE, Amole TG, et al. The effect of COVID-19 on maternal newborn and child health (MNCH) services in Bangladesh, Nigeria and South Africa: Call for a contextualised pandemic response in LMICs. Int J Equity Health 2021;20(1):77. https://doi.org/10.1186/s12939-021-01414-5 [ Links ]
21. Victora CG, Bahl R, Barros AJD, et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016;387(10017):475-490. https://doi.org/10.1016/S0140-6736(15)01024-7 [ Links ]
 Correspondence:
Correspondence:
M Coetzee
mel.coetzee@up.ac.za
Received 29 November 2024
Accepted 18 June 2025

{kind=link}
{kind=link}