










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Health Professions Education
On-line version ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.16 n.3 Pretoria Sep. 2024
https://doi.org/10.7196/ajhpe.2024.v16i3.1559
RESEARCH
A support framework to facilitate social learning and integration skills of fir t-year undergraduate medical students
N Tlalajoe-MokhatlaI; L J van der MerweII; M P JamaIII
IMSc, PhD; Division of Student Learning and Development, Office of the Dean, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIMB ChB, MMedSc, PhD; Division of Health Sciences Education, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIIBCur, MHigher Ed, PhD; Division of Student Learning and Development, Office of the Dean, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: Limited research exists on medical students' coping and adjustment skills, especially in the South African context. Stakeholders planning medical curricula need to be aware of emotional and communication skills that allow students to cope and adjust to stress associated with transitioning to medical studies
OBJECTIVE: To design a support framework to facilitate first-year undergraduate medical students' social learning and integration skills
METHODS: This descriptive qualitative case study used multiple data collection methods, nominal group meetings and Delphi questionnaires to explore and understand undergraduate medical students' challenges with social learning and integration factors. These insights were then used to develop the support framework
RESULTS: The support framework articulates levels of engagement and actions required to address social learning and integrated factors, namely under-preparedness, peer support, confidence, self-management, alienation and academic advice
CONCLUSION: Implementing the proposed support framework on social learning and integration could facilitate the successful transition of first-year undergraduate medical students from high school to university. This framework aids students in dealing with social learning and integrated factors, such as under-preparedness, peer support, confidence, self-management and alienation as well as academic advice using contextualised and appropriate skills and tools
Adapting to a university environment creates stress and uncertainty for students, especially those enrolling immediately after high school.[1] First-year students are most vulnerable to academic withdrawal early in their first semester because the first year is more complicated than the subsequent ones.[2] Also, first-year students experience 'culture shock', loss of confidence and a lack of tacit knowledge of learning expectations within the new environment (i.e. social adjustment issues).[3] A successful transition requires a 'capacity to navigate change'.[2] A lack of research has been reported on medical students' coping and adjustment skills in general, especially in the South African (SA) context.[4] Students are troubled by being away from home, academic pressures and faculty and institution-related challenges.[5] Hence, stakeholders planning medical curricula must know about emotional and communication skills that address stress factors. Such skills will enable students to recognise, understand and manage emotions in themselves and others.[6] Also, medical students can identify issues in themselves and their peers, demonstrating positive coping mechanisms. However, they feel more comfortable sharing those issues among themselves, which leads to low utilisation of available services. Positive coping mechanisms are associated with seeking social support to turn a negative experience into a personal growth experience. Medical students with good social functioning and support are more likely to recover quickly after experiencing difficulties.[7] Little is known about how to facilitate students' social learning and integration. This study investigated factors that affect first-year undergraduate medical students' social learning and integration. Furthermore, we sought experts' opinions on what to include in a support framework to facilitate these students' social learning and integration.
Methods
This study used a descriptive qualitative case study design to explore and understand the meaning individuals or groups ascribe to a social problem.[8] A nominal group technique (NGT) was used to explore and understand factors affecting first-year undergraduate medical students' social learning and integration when transitioning from high school to undergraduate medical studies. A Delphi technique was used to gather expert views in health sciences at higher education and training institutions and refine their judgments on a series of ranked statements collected from various nominal group meetings. This process aimed to achieve consensus on the recommendations proposed in response to which skills must be developed. These two methods allowed for consensus and convergence of opinions[9] and were used to develop a support framework for the social learning and integration of these students.
The social learning[10] and social integration[11] theories were used to ground the study. These two theories were combined to formulate one theory for the study: social learning and integration. This theory is defined as interaction through institutional experiences that can influence how individuals learn from each other through observation, imitation, modelling and persistence.[12] Furthermore, a literature review was conducted to investigate support programmes available to first-year undergraduate medical students and the social learning and integration skills they had to develop to facilitate their transition into the new education environment.[13]
The target population for the NGT was all registered undergraduate medical students from the first to the fifth year. Including senior students allowed rich viewpoints that could indicate a skillset needed in the 1st-year and could further develop with each transition. All registered undergraduate medical students had entered university directly from high school and passed all six modules: The Doctor and the Environment, Concepts of Health and Disease, General Skills, Structure and Development of the Body, Tissues of the Body and Health Psychology. The modules Structure and Development of the Body, Tissues of the Body and Health Psychology are regarded as 'high risk' due to their large content volume and require tutorial support. Furthermore, all registered undergraduate medical students who had initially failed the first semester of entering tertiary education directly from high school were recruited. These students could reapply to enrol in the programme for a second time the following year after completing a Learning Development Programme (LDP). Former LDP students may be considered for re-admission into the main MBChB programme upon successful completion of the LDP modules: Integrated Anatomy and Physiology, Basic Human Anatomy and Physiology, Biophysics and Medical Terminology, achieving an average mark of at least 70%.[4]
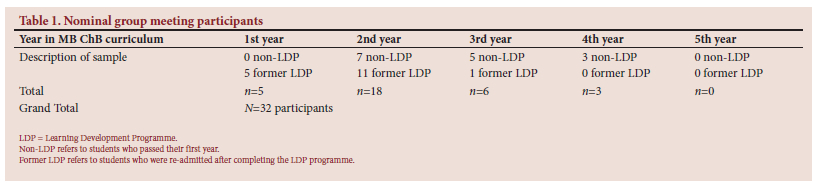
Thirty-two registered medical students who fulfilled the inclusion criteria participated in the NGT (Table 1). Table 1 presents participants in the nominal group meetings. All participants who completed their first year are designated as non-LDP, and those who failed their first year are designated as former-LDP. No limitations were imposed based on sex, ethnicity, home language, living conditions, year of birth and relationship status.[15] Five nominal group meetings were held, each scheduled per most participants' availability. Of the 32 participants who took part in the nominal group meetings, four participants were hosted in the first nominal group meeting during the pilot study. The second nominal group meeting hosted 13 participants from the non-LDP group on 12 April 2019 and the third and fourth nominal group meetings hosted 15 participants on 13 April 2019. During the third and fourth nominal group meetings, the 15 participants were divided into two separate groups: LDP-A (n=8) and LDP-AA (n=7), which ran simultaneously. The two LDP nominal groups were only brought together after they had voted on their top five ranked statements. The fifth nominal group meeting was held for the two small LDP groups in one large group, and they discussed only the top five ranked statements. This was a continuation of the small group meetings that were held separately. The meetings were facilitated using a guide containing the following open-ended questions:
1. What affected your social learning and social integration during your first year of medical studies in the Faculty of Health Science at the University of the Free State?
2. Kindly determine what social learning and social integration skills you used or did not use to help you adapt during the transition from high school to medical education.
The NGT yields data that can be analysed both quantitatively and qualitatively. In this study, analysis was performed as described by Van Breda[16] and McMillan et al.[17] Quantitative data were analysed first. Immediately after the meetings, an overview of each group's ideas was compiled, including the ideas with the highest scores and the number of participants who scored a specific idea. The researcher collected qualitative data from the discussions of statements through text data transcription captured on the flip charts and whiteboards used to record the participants' feedback.
The Delphi technique was the second method used for reaching a general agreement or convergence of opinions on the factors affecting first-year medical students' social learning and integration.[13] Experts in student support at health science and higher education and training institutions nationally and abroad were selected to participate in the Delphi, which focused on recommendations from statements shared during the nominal group meetings. The researcher applied a purposive sampling process, which was based on the belief that the researchers' knowledge about the population could be used to hand-pick the sample population.
The researcher solicited referrals to experts from senior colleagues who suggested suitable participants for this study. After obtaining the list of names, an invitation email was sent out and further engagement followed from the experts' responses. These experts were or had been involved in student support for at least 8 years. A sample of 10 experts was selected to participate in the study. This number was selected to ensure engagement from all participants, facilitating a variety of expert opinions.[18] Of those, six were from the Faculty of Health Sciences and four were from the Department of Higher Education and Training. The Delphi rounds comprised a self-administered questionnaire developed electronically using Microsoft Word 2016. This questionnaire presented a series of ranked and themed statements from the nominal group meetings. Participants were asked to rate these statements on a modified 3-point Likert scale, ranging from 'must-have' to 'good to have' to 'unnecessary'. The participants were requested to write free-text comments that, for example, explained their rating or expressed disagreement with the relevance of themed statements.[13] Consensus was considered to have been achieved on statements when a predetermined threshold of agreement, set at >70%, was reached. The viewpoints of various experts were used as a representation of the overall opinion of the expert group. Following this, participants had the opportunity to reassess and potentially modify their initial ratings for statements in later rounds based on the collective agreement of the group and the input provided by other participating experts.[9] Three rounds were conducted and the participants were requested to make their final submissions on the third round and provide comments about their choices in the free-text comment sections.
The findings from the abovementioned approaches were collated to formulate a support framework for social learning and integration of first-year undergraduate medical students. A framework in the context of this study refers to a basic structure that underlines concepts addressed in this research project. The concepts emphasised the theory of the study, recommendations that achieved consensus and particular actions on how to resolve the identified social learning and integration factors.
The study received ethical approval from the Health Sciences Research Ethics Committee (ref. no. UFS-HSD2018/1300/2711).
Results
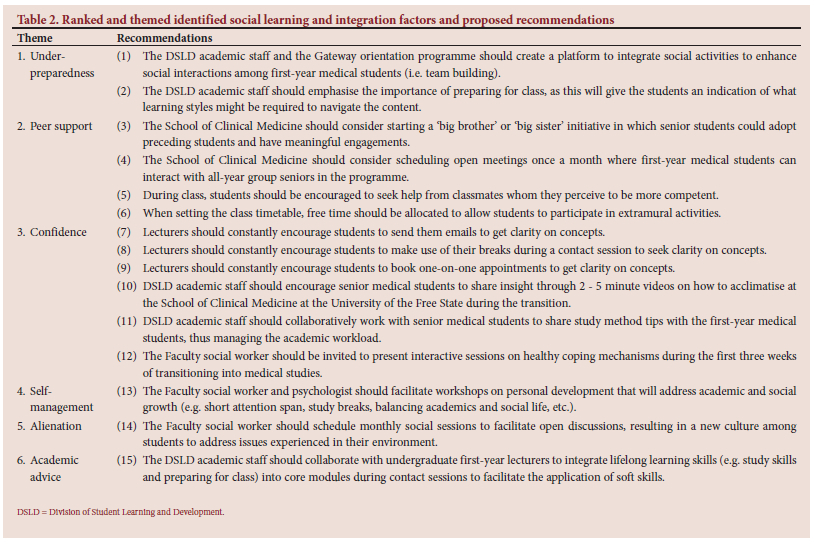
The analysis of findings from the nominal group meeting revealed 15 student recommendations on how the required skills could be developed through certain experiences. The consensus among the medical students who participated in this study was that social learning and integration factors during their transition were affected by six ranked themes: under-preparedness, peer support, confidence, self-management, alienation and academic advice. The medical students further proposed recommendations to respond to each themed statement. Table 2 shows the ranked and themed social learning and integration factors identified by the students, along with the recommendations they proposed for implementation.
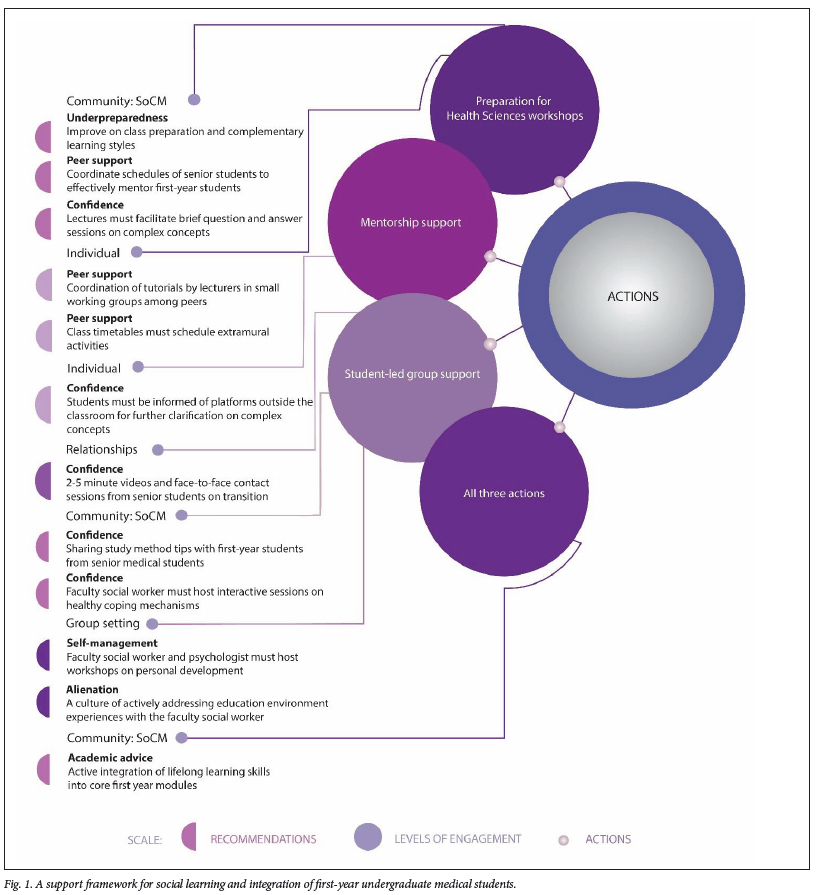
The findings from the Delphi questionnaire highlighted 12 recommendations reaching expert consensus. Emphasis was placed on required skills, free-text comments, key role players and strategies for managing challenges associated with utilising these skills. Levels of engagement were formulated as an umbrella term. From this umbrella term, four basket terms: (i) Community: School of Clinical Medicine (SoCM) level of engagement consists of a workforce team of academic and support staff.
(ii) Individual level of engagement emphasises the personal context during the educational transition. (iii) Group setting enables medical students to learn holistically, not only from their peers but from their education environment too. Finally, (iv) Collaborative relationships were generated. It could be expected to expose individuals to a certain environment such as an academic atmosphere during a collaborative relationship. If they interact with other individuals, relationships - long or short-term - will form (e.g. pairing a senior with a first-year medical student to discuss study approaches to academic work could develop beyond an academic setting and more towards a social setting). These basket terms emphasised the key role players that must participate in overcoming barriers to social learning and integration factors. Complementary to the levels of engagement, the overview of existing literature on support programmes highlighted coping strategies that complemented the recommendations that were suggested by the medical student. In this study, those coping strategies were denoted as actions likely to resolve the identified social learning and integration factors. These actions are contextualised to the findings of this study and are known as preparations for health sciences workshops, mentorship support and student-led group support.
The authors integrated the abovementioned empirical findings in constructing a support framework (Fig. 1). The importance of this framework is the relationship between the levels of engagement and the actions that need to be implemented to address the identified social learning and integration factors that affect the transition from school to university, as mentioned by medical students through the proposed recommendations.
Discussion
The support framework developed in this study is based on social learning and integration theory. The study findings include recommendations that reached consensus, engagement levels highlighted from free text through the Delphi questionnaire and actions highlighted from existing literature. The identified social learning and integration factors underlined were aligned with social learning and integration skills, collectively known as recommendations. A certain level of engagement and corresponding action(s) is needed to address and develop or enhance the lacking skills. The support framework's flow of activities, proposed as coping strategies, are not strictly interdependent, as each addressed theme is a stand-alone, with some overlap. The principal role of the proposed support framework is to facilitate the transition of first-year undergraduate medical students from high school to a new educational environment with newly imparted skills.
The proposed support framework gives a schematic representation of what approaches may be followed in equipping first-year students with social learning and integration skills to ease their transition into a new education environment.
The themed recommendations under the Community: SoCM level of engagement highlight preparation for health sciences workshops by involving community members of the SoCM as a strategy of action in assisting students in better preparing for classes. The expectation from the community: SoCM is to create an academic atmosphere that will allow a collaborative relationship among academic and support staff to function optimally as a collective or individual in developing these skills among first-year students. First-year students lack knowledge on how to prepare for class to the extent that their expectations regarding the time required contrast with the actual time they commit to academic activities.[19]
Peer support can be enhanced through mentorship in preparation for the health sciences workshop. This can be achieved by coordinating schedules among first-year and senior students, facilitated intentionally by the Community: SoCM. Peer mentoring is an effective strategy for developing foundational skills that form part of the cornerstones of improved academic achievement, retention, academic self-efficacy, satisfaction, communication skills and time management as well as providing students with psychosocial support, resulting in enhanced personal satisfaction and well-being.[20] This support framework emphasises the synchronisation of schedules among seniors who mentor first-year students to allow optimal use of these services.
To cultivate confidence among first-year students in academic modules, a suggested approach involves incorporating question-and-answer sessions between the lecturers of the modules and the first-year students during the preparation for health sciences workshops. This technique aims to contextualise intricate concepts and enhance understanding. Tutorials can serve as integrated learning spaces, and a lecturer needs to have a clear picture of the purpose of the tutorial sessions before they can be turned into a learning space.[21] In this study, we agree with Louw's[21] argument and posit that this intervention can enhance students' interaction in large groups, fostering the confidence to ask questions and provide answers in a large class setting.
The themed recommendations under the individual level of engagement also highlight preparation for health sciences workshops as the required actions in facilitating individual social learning and integrated skills development. The emphasised need is for peer support in an academic setting, achieved by facilitating tutorial sessions by lecturers in small working groups. The skill development involves nurturing individuals to shape their interactions with peers and fostering personal growth within the academic environment through social engagement. The small group settings further allow relationship-building among peers and the lecturer. The benefits of these relationships can extend into the large classroom setting.[22] Students are also advocating for the curriculum programme to incorporate extramural activities. The faculty should play a role in scheduling social activities that enable students and staff to interact informally and professionally.[6]
The themed recommendations under the individual level of engagement highlight mentorship support. This support is seen as essential for guiding students to platforms outside the classroom for additional support and clarification on complex content concepts. What is apparent from this finding is the necessity to equip students with tools to engage further with academic content outside an educational setting. This can be implemented through mentorship between academic and support staff and students. Literature indicates that mentoring programmes for first-year students are particularly effective.[23] This study's findings corroborate the literature's conclusions regarding the effectiveness of mentoring programmes.
Furthermore, this study's findings emphasise optimising the effectiveness of mentorship support even more. This implies that, during the selection and allocation process of mentor to mentee, attention should be paid to the type of personality and character of the mentor assigned to a mentee. Selecting mentors based on seniority alone is not necessarily equivalent to competence for effectively mentoring mentee(s).
The themed recommendation under the relationship level of engagement highlights the necessity of student-led group support. This involves collaborating with senior students to provide face-to-face or 2 to 5-minute videos about transitioning into a new educational environment. It also involves nurturing ongoing relationships among students by equipping them with skills to navigate conflict, raise self-awareness and nurture empathy early after arrival in the new educational environment. The student cohort enrolled for medical programmes in the SA context comprises medical students from diverse cultural, socioeconomic and educational backgrounds who vary in language and communication skills.[6,24,25]
Action student-led group further extends to the themed recommendation that requires the Community: SoCM to present seniors with platforms to share module-specific study tips among first-year students. Lifelong learning skills include applying effective learning skills to the health sciences modules during the semester or academic year the student is enrolled. Some skills must be developed sooner than others.[26]
Students also recommended the involvement of social and emotional support through interactive sessions on coping mechanisms within the new environment. Therefore, for students to form student-led groups and sustain them despite the members' diversity, counselling and life coaching must be provided by the faculty social worker and the psychologist to promote skills development in the students in a non-threatening environment. Understanding the factors that foster growth among first-year students is crucial for building training programmes that address the stresses they will encounter in their field practicums and growth opportunities.[27]
The penultimate-themed recommendation also required the action of student-led group support in developing social learning and integration skills for self-management and alienation. In addition to hosting workshops on health coping mechanisms for developing confidence, the request included hosting group settings and exposing students to psychosocial and emotional support workshops in self-management. The same applies to intentionally grouping students (i.e. through personal development workshops) to share experiences on the culture of the education environment. According to the social learning and integration theory, students can learn from each other when they observe and imitate each other within a group setting.[10] Of note is that the individual level of engagement and the group level of engagement complement each other because, within a group setting, different personal contexts also play a role in the interaction of medical students.[28] This indicates that in some instances, one level of engagement could influence the activation of another ,or two levels of engagement could occur concurrently.
The final themed recommendation entails a level of engagement with the community: SoCM, necessitating the effective implementation of all three actions: preparation for health sciences workshops, mentorship support and student-led groups to effectively address this aspect. With this last recommendation, it is essential to note that a collective response from academic and support staff, the students and their educational environment is required to address the integration of lifelong learning skills, also known as graduate attributes. Graduate attributes are the qualities, skills and understanding a university community agrees all its graduates should have developed after completing their university studies. These attributes include and extend beyond the disciplinary expertise or technical knowledge that has been the core of most traditional university courses.[29]
Strengths and limitations
The use of multiple methods of investigation to develop an in-depth understanding of the study and triangulation of the findings strengthened the study.
Since only one group of students at one institution participated, the study cannot be generalised.
Conclusion
A greater understanding of social learning and integration factors, skills and coping strategies was obtained. Implementing the proposed support framework on social learning and integration could facilitate the successful transition of first-year undergraduate medical students from high school to university by aiding them in dealing with social learning and integration factors, such as under-preparedness, peer support, confidence, self-management and alienation as well as academic advice using contextualised and appropriate skills and tools.
Declaration. None.
Acknowledgements. The authors thank the students who participated in this study.
Author contributions. NTM conceptualised the study, collected data and wrote the article. LvM and MJ supervised the execution of the study.
Funding. This study was funded by the National Research Foundation and the Health and Welfare Sector Education and Training Authority.
Data availability statement. The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Conflcts of interest. None.
References
1. Malau-Aduli BS, Adu MD, Alele F, et al. Adjusting to university: Perceptions of ürst-year health professions students. PLOS ONE 2021;16(5):e0251634. https://doi.org/10.1371/journal.pone.0251634 [ Links ]
2. Zhuhra RT, Wahid MH, Mustika R. Exploring college adjustment in first-year Gen Z medical students and its contributing factors. Malays J Med Sci 2022;29(1):126-137. https://doi.org/10.21315/mjms2022.29.1.12 [ Links ]
3. Rickard G, Bramble M, Maxwell H, et al. Exploring the first-year experience in a diverse population: Using participatory action research to explore strategies to support student transition into fast-track undergraduate degree programs. Stud Success 2018;9(4):41-51.https://doi.org/10.5204/ssj.v9i4.653 [ Links ]
4. Hamid S, Singaram VS. Exploring the relationship between demographic factors, performance and fortitude in a group of diverse 1st-year medical students. Afr J Health Prof Educ 2016;8(1):99-103. https://doi.org/10.7196/AJHPE.2016.v8i1.748 [ Links ]
5. Lane B. Beyond academic and social integration: understanding the impact of a STEM enrichment program on the retention and degree attainment of underrepresented students. CBE Life Sci Educ 2016;15(39):1-13. [ Links ]
6. McLean M, Gibbs T. Twelve tips to designing and implementing a learner-centred curriculum: prevention is better than cure. Med Tech 2010;32(3):225-230. https://doi.org/10.3109/01421591003621663 [ Links ]
7. Thompson G, McBride RB, Hosford CC, Halaas G. Resilience among medical students: The role of coping style and social support. Teach Learn Med 2016;28(2):174-182. [ Links ]
8. Creswell J. Qualitative Research Design Choosing among Five Approaches. 3rd edition. Lincoln. SAGE, 2013. [ Links ]
9. McMillan SS, King M, Tully MP. How to use the nominal group and Delphi techniques. Int J Clin Pharmacol 2016;38(3):655-662.https://doi.org/10.1007/s11096-016-0257-x [ Links ]
10. Bandura A. Social learning theory of identificatory process. In D.A. Goslin (Ed.). Handbook of Socialisation Theory and Research. Chicago, IL: Rand McNally & Company, 1969: 213-262. https://scirp.org/reference/referencespapers.aspx?referenceid=1569755 (accessed 10 November 2022). [ Links ]
11. Tinto V. Dropout from higher education: A theoretical synthesis of recent research. Rev Educ Res 1975;45(1):89-125. [ Links ]
12. Tlalajoe-Mokhatla N, van der Merwe L J, Jama M P. Social learning and integration factors affecting first-year medical students: Views of remedial programme students who failed their first year. J Stud Aff Afr 2023; 11(1):65-76. https://doi.org/10.24085/jsaa.v11i1.4271 [ Links ]
13. American Psychological Association. Publication manual of the American Psychological Association. 6th edition. Washington, DC:APA. 2010. [ Links ]
14. Tlalajoe N. A support framework for social learning and integration of first-year undergraduate medical students. Doctoral thesis. 2021.https://scholar.ufs.ac.za/handle/11660/11449 (accessed 10 November 2022). [ Links ]
15. Engelbrecht L, Mostert K, Pienaar J, Kahl C. Coping processes of South African first-year university students: An exploratory study. J Stud Aff Afr 2020;8(2):1-16. https://doi.org/10.24085/jsaa.v8i2.4443 [ Links ]
16. Van Breda AD. Steps to analysing multiple-group NGT data. Soc Work Pract. Res 2005;17(1):1-14. [ Links ]
17. McMillan SS, Kelly F, Sav A, et al. Using nominal group technique: How to analyse consensus across multiple groups. Health Serv Outcomes Res 2014;14(3):92-108. [ Links ]
18. Habibi A, Sarafrazi A, Izadyar S. Delphi technique theoretical framework in quantitative research. Int J Eng Sci 2014;3(4):8-13. [ Links ]
19. Reed DE; Jones G. The importance of first semester seminars for at-risk first-year students: Analysis of student skills and time spent on class preparation. Educ Sci 2021;11:510. https://doi.org/10.3390/educsci11090510 [ Links ]
20. Stone Kelly LE. Peer mentoring in an entry-level occupational therapy program: Student experiences during the COVID-19 pandemic. Open J Occup Ther 2022;10(3):1-15. [ Links ]
21. Louw I. Reclaiming tutorials as learning spaces in the sciences' Mentor. Tutoring: Partnersh Learn 2018;26(3):320-335. https://doi.org//10.1080/13611267.2018.1511952 [ Links ]
22. Epstein M, Draxler B. Collaborative assessment of an academic library and writing centre partnership: Embedded writing and research tutor for first-year students. Coll Res Libr 2020;509-537. [ Links ]
23. Pereira MAD, Barbosa MA. Teaching strategies for coping with stress - the perceptions of medical students. BMC Med Educ 2013;13:50. [ Links ]
24. https://doi.org/10.1186/1472-6920-13-50 [ Links ]
25. Swaminathan A, Viswanathan S, Gnanadurai T, Ayyavoo S, Manickan T. Perceived stress and sources of stress among undergraduate first-year medical students in a private medical college - Tamil Nadu. J Basic Clin Physiol Pharmacol 2015;6(1):9-14. http://www.njppp.com/?mno=202109 (accessed 4 September 2022). [ Links ]
26. Van der Merwe LJ, Van Zyl GJ, St Clair Gibson A, et al. South African medical schools: Current state of selection criteria and medical students' demographic profile. S Afr MJ 2016;106(1):76-81. [ Links ]
27. Hennis, H. Factors influencing the academic performance of first-year students in a medical program. (Unpublished Ph.D. thesis.) Walden University, Minneapolis, Minnesota. 2014. [ Links ]
28. Ben-Porat A, Gottlieb S, Refaeli T, Shemesh S, Reuven Even Zahav R. Vicarious growth among social work students: What makes the difference? Health Soc Care Community 2020;28:662-669. https://doi.org/10.1111/hsc.12900 [ Links ]
29. Hayes AL, Mansour N, Fisher R. Understanding intercultural transitions of medical students. Int J Med Educ 2015;6:26-37. https://doi.org/10.5116/ijme.54e7.b57f [ Links ]
30. Leong R, Kavanagh M. A work-integrated learning (WIL) framework to develop graduate skills and attributes in an Australian university's accounting program. Asia Pac J Coop Educ 2013;14(1):1-14. [ Links ]
 Correspondence:
Correspondence:
N Tlalajoe-Mokhatla
tlalajoen@ufs.ac.za
Received 22 September 2023
Accepted 15 April 2024

{kind=link}
{kind=link}
{kind=link}