










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Health Professions Education
On-line version ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.16 n.3 Pretoria Sep. 2024
https://doi.org/10.7196/ajhpe.2024.v16i3.525
RESEARCH
Obstetrics clinical learning needs: Priorities of undergraduate medical students
T Ntsekhe-MogashoaI; C N NyoniII; M J LabuschagneIII
IMB ChB [0000-0001-7031-5743]; Clinical Skills and Simulation Unit, School of Biomedical Sciences, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIPhD [0000-0001-6229-6984]; School of Nursing, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIIPhD [0000-0001-6273-0736]; Clinical Skills and Simulation Unit, School of Biomedical Sciences, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: The obstetrics clinical learning environment is complex and often not conducive to learning. Understanding the priority clinical learning needs of students with experience in this setting is essential for designing effective educational interventions to optimise clinical learning
OBJECTIVE: To describe the priority obstetrics-related clinical learning needs of undergraduate medical students informed by their experience of the clinical learning environment
METHODS: A multigroup nominal group technique (NGT) was applied to a purposively sampled group of medical students who had experienced obstetrics-related clinical placements in facilities at various levels of care, from primary to tertiary. Individual group priorities were further integrated into themes
RESULTS: Seven priorities emerged: (i) perinatal procedural skills, (ii) teaching approaches to obstetrics, (iii) pregnancy-related screening and complications, (iv) postnatal support for women, (v) interprofessional and gender roles, (vi) orientation to patient care and the clinical environment, and (vii) psychological preparation of students
CONCLUSION: Educational interventions to optimise the obstetrics clinical learning environment must consider students' priorities. These priorities extend beyond procedural skills and include collaborative practice and psychological preparation
The obstetrics clinical learning environment is constantly labelled as hostile and not conducive to learning.[1] The unpredictability and fast-paced nature of activities in this environment, coupled with the dire consequences of malpractice, heightens students' anxiety and negatively impact their learning outcomes.[2] These reported challenges of the obstetrics clinical learning environment add to the well-known difficulties of clinical learning, such as inadequate supervision due to staff shortages, the diversity of patients[3] and competition for patient contact among students from different professions and within the same profession.[4] Health professions education institutions must explore strategies to enhance learning in the obstetrics clinical environment despite existing barriers.
Medical students who rotate through the obstetrics clinical learning environment directly experience the influence of this learning environment on their clinical learning outcomes and therefore are ideally positioned to offer input into the curriculum.[2] Al-Hakeem[5] asserted that students provide valuable input in the development of educational interventions based on their personal experience. In addition, Dennick,[6] who argued for a constructivist approach to curriculum design, emphasised the synergistic interaction between educators, students and the clinical environment where students learn. These authors' arguments underscore the fundamental importance of exploring and understanding students' clinical learning needs to promote optimal learning, especially in a complex clinical environment.
The present study was conducted at a South African (SA) medical school with ~1 000 undergraduate students enrolled in a 5-year programme. The medical school is accredited by the Health Professions Council of South Africa (HPCSA), which sets the standards for medical education in SA. This medical programme is structured into three phases: foundational/introductory (Phase I; 6 months), preclinical (Phase II; 2 years) and clinical (Phase III; 2.5 years), with obstetrics clerkship starting in the final phase. Over a 2-week period, students are required to work with obstetric patients at various clinical sites. Educators assess learning through logbook-completion, written exams and performance exams.[7] While student feedback on the module is provided in evaluations at the end of each 2-week cycle, limited information is gathered about the learning needs of students specifically for the clinical component. However, evidence indicates that students perceive the educational environment at obstetric clinical platforms at the institution negatively.[8] In addition to the students' perceptions of the obstetric clinical learning environment, provincial maternal mortality and morbidity statistics indicate some of these clinical facilities reported the poorest maternal mortality and morbidity outcomes in the country between 2018 and 2020.[9] This suggests that students may be confronted with unusual obstacles in this discipline at these clinical platforms. Currently, it is unclear how the clinical educational experiences of students completing obstetrics clinical clerkships can be optimised.
The obstetrics clinical environment, comprising primary care clinics and hospitals, is characterised by limited resources, staff shortages and a high patient load.[8] Students' experiences in this learning environment illuminate the strengths and weaknesses of such rotations. These experiences may be harnessed to influence the development of an educational intervention aimed at optimising their clinical learning experience. This study aimed to determine the priority obstetrics-related clinical learning needs of undergraduate medical students informed by their experiences of the clinical learning environment.
Methods
A qualitative descriptive research design employing the nominal group technique (NGT)[10] was used. This included a purposively sampled group of 27 out of 127 final-year undergraduate medical students. The NGT is a consensus-building technique that is executed in sequential rounds. The initial round-robin is based on a stimulus topic, in which participants generate ideas individually. Subsequently, discussions aimed at clarifying the generated ideas are made and the final step involves prioritising the generated ideas. The NGT allows for equal participation and provides prioritised immediate results. All participants had undergone clinical rotations in obstetrics at primary care clinics and hospitals. The students were split into four smaller groups for data collection. Data were collected in phases, led by the first author who, after explaining the purpose and process of the study, asked the following question: What do you think you should have learnt before being placed in the obstetrics-related clinical environment during semester six (the second semester of year three in a five-year [10 semesters] programme) of your training?
In the first phase of the NGT, participants recorded their responses individually in writing. Subsequently, these responses were recorded verbatim on a whiteboard in full view of the group members. A discussion ensued aimed at clarifying the responses and removing duplicates of some of the suggestions. In the final phase, each participant had to select five suggestions from the list of previous suggestions they valued most. They were required to rank these suggestions in order of importance, assigning the highest vote of five to their most important suggestion and a vote of one to their least important. The votes were then tallied across the group and the top five suggestions with the highest votes per group were presented. Secondary analysis through thematic analysis was done to combine the priorities across the four groups into themes. The ranking of themes enabled the authors to collate results and identify priority obstetrics-related learning needs across multiple nominal group discussions. Ethics approval for this study was granted by the institutional ethics committee [UFS-HSD 2019/1621/2801].
Results
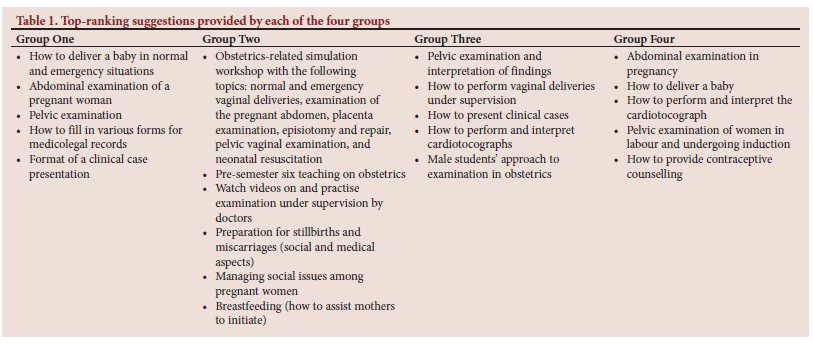
Table 1 presents the top-ranking suggestions from each nominal group discussion listed in order of importance as determined by group votes. Seven themes emerged from the secondary analysis of the data and are presented in order of priority.
Theme 1: Perinatal procedural skills
The perinatal procedural skills represented clinical skills, such as history-taking, examination of the pregnant abdomen and pelvic examination of women who are either in labour or undergoing induction of labour. Other suggestions related to managing normal and complicated deliveries, performing and repairing episiotomies and the management of perineal tears. Participants also mentioned the need to learn about the immediate care and resuscitation of the newborn infant. In terms of communication, they reflected on the need to learn how to deliver bad news to their patients and how to present clinical cases to their supervisors. Lastly, they wanted to know how to complete maternal record booklets.
Theme 2: Teaching approaches to obstetrics
Participants suggested that teaching should incorporate revision of basic sciences and pharmacology relevant to obstetrics. It was also suggested that teaching on obstetric topics should be emphasised in the semester preceding the clinical rotation. Participants believed that learning could be enhanced through digital resources such as videos and that students could benefit from practising skills and procedures under supervision. Clinical simulation was recommended as a teaching approach specifically for physical examination techniques, deliveries and management of obstetric emergencies.
Theme 3: Pregnancy-related screening and complications
Suggestions grouped under this theme pertained to procedures for the identification of pregnancy-related conditions and/or complications. Learning how to perform and interpret side-room tests like urine tests for obstetric patients was a priority, as was the ability to categorise risks such as pre-eclampsia.
Theme 4: Postnatal support for women
The suggestions categorised under this theme focused on learning how to assist women in successfully initiating breastfeeding following delivery and providing contraceptive counselling.
Theme 5: Interprofessional and gender roles
Participants highlighted the need to learn how to work harmoniously with other health professionals. They suggested the need for role clarification ahead of the obstetrics rotation to support students in distinguishing the responsibilities of doctors from those of midwives. In addition, they highlighted the need for male students to learn how to navigate intimate examinations of women.
Theme 6: Orientation to patient care and the clinical environment
This theme related to the orientation of students to protocols and policies concerning professional conduct and managing patients in an obstetrics setting. One suggestion was the need to learn how to manage social issues. Furthermore, participants expressed the need to learn how to apply tuberculosis (TB) and HIV management algorithms in the care of obstetric patients. Additionally, they emphasised the importance of familiarising students with medications typically used in obstetrics. Participants also suggested clarifying whether junior or senior students are given preference regarding patient contact when both groups are working at one clinical site and patient numbers are limited.
Theme 7: Psychological preparation of students
The importance of mental preparation for the obstetrics clinical environment was emphasised. Participants suggested that future students be warned about how stressful the obstetrics environment could be. They suggested that students receive some exposure to childbirth ahead of the rotation as mental preparation for the experience.
Discussion
This study aimed to describe the priority obstetrics clinical learning needs of undergraduate medical students. Experiences from previous obstetrics rotations were used to formulate the clinical learning needs, and through the nominal group technique, priorities could be established and grouped into themes. Four of the listed priorities were aligned to the core learning outcomes related to basic obstetrics.[11] These priorities specifically involved learning procedural skills, pregnancy-related screening and complications, postnatal support of women and the orientation of students to patient care and the clinical environment.
Clarity on students' professional roles, including approaches towards collaborative practice, was highlighted as a priority clinical learning need. Interprofessional education and collaborative practice facilitate teamwork that results in holistic patient care, which is crucial in the obstetrics environment.[2] Ultimately, teamwork relies on clarity regarding professional roles and acknowledgement of the contributions made by individuals from different professions to clinical care. Various undergraduate medical programmes involve the integration of interprofessional education within their mainstream programmes.[12] Using simulated obstetric cases to emphasise role clarification and teamwork could enhance students' understanding of professional roles, consequently optimising clinical learning.
The obstetrics clinical learning environment is complicated and may aggravate anxiety experienced by students.[2] In this study, we found that students valued psychological preparation for obstetrics clinical placement, including specific support needed for male students. Shiner[13] supported the notion of mentally and emotionally preparing students for the clinical environment. Scaffolded high-fidelity simulation activities, engaging students' senses, represent a proximal strategy for preparing them for the clinical setting. In this simulation environment, students benefit from a safe space with guaranteed support from educators, who then debrief them on their learning experiences.[13] It has been reported that students exposed to simulation activities are mentally and emotionally ready to engage with the clinical environment.[12]
The medical students in this study reflected on how they should be taught as a priority clinical learning need. In addition to content sequencing and the inclusion of basic sciences and pharmacology, they further suggested simulation-based education as an essential approach to clinical learning. The curriculum structure of this medical programme follows a traditional approach, with an initial 6-month introductory phase, then a 2-year preclinical phase and then a 2.5-year clinical phase. The preclinical phase is university-based and focuses on basic medical sciences. Teaching and learning activities that integrate basic sciences, including pharmacology, with clinical sciences may be adopted[14] as they have been demonstrated to positively influence students' maturation and engagement in the clinical learning environment.[15,16]
Students are stakeholders in the educational process and educators must investigate and incorporate students' priorities into the design and development of an educational intervention as an essential step to improve clinical learning. Optimising obstetrics clinical learning involves designing an integrated obstetrics educational intervention that prioritises clinical procedural skills and incorporates simulation-based strategies that orientate students into their own professional roles and those of other healthcare professionals within the clinical environment.
Conclusion
By employing the nominal group technique, we described the priorities of obstetrics-related clinical learning needs of undergraduate medical students. These priorities are aligned with students' development in obstetrics and further reflect other essential needs like collaborative practice, gender roles, psychological preparation and approaches to teaching obstetrics. This study was conducted at a single medical school based on students' experiences of the obstetrics clinical learning environment. These students might not represent all medical students in this setting, but their voices were essential in shedding light on the priorities of medical students rotating in obstetrics. Bringing students' voices into the design and development of an educational intervention is an indispensable step in optimising clinical learning.
Declaration. None.
Acknowledgements. The authors acknowledge Prof Yvonne Botma for assisting with the conceptualisation of this work. Daleen Struwig is thanked for her exceptional language editing skills.
Author contributions. TNM, CNN and MJL conceptualised the study, TNM collected the data, TNM and CNN analysed the data and TN, CNN and MJL drafted and revised the manuscript.
Funding. None.
Conflicts of interest. None.
Data availability statement. Data will be made available upon reasonable request.
References
1. Olson HL, Towner D, Hiraoka M, Savala M, Zalud I. Academic clinical learning environment in obstetrics and gynecology during the COVID-19 pandemic: responses and lessons learned. J Perinat Med 2020;48(9):1013-1016. https://doi.org/10.1515/jpm-2020-0239 [ Links ]
2. Rahimi M, Haghani F, Kohan S, Shirani M. The clinical learning environment of a maternity ward: a qualitative study. Women Birth 2019;32(6):e523-e529. https://doi.org/10.1016/j.wombi.2019.01.002 [ Links ]
3. Labuschagne MJ, Nel MM, Nel PPC, Van Zyl GJ. Recommendations for the establishment of a clinical simulation unit to train South African medical students. Afr J Health Prof Educ 2014;6(2):138-142. https://doi.org/10.7196/AJHPE.345 [ Links ]
4. Cotter D, Turner MJ, McAuliffe FM, Higgins MF. Medical students learning experiences of the labour ward: A qualitative research study. Eur J Obstet Gynecol Reprod Biol 2016;206:204-207. https://doi.org/10.1016/j.ejogrb.2016.09.022 [ Links ]
5. Al-Hakeem MMM. Assessment of students' satisfaction on academic environment, clinical skills and examinations in obstetrics and gynaecology course of undergraduate curriculum. Asian J Med Sci 2013;5(1):52-57. https://doi.org/10.3126/ajms.v5i1.8073 [ Links ]
6. Dennick R. Constructivism: Reflections on twenty five years teaching the constructivist approach in medical education. Int J Med Educ 2016;7:200-205. https://doi.org/10.5116/ijme.5763.de1 [ Links ]
7. University of the Free State (UFS). Information guide and outcomes: MBChB III MOBG3823 Semester 6. Bloemfontein, 2019. [ Links ]
8. Schoeman S, Raphuthing R, Phate S, Khasoane L, Ntsere C. Assessment of the education environment of senior medical students at the University of the Free State, Bloemfontein, South Africa. Afr J Health Prof Educ 2014;6(2):143-s149. https://doi.org/10.7196/AJHPE.397 [ Links ]
9. Malakoane B, Heunis JC, Chikobvu P. et al. Public health system challenges in the Free State, South Africa: a situation appraisal to inform health system strengthening. BMC Health Serv Res 2020;20(1):58. https://doi.org/10.1186/s12913-019-4862-y [ Links ]
10. Van Breda AD. Steps to analysing multiple-group NGT data. Soc Work Pract Res 2005;17(1):1-14. https://www.researchgate.net/publication/292746636_Steps_to_analysing_multiple-group_NGT_data (accessed 22 November 2022). [ Links ]
11. Edmonds DK, Lees C, Bourne T. Dewhurst's Textbook of Obstetrics and Gynaecology. 9th ed. Hoboken, NJ: Wiley Blackwell; 2018. [ Links ]
12. Maeno T, Haruta J, Takayashiki A, Yoshimoto H, Goto R, Maeno T. Interprofessional education in medical schools in Japan. PLoS One 2019;14(1):e0210912. https://doi.org/10.1371/journal.pone.0210912 [ Links ]
13. Shiner N. Can simulation impact on first year diagnostic radiography students' emotional preparedness to encounter open wounds on their first clinical placement: A pilot study. Radiography 2019;25(4):294-300. https://doi.org/10.1016/j.radi.2019.04.009 [ Links ]
14. So HY, Chen PP, Wong GKC, Chan TTN. Simulation in medical education. J R Coll Physicians Edinb 2019;49(1):52-57. https://doi.org/10.4997/JRCPE.2019.112 [ Links ]
15. Hafeez A, Jamil B, Khan AF. Roadblocks to integration: Faculty's perspective on transition from traditional to integrated medical curriculum. Pak J Med Sci 2021;37(3):788-793. https://doi.org/10.12669/pjms.37.3.3217 [ Links ]
16. Wijnen-Meijer M, van den Broek S, Koens F, Ten Cate O. Vertical integration in medical education: The broader perspective. BMC Med Educ 2020;20(1):509. https://doi.org/10.1186/s12909-020-02433-6 [ Links ]
 Correspondence:
Correspondence:
C Nyoni
nyonic@ufs.ac.za
Received 29 November 2022
Accepted 15 April 2024

{kind=link}