










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Health Professions Education
On-line version ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.16 n.3 Pretoria Sep. 2024
https://doi.org/10.7196/ajhpe.2024.v16i3.384
RESEARCH
Development of a framework for community health workers to contribute to interprofessional learning teams
A Joubert; M Reid
PhD; Faculty of Health Sciences, School of Nursing, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: Community health workers' knowledge, skills and training seem to affect their contribution to 4th-year health sciences student teams who are following an interprofessional learning programme aimed at improving two South African rural communities' health outcomes related to diabetes
OBJECTIVE: To develop a framework for community health workers to contribute to interprofessional learning teams
METHODS: The framework development forms part of previous phases of a multi-method study. The theory of change logic model guided the development of the draft framework, informed by data from two ecogram sessions, five nominal group technique discussions and a scoping review. The final framework was validated by experts during a workshop using forward and backward mapping
RESULTS: The framework addresses the need for community health workers to gain knowledge, skills and training related to diabetes to effectively contribute to interprofessional learning teams. The theory of change process identified community needs and assets, desired results, influential factors, evidence-based strategies and assumptions required to address the problem
CONCLUSION: The framework focuses on a problem within specific interprofessional learning teams. Collaboration with stakeholders contributed to a rigorous research process, and the validation, refinement and future implementation of the framework. The framework eventually led to the development of an evidence-based training programme comprising knowledge, skills and training strategies related to diabetes. It is predicted that once community health workers have completed this training programme, they will be able to contribute effectively to the interprofessional learning teams
Keywords: Community health workers, diabetes, ecogram, framework, interprofessional learning, nominal group technique, scoping review, theory of change logic model.
In its Global Strategy on Human Resources for Health (HRH): Workforce 2030, the World Health Organization (WHO) relies on countries to ensure that the skills mix of community health workers (CHWs) is diverse and sustainable and that their potential to contribute to interprofessional primary care teams is utilised.[1] Broadly defined, CHWs represent a sub-category of health workers who provide health promotion and prevention services within communities. CHWs are valued for their knowledge of the communities' geographies, cultural norms and healthcare needs.[2] CHWs can contribute to positive health outcomes, and leveraging the potential of various types of CHWs is vital for addressing inequities in access to essential health services in underserved communities.[1]
Positive health outcomes have been achieved through interventions by CHWs and their integration into healthcare programmes. A systematic review conducted by Trump[3] found that 'the main foci across studies' demonstrated a relationship between CHW-delivered interventions and improvements in patients' physical and emotional health, knowledge and self-care behaviours. Other studies confirmed that integrating CHWs into community health programmes positively affected health outcomes.[4,5] Successful CHW interventions require effective service delivery management and a supportive environment, including education.[6]
According to the WHO's recommendation 1A,[7] applying evidence-based models for education is a prerequisite to ensuring CHWs are effective at service delivery. A key message in the guideline on health policy and system support is therefore to optimise community health worker programmes.[7]
In these guidelines, recommendation 1A stipulates a minimum educational level adequate for the task(s) required of CHWs. Recommendation 2 of the WHO outlines criteria for determining the length of CHWs' pre-service training, including their scope of work, responsibilities and roles, required skills and pre-existing knowledge and skills.
Many studies describe the application of evidence-based educational models. Evidence includes culturally tailored diabetes self-management education and support programmes,[8] telehealth[9] and online training.[10] However, in terms of CHWs' scope of work, evidence points to a lack of alignment with important healthcare challenges.[11] Furthermore, although many countries and states recognise CHWs' scope of practice, only a few have established key competencies recognised by legislation.[12]
Regarding types of CHWs, recommendation 12 of the WHO guidelines proposes that CHWs who are equipped with specific skill sets and assigned particular responsibilities can contribute to addressing population health needs.[7] The WHO guideline also lists several implementation considerations for the effective design of CHW initiatives and programmes. These considerations include conducting a sound situation analysis to determine health needs and requirements and ensuring alignment of CHW initiatives and programmes to broader national health and health workforce policies.
The objective of our study was to develop a framework for community health workers to contribute to interprofessional learning teams. This objective is based on the authors' realisation that the knowledge, skills and training of a selected group of CHWs seemed to affect their contributions to interprofessional learning (IPL) teams, which included 4th-year health sciences students representing the schools of Health and Rehabilitation Sciences, Clinical Medicine and Nursing.
These IPL teams follow a programme tailored to improve health outcomes for two South African (SA) rural communities. To complete the IPL programme, teams require a certain scope of knowledge, skills and training. The programme involved: the screening of adult patients diagnosed with diabetes mellitus using tools such as the depression, anxiety and substance abuse scales; a 60-second foot screening checklist and the International Classification of Functioning, Disability and Health assessment, to determine the patients' health status. Data obtained through these screenings were captured electronically by the IPL teams and then used to structure health education sessions and activities to promote a healthier lifestyle among patients with diabetes.
The CHWs in our study were members of the community and therefore had an in-depth understanding of the community they serve.[13] Their role was limited to notifying the patients that students would be visiting them and providing students with directions to the patients' houses. In this setting, CHWs' contribution to the health outcomes of patients with diabetes was ill-defined. To expand these roles within the context of this IPL, the authors presupposed that CHWs required certain knowledge, skills and training related to diabetes. Therefore, this article aims to develop a framework for community health workers to contribute to IPL teams.
Methods
The development of the framework is the outcome of data gathered and extrapolated through a broader multi-method study (UFS-HSD2019/1079/2708) that aimed to support CHWs through IPL. These methods offer detailed descriptions of data collection, interpretation and presentation of the results,[14] while applying a theory of change logic model illustrates the framework's development.[15] Previous phases included two ecograms, five nominal group technique (NGT) discussions and a scoping review. The ecogram technique discussions conducted with the CHWs aimed to describe the available support structures for them (authors, unpublished). The five NGT discussions involving CHWs, students and facilitators aimed to outline the contributions of CHWs to IPL teams in terms of their knowledge, skills and training.[16] The scoping review[17] provided an evidence-based approach to the development of the framework. Data triangulated from these previous phases were used to populate the framework. A group of experts validated the proposed framework during a member-checking workshop.
Theoretical underpinning of the framework
A logic model is a systematic and visual means to communicate one's insight into the connections between resources or inputs available to manage a programme.[15,18] The model illustrates one's planned activities and envisioned results through steps, such as planned actions, outputs, outcomes and impact.[15,18] Using logic models as a tool requires systematic thinking and planning related to programme design and ongoing reviews to address changes.[18] A logic model serves as an instrument to facilitate programme design by illustrating a programme's key concepts. It enables stakeholders to apply best-practice research and leverage their practitioner expertise, while also facilitating critical reflection on aspects important for programme monitoring, reporting and adjustments.[18] Additionally, logic models help in identifying gaps in the theory or logic of a programme, engaging stakeholders in design processes and creating a platform to understand the programme's focus and the interrelationships among its components.[15,18] According to Anderson et al.,[15] conceptual models and causal diagrams can potentially contribute to transparency in systematic reviews and are therefore convincing to decision-makers. Approaches to logic models include either a theory, outcomes or an activities approach model.[18] The theory of change logic model provided us with a valid reason to explore the idea of a framework for CHWs to contribute to IPL teams.[18] The following section contains a brief description of the research techniques or methods that were applied to reach the objectives that were stated in the previous phases of the multi-method study. Excerpts of data that were available to develop the framework are also provided.
Empirical foundation of the theory of change logic model framework
We applied the ecogram and nominal group techniques to gather relevant data, while the scoping review addressed core concepts related to the study.[16,17] A theory of change logic model underpinned the framework validation workshop.
The ecogram, nominal group discussion and scoping review
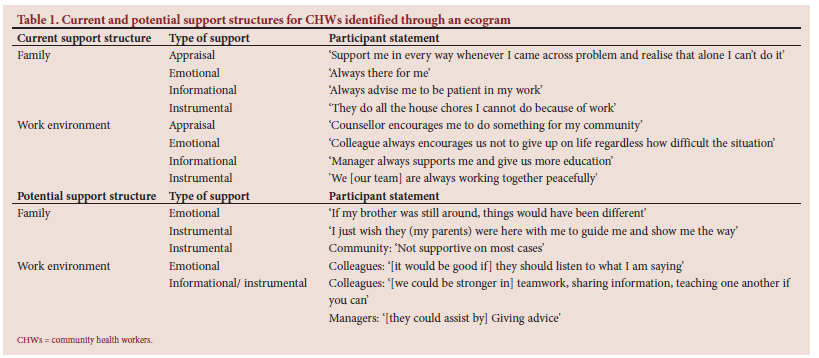
An ecogram, described as qualitative in nature and a 'concrete clinical method', is a suitable technique for appreciating people in their environments.[19] A purposive sampling method led to the inclusion of 26 CHWs from two rural towns who consented to participate. CHWs were specifically selected to participate to determine the types of support that could be included in the framework. Before completing their ecograms, CHWs signed informed consent forms and received an information leaflet outlining the steps to be followed during the data-gathering session. Sheets of paper and coloured pens were handed to the participants. They were asked to write down the people, organisations or systems that support them and those they think could support them in the future. Firstly, the CHWs' feedback was individually presented as a drawing that consisted of circles, with each circle presenting either support received or potential support that could benefit them. This step was followed by a group discussion to allow CHWs to elaborate on the support depicted in their ecograms and for the researchers to accurately capture each participant's feedback regarding the available support structures. We selected the thematic analysis approach proposed by Clarke and Braun[20] to structure the data. Excerpts of the current and potential support structures, types of support and verbatim transcripts of participants' statements that emerged from the analysis are presented in Table 1. The support structures included family and the work environment. Appraisal as a type of support involves facilitating decision-making, providing appropriate feedback and assisting in determining a course of action; emotional support refers to rendering care and showing empathy, love and trust; informational support refers to providing information during times of stress and instrumental support involves any actions taken to assist a person with problem-solving by providing help or information.[21]
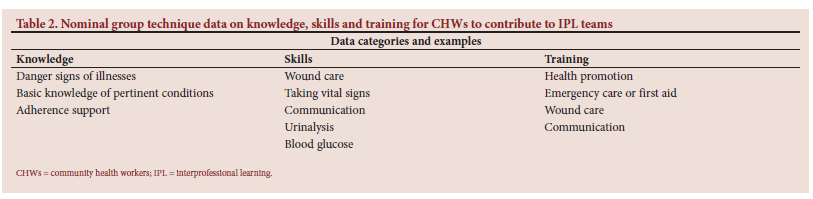
A nominal group discussion, described as a qualitative consensus-seeking method, lends itself to developing problem-solving strategies.[22] To ensure valid and reliable data, nominal group discussions require groups of at least 10 participants.[23] The nominal group discussions that followed a specific procedure were conducted after purposive sampling of 56 participants. The participants, two CHWs groups, two interprofessional learning student groups and a group of IPL facilitators and coordinators, were requested to identify the knowledge, skills and training CHWs require to contribute to IPL. An analysis of the multiple-group data was conducted.[16,22,24] Table 2 depicts the final top priority related to knowledge, skills and training indicated by each of the five groups. Priorities were determined by applying several steps to calculate and organise scores.[22] In terms of training, two groups identified health promotion as the top priority.
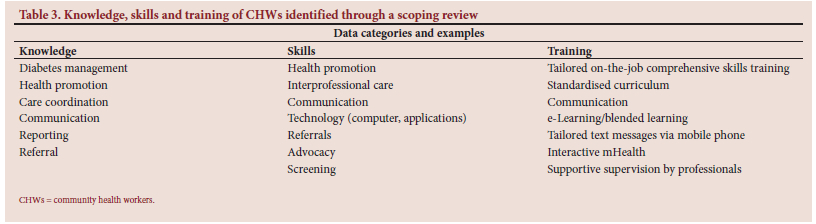
Scoping reviews, a relatively new approach to evidence synthesis, are suitable to demarcate the extent of literature coverage on the topic being investigated. These reviews provide an indication of the literature available and the scope or focus related to the review topic.[25] The key to conducting scoping reviews is the mapping of identified evidence.[25] We conducted an extensive electronic database search on the EBSCOhost platform from 1 January 2009 - 03 February 2020, to map the literature related to the research question: What is known about the knowledge, skills and training of CHWs to contribute towards interprofessional learning? The search concepts were: community health workers, interprofessional, knowledge, skills and training. The electronic search yielded 2113 results. Of those, 32 studies were suitable for analysis.[17] Excerpts of the results are presented in Table 3.
In this study, our framework, underpinned by the theory of change logic model, was populated using data triangulated from the abovementioned phases and validated during a face-to-face workshop and online discussions.
Framework development and validation
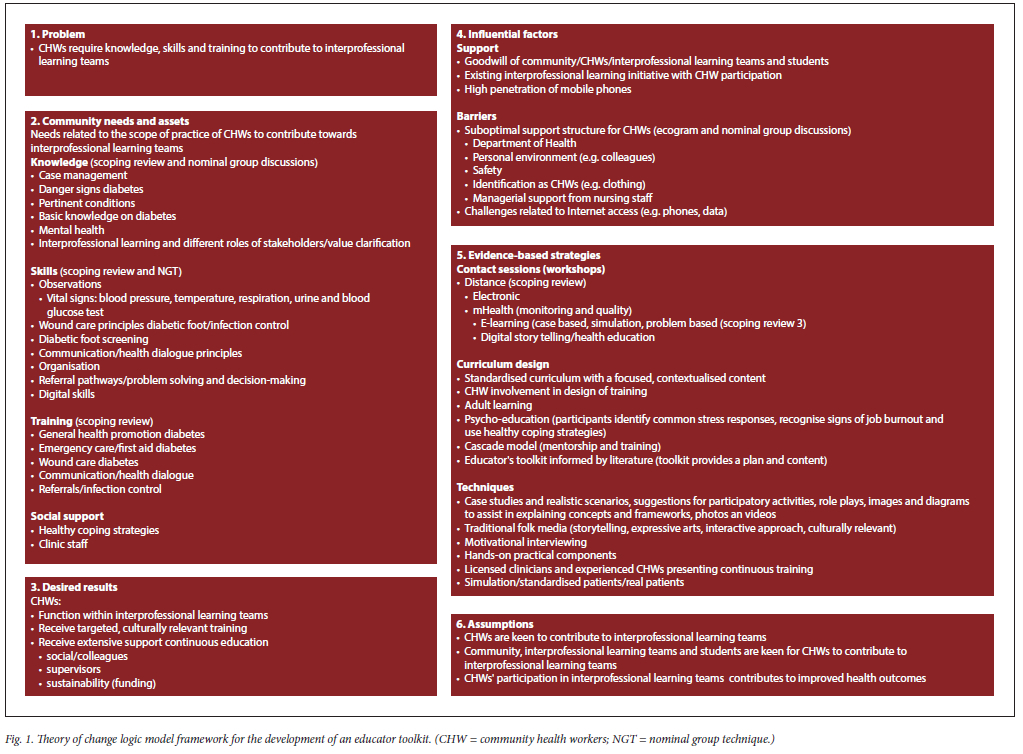
We applied the aspects involved, including the identified problem, community needs and assets, desired results, influential factors, evidence-based strategies and assumptions depicted in the logic model to develop our draft framework (Fig. 1). We used data collected from the ecogram, the nominal group discussion and the scoping review to populate this framework.[16,17] A purposive selection of stakeholders resulted in the inclusion of experts/peers in the field of framework development and people knowledgeable about the research topic. While adhering to COVID-19 regulations, we implemented alternative strategies to validate our draft framework. First, a face-to-face workshop that involved only six stakeholders was conducted. Second, two stakeholders provided input through a spoken conversation via the Skype software application as an online platform. In both cases, we used PowerPoint to present the logic model and our draft framework. Stakeholders were requested to add to the draft framework based on their expert knowledge to enrich the validated framework. The process we followed allowed us to use checking questions, such as 'How did we get here?' and ' Why is there a connection between certain components within the model?'. The process of forward and backward mapping was concluded once data saturation was noted.[18] Finally, feedback from stakeholders was added, and our framework was adjusted accordingly. The final framework contained evidence of data collected through stringent research processes and depicts the input of stakeholders in the validation group (Fig. 1).
Methodological rigor
Rigor was enhanced through extensive planning and execution of our study.[26] For example, we ensured the qualitative validity of our framework by applying key criteria: credibility (truth value/internal validity), transferability (generalisability/external validity), dependability (consistency/reliability) and confirmability (neutrality/objectivity).[26] We also employed multiple procedures, including data triangulation, member checking and peer reviews.[14,27]
Credibility: truth value/internal validity
Credibility addresses the coherence between participants' feedback and the researcher's depiction of it.[28] Truth value, embedded in credibility, is how researchers convince themselves and others that their research findings are noteworthy.[28] Internal validity aims to prove that the description of research data is supported by accurate data and the research itself.[14,26] Internal validity encompasses truth value and credibility.[26] We used the following strategies to guarantee the accuracy of our findings and to convince readers of their truthfulness.[14] First, we based our draft framework on rigorous research processes, analysing data obtained through the ecogram, nominal group technique and scoping review, along with the detailed descriptions of findings related to these research techniques.[27,28] Second, we increased credibility by comparing our initial findings with the raw data, performing data triangulation, and involving stakeholders in validating our findings.[28] Data triangulation involves using evidence from multiple sources and methods to validate the accuracy of a study.[14,26,27] Lastly, we applied member checking or participant endorsement to explore and establish the credibility of our research findings.[27] We included participants and topic experts to validate the framework. The topic experts served as an external check, providing insights from people who are knowledgeable about the phenomenon being explored.[27]
Transferability: generalisability/external validity
According to Nowell et al.,[28] transferability refers to the generalisability of inquiry. While it is impossible to predict how other researchers may opt to apply our findings, the detailed descriptions of our research processes and findings could help them in evaluating the transferability to specific sites.[28]
Dependability: consistency/reliability
Dependability or reliability is 'the ability to obtain the same results if the study were to be repeated'.[29] The dependability of our research was enhanced through the stringent application of research principles, sharing of data analysis and interpretation by more than one researcher, along with clear documentation of the results.[14,28] Applying the aspects depicted in the logic model contributed to our confidence that the content projected in our framework is reliable (Fig. 1).
Confirmability: neutrality/objectivity
Confirmability concerns establishing that the researchers' interpretations and conclusions were deduced from the data and that the researcher demonstrates how these interpretations and conclusions were reached. Therefore, confirmability is achieved when credibility, transferability and dependability are attained.[28] We applied both inductive and deductive reasoning to derive sound interpretations and conclusions. The theory of change was a suitable model for populating our framework.
Ethical endorsement
We adhered to the principles stated in the Nuremberg Code of 1947, the Declaration of Helsinki (1964) and the three fundamental ethical principles of respect for persons, beneficence and justice.[30] Ethical principles we applied included obtaining permission from different stakeholders to conduct the study, negotiating to enter the research settings, obtaining informed consent from participants, allocation codes to mask participants' personal information and providing constant feedback to participants regarding the interpretation of data and conclusions.[26-28] We addressed possible bias through a detailed description of the research design, obtaining ethical approval to conduct the study and doing member-checking of the interpreted data.[27]
Discussion
A theory of change logic model is developed based on extensive thoughts and ideas underlying the conceptualisation of a programme.[18] Applying a systematic approach based on theory, including qualifying the problem related to CHWs' knowledge, skills and training, specifying our selected
community's needs or assets and identifying the vision for our CHWs programme, resulted in a visual presentation and master plan for the development of the educator toolkit related to CHWs. The problem depicted in the framework originates from; i) our experience of working with CHWs as contributors to specific IPL teams, ii) collaborating with international funders to address support required by CHWs to contribute to IPL and iii) issues noted as part of our rigorous research described in this article. In our framework, we depict CHWs as the 'community'. The needs and assets therefore relate to CHWs' knowledge, skills and training, enabling them to contribute to IPL teams. An important asset was the support CHWs received from family, friends, the church community, government structures and colleagues. Influential factors, classified as either support or barriers, are closely linked with achieving the desired results noted in this framework. The high penetration of mobile phones among these CHWs was an important asset that facilitated their participation in IPL. However, this asset was counteracted by the challenge of affording internet access, particularly data costs. The desired results include CHWs contributing effectively to IPL teams, receiving targeted, culturally relevant training and receiving extensive support in terms of continuous education.
To achieve the desired results, we classified our evidence-based strategies into three main areas: i) communication: including contact sessions, distance education through mHealth, videoconferencing and eLearning; ii) curriculum design: standardised curricula, CHWs' involvement in the design of training and adult learning and iii) techniques: case studies and scenarios, role-playing, traditional folk media, motivational interviewing, hands-on practical components and licensed clinician and experienced CHWs presented training. Ultimately, our assumptions hinge on several cause-effect relationships addressed in our framework: that CHWs were keen to contribute to IPL teams, that the community, IPL facilitators and students support CHWs' involvement in IPL teams and that CHWs' participation in IPL teams will contribute to improved health outcomes (Fig. 1).
Study limitations
Due to the contextual nature of the framework, the generalisability of the theory of change logic model framework can only be determined if other researchers decide that the content of this framework is suitable for application to their settings.
Conclusions
This article offers the development of a framework for community health workers to contribute to IPL teams. The framework is based on the need for CHWs to acquire knowledge, skills and training to contribute to specific IPL teams. First, input from stakeholders contributed to validating and refining the framework. Among the valuable suggestions made by stakeholders was that CHWs should not become paraprofessionals. It was also suggested that they should have a clear understanding of interprofessional collaboration and how the roles of stakeholders are interlinked to ensure improved health outcomes. Second, applying the theory of change logic model provided us with the necessary evidence-based strategies to apply another stage of our research (not described in this article) to develop an educator training programme related to diabetes. Among these strategies, implementing simulation and using either standardised or real patients is worth considering when developing similar training programmes. Lastly, we predict that CHWs, equipped with targeted and culturally relevant training, will be keen to contribute to IPL teams and that these teams will value their involvement in achieving health outcomes. However, to ensure that CHWs' contribution to IPL teams is sustainable, efforts to provide continuous education and supportive supervision remain vital. Future research should focus on integrating CHWs into IPL teams.
Declaration. None.
Acknowledgements. The authors would like to acknowledge Vlir'Uos for their contribution towards Community Health Workers' engagement.
Author contributions. MR and AJ collaboratively conceptualised and conducted the study, that is, determined the methodology and participated in the collection, analysis and interpretation of data, and preparing final the manuscript.
Funding. None.
Data availability statement. The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Conflicts of interest. The authors declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
References
1. World Health Organization. Guideline Development Group (GDG) convenes in Geneva for its first meeting on WHO guidelines on policy and system support for community-based health worker programmes. WHO, 2016. https://www.who.int/news/item/25-10-2016-guideline-development-group-(gdg)-convenes-in-geneva-for-its-first-meeting-on-who-guideline-on-policy-and-system-support-for-community-based-health-worker-programmes (accessed 4 May 2022). [ Links ]
2. O'Donovan J, O'Donovan C, Kuhn I, et al. Ongoing training of community health workers in low-income and middle-income countries: A systematic scoping review of the literature. BMJ Open 2018;(8):e021467. https://doi.org/10.1136/bmjopen-2017-021467 [ Links ]
3. Trump L. An alternative approach to Type 2 diabetes care: The inclusion of community health worker interventions in patient care. Minnesota Digital Conservancy, 2017. https://hdihandle.net/11299/188880 [ Links ]
4. Alaofè H, Asaolu I, Ehiri J, et al. Community health workers in diabetes prevention and management in developing countries. Annals Glob Health May-Aug 2017;83(3-4):661-675. https://doi.org/10.1016/j.aogh.2017.10.009 [ Links ]
5. Dos Santos A de F, da Rocha HA, de Lima ÂM, et al. Contribution of community health workers to primary health care performance in Brazil. Revista de Saúde Pública 2020;54(143). https://doi.org/10.11606/s1518-8787.2020054002327 [ Links ]
6. Schmidt B, Campbell S, McDermott R. Community health workers as chronic care coordinators evaluation of an Australian Indigenous primary health care program. Aust NZ J Public Health 2016;40(Suppl 1):S107-S114. https://doi.org/10.1111/1753-6405.12480 [ Links ]
7. World Health Organization. Guideline on health policy and system support to optimise community health worker programmes. Geneva: WHO, 2018. [ Links ]
8. Creason J, Axelrod C, Conneely MM, et al. A community health worker-led educational intervention for Latinos with T2d diabetes. Diabetes 2020;69(Supplement-1):645-P. https://doi.org/10.2337/db20-645-P [ Links ]
9. Keegan CN, Johnston CA, Cardenas VJ Jr, Vaughan EM. Evaluating the impact of telehealth-based, diabetes medication training for community health workers on glycemic control. J Pers Med 2020;10(3):121. https://doi.org/10.3390/jpm10030121 [ Links ]
10. Yeary KHK, Ounpraseuth S, Wan F, et al. Assessing the feasibility of an online training designed to enable community health workers to deliver a comprehensive, evidence-based weight loss intervention for rural African Americans of faith. J Canc Educ 2021;36(6):1277-1284. https://doi.org/10.1007/s13187-020-01764-8 [ Links ]
11. Majee W, Anakwe A, Johnson L, Rhoda A, Frantz J, Schopp L. A self-management training intervention: Perceptions and practices of community health workers in South Africa. Health Promot Pract 2020;21(6):983-992. https://doi.org/10.1177/1524839918820038 [ Links ]
12. Corder-Mabe J, Johnson S, Mazmanian PE, Smith WR. Development of a framework to describe functions and practice of community health workers. J Contin Educ Health Prof 2019;39(4):265-269. https://doi.org/10.1097/CEH.0000000000000274 [ Links ]
13. Malcarney M-B, Pittman P, Quigley L, Horton K, Seiler N. The changing roles of community health workers. Health Serv Res 2017;52(1);PartII:360-382. https://doi.org/10.1111/1475-6773.12657 [ Links ]
14. Creswell JW, Creswell JD. Research Design. Qualitative, Quantitative, and Mixed Methods Approaches. 5th ed. Los Angeles: Sage, 2018. [ Links ]
15. Anderson LM, Petticrew M, Rehfuess E, et al. Using logic models to capture complexity in systematic reviews. Research Synth Methods 2011;2(1):33-42. https://doi.org/10.1002/jrsm.32 [ Links ]
16. Joubert A, Reid M. Knowledge, skills, and training of community health workers to contribute to interprofessional education: A scoping review, J Interprof Care 2023;38(2):308-318. https://doi.org/10.1080/13561820.2023.2176472 [ Links ]
17. Joubert A, Reid M, Knowledge, skills, and training of community health workers to contribute to interprofessional education: A scoping review, 2023. [ Links ]
18. Kellogg Foundation. Logic model development guide. Battle Creek, MI: Kellogg Foundation, 2004. http://www.compact.org/wp-content/uploads/2010/03/LogicModelGuidepdf1.pdf [ Links ]
19. Jasui M, The cultural ecogram: A tool for enhancing culturally anchored shared understanding in the treatment of ethnic minority families. J Ethnic Cultural Div Soc Work 2015;24(Issue 2):89-108. https://doi.org/10.1080/15313204.2014.991980 [ Links ]
20. Clarke V, Braun V Teaching thematic analysis: overcoming challenges and developing strategies for effective learning. Psychol 2013;26(2):120-123. [ Links ]
21. Gale NK, Kenyon S, MacArthur C, Jolly K, Hope L. 'Synthetic social support: Theorizing lay health worker interventions, Soc Sci Med 2018;196:96-105, https://doi.org/10.1016/j.socscimed.2017.11.012 [ Links ]
22. Roets L, Lubbe I. Power imbalances in research: A step by step illustration of an adapted multiple nominal group analysis, Int J Arts & Sci 2015:8(5):151-164. [ Links ]
23. Olsen J. The nominal group technique (NGT) as a tool for facilitating pan-disability focus groups and as a new method for quantifying changes in qualitative data. Int J Qual Methods 2019;18:1-10. https://doi.org/10.1177/1609406919866049 [ Links ]
24. Van Breda AD. Steps to analyzing multiple-group NGT data. The Social Work Practitioner Researcher 2005:17(1):1-15. [ Links ]
25. Munn Z, Peters MDJ, Stern C, Tafanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 2018;18:143. https://doi.org/10.1186/s12874-018-0611-x [ Links ]
26. Cohen L, Manion L, Morrison K. Research methods in education. Eighth edition. Taylor & Francis, London; 2018. [ Links ]
27. Creswell JW, Poth CN. Qualitative Inquiry and Research Design. 4th ed. Sage, 2018. [ Links ]
28. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria international J Qual Methods 2017;16:1-13. https://doi.org/10.1177/1609406917733847 [ Links ]
29. Morse JM. Critical analysis of strategies for determining rigor in qualitative inquiry. Qual Health Res 2015;25(9):1212-1222. https://doi.org/10.1177/1049732315588501 [ Links ]
30. Brink H, van der Walt C, van Rensburg G. Fundamentals of Research Methodology for Healthcare Professionals. 3rd ed. Cape Town: Juta, 2012. [ Links ]
 Correspondence:
Correspondence:
A Joubert
dr.ajoubert@outlook.com
Received 1 November 2022
Accepted 15 May 2024

{kind=link}
{kind=link}
{kind=link}
{kind=link}