










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Health Professions Education
On-line version ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.16 n.3 Pretoria Sep. 2024
https://doi.org/10.7196/ajhpe.2024.v16i3.1625
RESEARCH
Unani Tibb students' and educators' perceptions of spirituality and spiritual care in education in South Africa: A mixed-methods study
M HoosenI; N V RomanII; T G MthembuIII; M NaseerIV
IMSc; School of Natural Medicine, Faculty of Community & Health Sciences, University of the Western Cape, Cape Town, South Africa
IIPhD; Centre for Interdisciplinary Studies of Children, Families and Society, Faculty of Community and Health Sciences, University of the Western Cape, Cape Town, South Africa
IIIPhD; Department of Occupational Therapy, Faculty of Community and Health Sciences, University of the Western Cape, Cape Town, South Africa
IVMD; Department of Moalejat, Ajmal Khan Tibbiya College, Faculty of Unani Medicine, Aligarh Muslim University, Aligarh, India
ABSTRACT
BACKGROUND: Unani Tibb promotes holistic patient care, yet spirituality and spiritual care seem to be neglected in education. This theory-practice gap was previously highlighted in studies on Unani Tibb practitioners. The role of spirituality and spiritual care in Unani Tibb education in South Africa (SA) remains unclear
OBJECTIVES: To explore Unani Tibb students' and educators' perceptions and attitudes of spirituality and spiritual care in SA
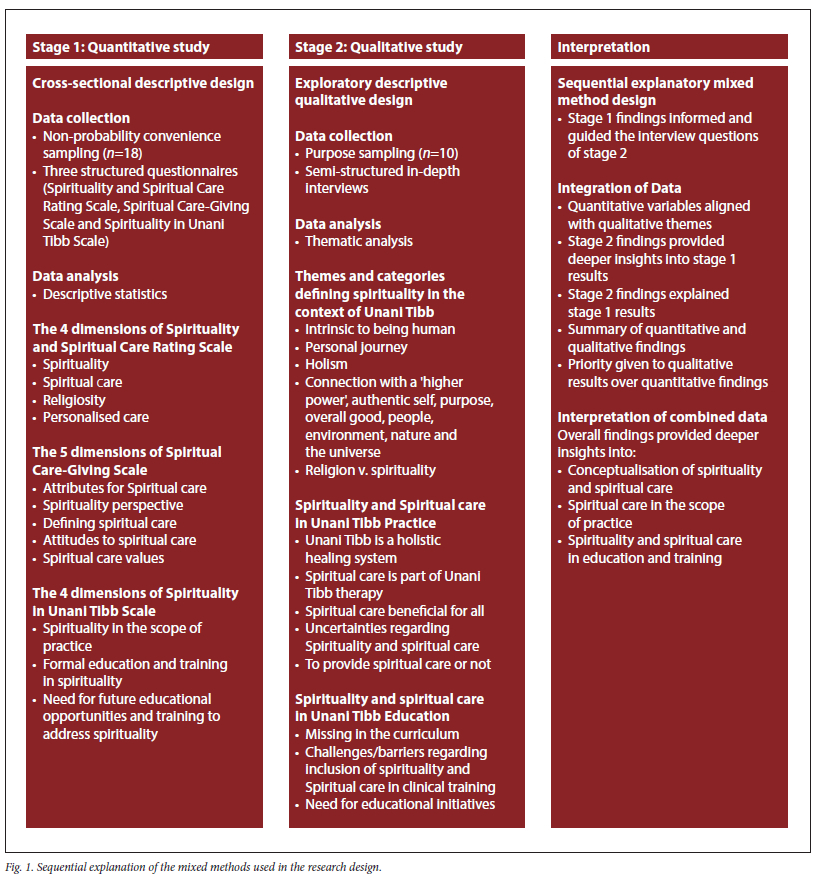
METHODS: A two-stage sequential explanatory mixed-method study was conducted. Quantitative data from stage 1 was obtained using a cross-sectional descriptive study followed by in-depth interviews for the qualitative study in stage 2. Stage 1 guided the interview questions in stage 2. Descriptive data analysis was performed for the quantitative study, followed by thematic analysis for the qualitative data
RESULTS: A total of 18 (90%) participants took part in the quantitative study followed by 10 participants (50%) in the qualitative study. Three study findings emerged: i) a heightened level of spiritual awareness was recorded for this cohort despite the lack of spirituality and spiritual care content in the curriculum, ii) participants viewed spiritual care as integral to Unani Tibb philosophy, education and practice and iii) formal integration of spirituality and spiritual care concepts in Unani Tibb education was identified as a necessity to ensure the integrity of the holistic approach required by the profession
CONCLUSION: This study has implications across the health education sector and more specifically for Unani Tibb educators to consider the inclusion of spiritual care content in education programmes
Keywords: Unani Tibb, student, educator, spirituality, spiritual care, education, mixed methods.
Spirituality and complementary and alternative medicine (CAM) are interconnected and integral to all communities globally.[1,2] Spirituality is a fundamental tenant of CAM, often discussed in the context of holistic care.[3-5] CAM systems, such as African traditional medicine and Unani Tibb, are utilised by millions and deeply rooted in many cultures and traditions.[1,2] In Africa, up to 80% of people rely on CAM for their healthcare needs.[2,5] In SA, several forms of CAM, like Unani Tibb, have been included in university curricula for health profession students.[1,2,5] Unani Tibb is a widely accepted form of CAM practised in many of the World Health Organization (WHO) member states, including SA.[2,5-7] A large proportion of the SA population uses CAM products and services.[5,8,9] These include medication of plant, animal or mineral origin, manual body therapies, such as cupping, massage and acupuncture, as well as spiritual therapies like prayer medicine, meditation and yoga. [2,5,8,9] Therefore, patients associate spirituality with CAM and expect spiritual care from Unani Tibb practitioners.[5,8,9] However, Unani Tibb practitioners reported that they were not adequately skilled in the area of spirituality and spiritual care owing to the lack of formal training on these specific topics.[2,5,9]
There are positive associations between spirituality, individual healthcare outcomes and quality of life.[2,4,5,8-10] Koenig[10] provides a comprehensive review of the relationship between religion/spirituality and mental and physical health. Some of the positive outcomes for mental health reported include happiness, wellbeing, hope, optimism, meaning and purpose, high self-esteem, a sense of control over life and gratefulness. Better physical health outcomes were reported for several disorders, including cardiovascular, cerebrovascular, endocrine and immunological disorders.[10] For this reason, the topic of spirituality and spiritual care is firmly fixed within the healthcare agenda in most healthcare professions. It is expected by healthcare authorities that healthcare professionals increase their competence in spirituality as part of healthcare services.[12,13] However, studies report that spirituality remains neglected in healthcare education.[14,15] Mthembu et al.,[14,15] reported on the relevance and importance of spirituality in health education and its applicability to the needs of society. The response of medical schools includes adapting education and practices to address the new realities of the world. Healthcare training institutions are advised to adopt an integrative, transformative, collaborative and interdisciplinary approach towards the training of health science graduates in the field of spirituality and spiritual care.[14] There is growing interest in the field of spirituality and spiritual care in most healthcare education settings.[11] However, this is not the case for CAM education,[2-4] specifically Unani Tibb education, in SA.[2,5,9]
Research on spirituality and spiritual care in Unani Tibb is extremely rare.[2,5,9] In a multi-site exploratory study, Unani Tibb practitioners, among other CAM professionals, agreed that spirituality was a key area of concern for their patients during illness. In this study, Unani Tibb practitioners advocated for the inclusion of spirituality and spiritual care into education and clinical practice.[2,4,16] In the SA context, a study conducted on the perceptions of spirituality and spiritual care of Unani Tibb practitioners in clinical practice confirmed that Unani Tibb practitioners valued spirituality and spiritual care despite the lack of formal training on these topics.[9] Another significant finding was that all practitioners in this study reported being ill-equipped to deal with spiritual care attributed to the lack of formal training. This study highlighted the need for guidelines on spirituality and spiritual care to improve holistic care in the Unani Tibb profession.[9] In India, Ahmad[16] reported that Unani Tibb students regard spirituality as a crucial component of their education and profession. That study reported a significant correlation between spiritual personality and the level of empathy expressed to patients. No studies on the role of spirituality and spiritual care in Unani Tibb education in SA were found. There is a clear need to investigate this phenomenon in the SA context to gain insights into the perceptions of Unani Tibb students and educators regarding spirituality and spiritual care.[2,5,9]
Methods
This study is in line with sustainable developmental goals (SDG): good health and well-being (SDG3) and quality education (SDG4). This study was conducted at the School of Natural Medicine (SoNM), Faculty of Community and Health Sciences (FCHS), University of the Western Cape (UWC), Cape Town, SA. We employed a sequential explanatory mixed-method approach, consisting of two stages: an initial quantitative study (stage 1) followed by a qualitative study (stage 2). The results of the quantitative study informed and guided the interview questions of the qualitative study.
In stage 1, a quantitative cross-sectional descriptive design was used to provide perspectives of the Unani Tibb students and educators. The convenience sampling method was used to recruit all registered 4th and 5th-year Unani Tibb students (n=10) and Allied Health Professions Council of South Africa (AHPCSA) registered educators (lecturers, clinical supervisors, external examiners and external moderators) (n=10) to participate in the study. The AHPCSA is a statutory health body under the National Department of Health in SA, responsible for the formal regulation of several modalities of CAM including Unani Tibb.[17,18]
A previously validated quantitative tool[2,5,9,13,15,20-22] was used comprising the Spiritual Care-Giving Scale (SCGS),[20] the Spirituality and Spiritual Care Rating Scale (SSCRS)[21] and Spirituality in Unani Tibb Scale (SUTS).[9,15]
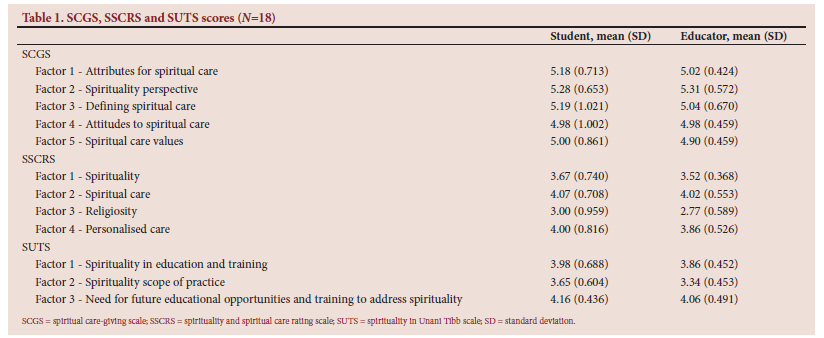
The online Likert scale-type questionnaire was sent via email as a Google link. Participant responses were automatically calculated online, and then exported to Microsoft Excel 2010 to create a compatible dataset for statistical analysis. Descriptive statistics were used to characterise demographic data, presented as frequencies (n) and percentages (%). For the variables from the SCGS, SSCRS and SUTS scales, proportions, mean scores and standard deviations (SDs) are reported. Higher mean scores on these scales indicate a higher level of agreement and a more positive perception and attitude toward spirituality and spiritual care for participants.[5,9,13]
For stage 2, an exploratory descriptive qualitative approach was employed. All participants from stage 1 (quantitative study) were invited to participate in the interviews of stage 2. A purposive sampling method was used to select all registered 4th- and 5th-year Unani Tibb students (n=10) and educators (n=10) at SoNM, including lecturers, clinical supervisors, external examiners and external moderators, to participate in the study.
Individual online interviews were conducted via Google Meets and Zoom from October 2021 - August 2022. The semi-structured interviews were recorded and lasted 30 - 45 mins. All interviews were automatically transcribed via Google Meets/Zoom by enabling the automated transcription option. The interviews continued until data saturation was reached.
An inductive approach to thematic analysis was followed in this study. The six steps of thematic analysis recommended by Braun and Clarke[19] were followed: data familiarisation, initial coding then searching, reviewing, defining, naming and reporting themes. The most significant participant quotes were selected and grouped under the related categories and themes.[19] Co-coding was employed in this study. The qualitative data obtained from stage 2 provided deeper insights into the quantitative findings of stage 1. Both sets of data were analysed separately and then combined after stage 2 to provide the final interpretation of the findings.[19] The sequential explanatory mixed-method design is presented in Fig. 1.
This study was approved by the Biomedical Ethics Committee (ref. no. BM20/2/7) at the UWC.[5]
Results
Stage 1
A total of eight (80%) Unani Tibb students and 10 (100%) Unani Tibb educators participated in the quantitative study. The mean values for perceptions of spirituality and spiritual care were computed for each factor on the SCGS. The mean scores regarding spiritual care practice were computed for each factor on the SSCRS. The mean scores relating to spirituality in Unani Tibb education were computed for each factor on the SUTS. The SCGS, SSCRS and SUTS scores are presented in Table 1.
Stage 2
Five (50%) students and five (50%) educators participated in the qualitative study.
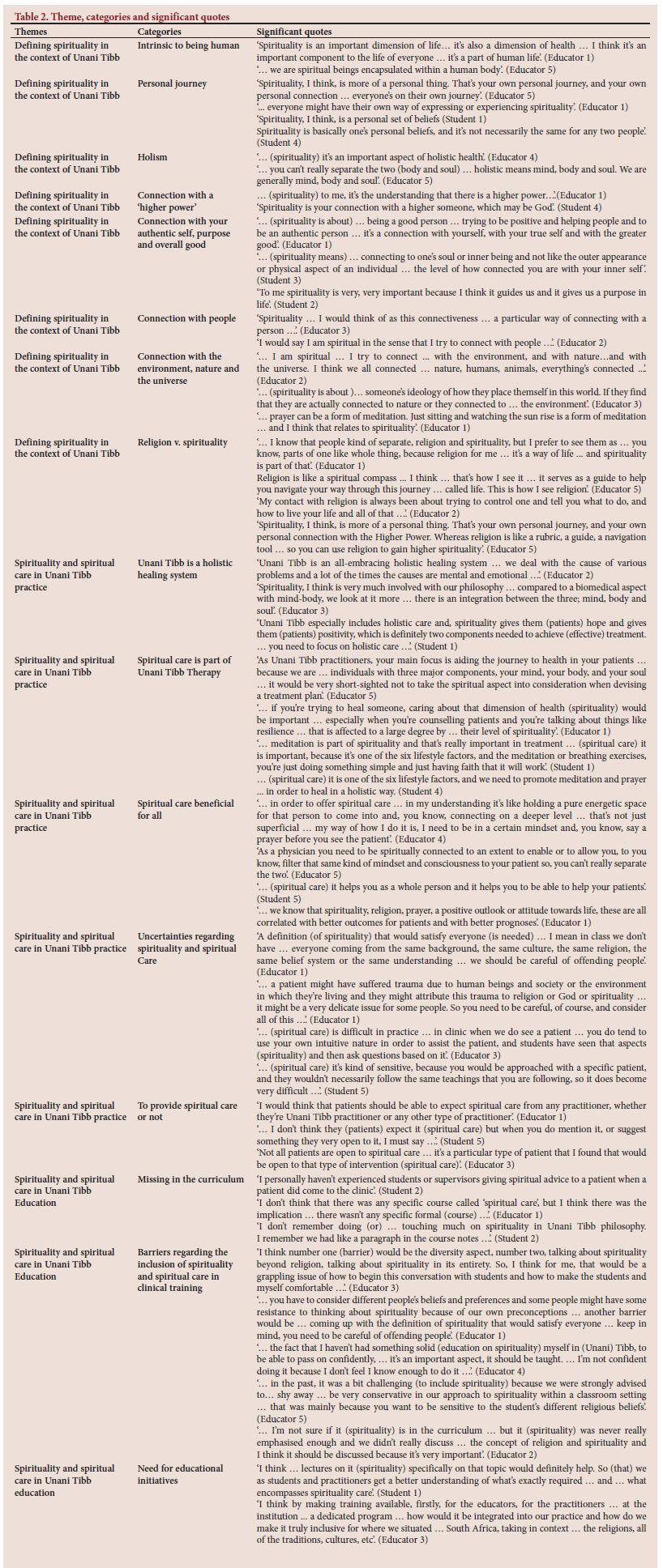
Overall, three interrelated themes, 16 categories and 51 significant quotes emerged from this study (Table 2).
Theme 1: Defining spirituality in the context of Unani Tibb
This theme consists of eight categories, indicating the meaning of spirituality in the context of Unani Tibb. Categories that emerged from this theme include: Intrinsic to being human, Personal journey, Holism, Connection with a 'Higher Power', Connection with your authentic self, purpose and overall good, Connection with people, Connection with the environment, nature and the universe and Religion v. Spirituality.
Theme 2: Spirituality and spiritual care in Unani Tibb practice
This theme encompasses four categories, reflecting student and educators' views on spirituality and spiritual care in Unani Tibb practice. Categories that emerged from this theme include: Unani Tibb is a holistic healing system, Spiritual Care is part of Unani Tibb therapy, Spiritual Care beneficial for all, Uncertainties regarding Spirituality and Spiritual Care and To provide Spiritual Care or not.
Theme 3: Spirituality and spiritual care in Unani Tibb education
This theme comprises three categories that reflect students' and educators' views on spirituality and spiritual care in Unani Tibb education. This theme emerged from the following categories: Missing in the curriculum, Barriers to the teaching and learning of Spiritual Care and Need for educational initiatives.
Discussion
The most significant finding of this mixed-method study was the heightened level of spiritual awareness of this cohort of Unani Tibb students and educators, despite the lack of spirituality and spiritual care content in education and practice in SA. All participants emphasised the holistic nature of Unani Tibb and the importance of spirituality and spiritual care in the lives of students, educators, patients and practitioners. They strongly advocated for the inclusion and integration of spirituality and spiritual care content into the Unani Tibb curriculum.
Conceptualising spirituality and spiritual care
In this study, participants conceptualised spirituality as an important, universal, personal and innate quality of human beings that contributes to emotional and overall well-being. These findings are supported by a previous quantitative study conducted on Unani Tibb practitioners in SA, which reported that most participants scored high on items relating to spiritual awareness and overall patient health and wellness.[9] The study design and quantitative results of stage 1 of this mixed-methods study are congruent with that of the previous study conducted on Unani Tibb practitioners.[9] In addition, in the qualitative component of stage 2 of this mixed-methods study, participants further described their spirituality as a connection to a 'higher power', the authentic self, people, nature and the environment. The connective nature of spirituality was viewed as an internal and external unifier which contributes to inner peace and wellbeing.
All participants found it challenging to define spirituality and spiritual care. However, they understood the existence, importance and related benefits of these concepts in healthcare. They concurred that spirituality involves instilling hope in patients regarding their illness. They viewed spiritual care as a process and not a one-time event or activity. They believed that spiritual care is about respecting a patient's religious, cultural, traditional, spiritual and personal beliefs. Furthermore, participants concurred that sensitivity and intuition help the Unani Tibb practitioner to provide spiritual care.
This study highlights the importance of self-awareness among students and educators concerning their views on spirituality and spiritual care. Spiritually active healthcare practitioners were found to be more sensitive to the spiritual needs of their patients.[2,5,9] Previous studies raised the importance of the relationship between spiritual awareness, spiritual/ religious practices and spiritual care offered by students and educators in clinical settings.[20-24] The high level of spiritual awareness reported for this cohort seems to have contributed to their positive attitudes towards spirituality and spiritual care.
Spiritual care in the scope of practice
In stages 1 and 2 of this mixed-methods study, most participants confirmed that spirituality should be addressed by Unani Tibb practitioners. They emphasised that spiritual care is fundamental to holistic Unani Tibb therapy. They confirmed that addressing the patient's spiritual needs is the responsibility of the Unani Tibb practitioner. Regarding the delivery of spiritual care, participants expressed their feelings of discomfort when addressing spirituality with patients. Participants admitted that they were only comfortable in addressing the spiritual needs of patients when they shared similar religious or spiritual beliefs. This may compromise the holistic approach, which should be applied to all patients of all backgrounds. In a multi-site exploratory study on the role of religion and spirituality in healthcare among CAM practitioners, it was reported that some CAM practitioners felt comfortable in addressing matters of spirituality. However, they acknowledged that they did not have the expertise to deal with this aspect appropriately.[4] Spiritually inclined practitioners were more likely to include spiritual care into their treatment regimens but they felt that they did not have sufficient knowledge on these topics. These practitioners depended on their own forms of spirituality to guide their approach to spiritual care.[2,5,9] CAM practitioners who were less spiritually inclined were less likely to include spiritual care in their treatment. Spiritual care needs of patients seem to be dependent on the practitioner's views on spirituality, which may comprise the holistic approach expected from CAM practitioners. [2,5,9] This seems to be the case for Unani Tibb education and practice in SA.[2,5,9]
Most participants in this study reported that they do not use spiritual assessments to evaluate their patient's spiritual needs. They admitted that they lack awareness of various assessments that address the spiritual needs of their patients. This was confirmed by the previous study on Unani Tibb practitioners that reported the lack of knowledge and use of spiritual assessments in clinical practice.[9] The lack of knowledge of resources on spirituality was seen as a barrier to spiritual care for Unani Tibb practitioners in SA. Additional barriers that were reported were 'general discomfort' and a 'concern of offending patients'.[9] However, the current study reports on an additional barrier to spiritual care at the departmental level within the institution of higher education. A participant explained that a line manager within a department strongly advised against the inclusion of any type of discussion on religion or spirituality in the classroom setting. This contributed to the educator's reluctance to address the topic of spirituality or spiritual care in training. This highlights the need for the formal integration of spirituality and spiritual care concepts into Unani Tibb education. This need has been previously confirmed by Mthembu et al.,[14] regarding occupational therapy education and Linda et al.,[24] regarding nursing education. Both these studies were conducted in SA within a similar sample group to the current study. Furthermore, all participants felt ill-equipped to deal with spiritual care in the classroom and clinical setting. This was largely because of the lack of spirituality and spiritual care content in the curriculum. Therefore, all participants emphasised that spiritual care should be instilled throughout the Unani Tibb education programme and be positively reinforced in Unani Tibb practice. These findings align with those of studies within the Unani Tibb profession in SA and abroad, which reported the need for the integration of spiritual care in Unani Tibb education and practice.[2,4,5,9,16]
Spirituality and spiritual care in education and training
A significant mixed-method finding of this study is the unanimous consensus by participants on the role of spirituality and spiritual care in Unani Tibb education and training. All participants confirmed that their formal education did not adequately prepare them to address the spiritual needs of their patients. This finding is further supported by a previous study conducted on Unani Tibb practitioners in SA.[9] Most practitioners in this study reported a lack of spirituality and spiritual care content in the Unani Tibb curriculum.[9] Spirituality and spiritual care are important concepts in Unani Tibb philosophy but not formalised in education or practice at a regional and global level.[2,5,9]
The Unani Tibb training programme in SA consists of several discipline-specific modules that briefly point out the importance of spirituality and spiritual care. However, there are no specific modules or topics in module descriptors or module outlines with spirituality and spiritual care competency outcomes.[25] The lack of spirituality and spiritual care content in Unani Tibb education seems to be a global phenomenon.[2,5,9] Previous studies in CAM and other health professions reported on the lack of clinical application of spiritual care-related theory.[3-5,9,14,15,24]
The theory-practice gap regarding spirituality and spiritual care also exists in Unani Tibb, as previously reported in other CAM and other healthcare professions.[3-5,9,14,15,24]
In this study, all participants recognised spirituality as an integral part of the human experience and fundamental to the Unani Tibb philosophy and clinical practice. They strongly critiqued the absence of spirituality and spiritual care in education and encouraged the formal integration of these concepts in education and practice. Participants strongly recommended introducing educational workshops or courses for students, educators and practitioners by experts in the field through a multidisciplinary approach.
Study limitations
This study had several limitations. The sample size of this study was small. This study was explorative, Unani Tibb education is a specialised field in SA, with a low number of registered students and educators. A convenience sample method was used in the quantitative study. Participants who volunteered in this study may have a specific interest in this topic. Their views may differ from participants who declined to take part in this study. The qualitative data of this study are subjective and apply to the study participants only, therefore the findings cannot be generalised.
Recommendations
Further research is needed in the SA context to gain deeper insight into this phenomenon. Guidelines for the inclusion of spirituality and spiritual care into Unani Tibb education programmes are required to capacitate Unani Tibb educators to teach spirituality and spiritual care. This will facilitate the integration of holistic caring values in the clinical training setting.
Conclusion
This research fills a critical gap in knowledge regarding the role of spirituality and spiritual care in Unani Tibb education. This is a milestone study conducted in SA, investigating Unani Tibb students' and educators' perspectives on spirituality and spiritual care.
This mixed-methods study provides a deeper understanding of spirituality and spiritual care in Unani Tibb education. Participants in this study acknowledged the integral nature of spirituality in the lives of all people. They also identified spiritual care as fundamental to holistic Unani Tibb practice. This study revealed a heightened spiritual awareness for this cohort despite the lack of spirituality and spiritual care topics in the curricula. All participants emphasised the need for educational initiatives towards formal integration of spirituality and spiritual care in Unani Tibb education. This was regarded as crucial to ensure the integrity of the holistic approach required in clinical practice.
Declaration. This research was done in partial fulfilment of a PhD degree.
Acknowledgements. The authors would like to thank the UWC for the overall support throughout this study. The authors are grateful to the Unani Tibb students and educators at SoNM, FCHS (UWC) for participating in this study. The authors are thankful to Dr Lya Hwa Tiew, Dr Douglas N. Morris and Prof Wilfred McSherry for granting permission to use their instruments for this study.
Author contributions. MH conceptualised the study, collected and analysed data, reviewed the literature, and wrote the manuscript. NVR contributed towards the development of the study, and the analysis of the findings and critically reviewed the manuscript as a supervisor. TGM designed the survey (stage 1) and critically reviewed the manuscript as a supervisor. MH adapted the survey for this study and obtained permission from the authors to use their instruments. MN provided input from the Unani Tibb perspective and critically reviewed the manuscript as a supervisor. All authors commented on previous versions of the manuscript and approved the final manuscript.
Funding. This research is supported in part by the National Research Foundation of South Africa (NRF) (Unique Grant No. 122037). Any opinion, findings and conclusion or recommendations expressed in this material are that of the authors and the NRF does not accept any liability in this regard.
Data availability statement. The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Conflicts of interest. None.
References
1. World Health Organization. WHO traditional medicine strategy: 2014-2023. Geneva: WHO, 2013. http://www.who.int/medicines/publications/traditional/trm_strategy14_23/en/ (accessed 8 May 2022). [ Links ]
2. Hoosen M, Roman NV, Mthembu TG. The role of spirituality and spiritual care in complementary and alternative medicine: A scoping review. Bangladesh J Med Sci 2020;20(4):714-724. https://doi.org/10.3329/bjms.v20i4.54125 [ Links ]
3. Grant A. Spirituality, health and the complementary medicine practitioner. J Au Trad-Med Soc 2017;13(4):207-209. [ Links ]
4. Ramakrishnan P, Dias A, Rane A, et al. Perspectives of Indian traditional and allopathic professionals on religion/ spirituality and its role in medicine: Basis for developing an integrative medicine program. J Relig Health 2014;53(4):1161-1175. https://doi.org/10.1007/s10943-013-9721-2 [ Links ]
5. Hoosen M, Roman NV, Mthembu TG. The development of guidelines for the inclusion of spirituality and spiritual care in Unani Tibb practice in South Africa: A study protocol. J Relig Health 2020;61(2):1261-1281. https://doi.org/10.1007/s10943-020-01105-5 [ Links ]
6. World Health Organization. WHO Benchmarks for the Practice of Unani Medicine. Geneva: WHO, 2022. https://www.who.int/publications/i/item/9789240042698 (accessed 26 June 2022). [ Links ]
7. World Health Organization. WHO Benchmarks for the Training of Unani Medicine. Geneva: WHO, 2022. https://www.who.int/publications/i/item/9789240042735 (accessed 26 June 2022). [ Links ]
8. Peltzer K. Utilisation and practice of traditional/complementary/alternative medicine (TM/CAM) in South Africa. Afr J Trad Med 2009;6(2):175-185. [ Links ]
9. Hoosen M, Roman NV, Mthembu TG, Naseer M. Unani Tibb practitioners' perceptions and attitudes towards spirituality and spiritual care in Unani Tibb practice in South Africa. BMC Complement Med Ther 2023;23(1):189. https://doi.org/10.1186/s12906-023-04002-y [ Links ]
10. Koenig HG. Religion, spirituality and health: The research and clinical implications (Review Article). ISRN 2012;14(1):1-33.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3671693/ [ Links ]
11. McSherry W, Cash K, Ross L. Meaning of spirituality: Implications for nursing practice. J Clin Nurs 2004;13(8):934-941. https://doi.org/10.1111/j.1365-2702.2004.01006.x [ Links ]
12. Meredith P, Murray J, Wilson T, Mitchell G, Hutch R. Can spirituality be taught to health care professionals? J Relig Health 2012;51(3):789-889. https://doi.org/10.1007/s10943-010-9399-7 [ Links ]
13. Mthembu TG, Roman NV, Wegner L. A cross-sectional descriptive study of occupational therapy students' perceptions and attitudes towards spirituality and spiritual care in occupational therapy education. J Relig Health 2016;55(5):1529-1545. https://doi.org/10.10.1007/s1094-015-0125-3 [ Links ]
14. Mthembu TG, Wegner L, Roman NV. Teaching spirituality and spiritual care in health sciences education: A systematic review. Afr J Phys Act Health Sci 2016;22(4:1):1036-1057. http://hdl/handle.net/10520/EJC200068 [ Links ]
15. Morris DN. Perceptions of spirituality and spiritual care in occupational therapy practice. Occup Ther Ment Health 2013;29:60-77. https://doi.org/10.1080/0164212X.2013.761109 [ Links ]
16. Ahmad A. Exploring the relationship between spiritual personality and emotional empathy among medical and Unani students. Int J Indian Psychol 2015;2(3):152-169.https://doi.org/10.25215/0203.090 [ Links ]
17. The South African Tibb Association. Tibb training in South Africa- UWC South Africa: SATA.www.satibb.co.za (accessed 20 April 2022). [ Links ]
18. The Allied Health Professions Council of South Africa. South Africa: AHPCSA www.ahpcsa.co.za (accessed 20 April 2022). [ Links ]
19. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3(2):77-101. https://doi.org/10.1191/1478088706qp063oa [ Links ]
20. National University of Singapore. Tiew LH. Nursing students' perceptions and attitudes about spirituality and spiritual care in practice. Ph.D. thesis. Singapore: 2011. https://core.ac.uk/download/pdf/48646025.pdf (accessed 30 April 2020). [ Links ]
21. McSherry W, Draper P, Kendrick D. Construct validity of a rating scale designed to assess spirituality and spiritual care. Int J Nurs Stud 2002;39(7):723-734. https://doi.org/10.1016/s0020-7489(02)00014-7 [ Links ]
22. Tiew LH, Creedy DK, Chan MF. Student nurses' perspectives of spirituality and spiritual care. Nurs Educ Today 2013;33(6):574-579. https://doi.org/10.1016/j.nedt.2012.06.007 Mthembu TG, Ahmed F, Nkuna T, Yaca K. Occupational therapy students' perceptions of spirituality in training. J Relig Health 2015;54:2178-2197. https://doi.org/10.1007/s10943-014-9955-7 [ Links ]
23. Linda NS, Phetlhu DR, Klopper HC. Nurse educators' understanding of spirituality and spiritual care in nursing: A South African perspective (part 1). Int J Afr Nurs Sci 2020;12:100187. https://doi.org/10.1016/j.ijans.2019.100187 [ Links ]
24. University of the Western Cape. BCM Complementary Medicine: Unani Tibb (8354) Academic Program. South Africa; 2018. https://ap.uwcacza/ViewProgrammeModules.aspx?year=2018&faculty=CHS&programme=8354&costtyp=L (accessed 20 July 2021). [ Links ]
 Correspondence:
Correspondence:
M Hoosen
mahoosen@uwc.ac.za
Received 16 October 2023
Accepted 15 May 2024

{kind=link}
{kind=link}
{kind=link}