










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Family Practice
On-line version ISSN 2078-6204Print version ISSN 2078-6190
SAFP vol.67 n.1 Cape Town Feb. 2025
https://doi.org/10.4102/safp.v67i1.6098
OPEN FORUM
The role of vitamin C on the skin
Lehlohonolo MakhakheI, II
IDepartment of Dermatology, Faculty of Health Science, University of the Free State, Bloemfontein, South Africa
IIThe South African Institute of Dermatology, Bloemfontein, South Africa
ABSTRACT
Vitamin C (ascorbic acid or ascorbate) plays an important role in regulating the health of the skin, promoting the differentiation of epithelial skin cells (keratinocytes) while contributing a notable role in the reduction of melanin synthesis, leading to antioxidative protection against solar-related skin damage. Vitamin C is only sourced from diet because humans have no ability to synthesise it in vivo. Routine dietary intake choices become key in maintaining the skin's integrity, preventing and treating some of the skin conditions encountered regularly by general practitioners and skin specialists alike. There is a strong association between vitamin C and the ageing process, skin pigmentation, control of certain skin diseases and a role in some skin cancers through antioxidation properties. Literature suggests that topical application of vitamin C in different forms of formulations has been demonstrated to have more clinical effect than oral intake.
CONTRIBUTION: This article spotlights the benefits of a vitamin commonly encountered in topical pharmaceutics, ingested as tablets or as part of our routine diet.
Keywords: ascorbic acid; vitamin C; vitamin E; ageing; antioxidant; diet; skin application; UV radiation.
Introduction
The skin is complex and multi-functional; being the largest organ of the body and easily clinically accessible, it can further serve as a reflective source of internal health of the rest of the body. The skin's fundamental role is in providing a protection shield against external environmental threats, such as microbes, chemicals, allergens and radiation.1
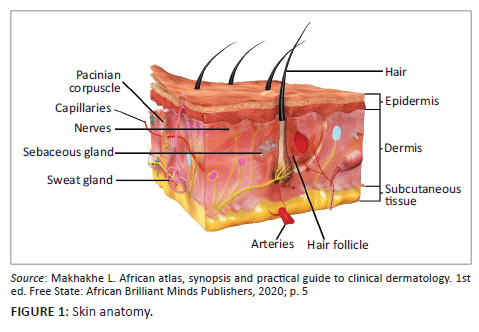
In different cutaneous layers, vitamin C plays a pivotal role in aiding the skin to carry out some of the key functions. These vary from preventative, protective, healing and rejuvenative to assistance in the clinical improvement of some dermatological conditions.2 The epidermis primarily houses keratinocytes and melanocytes, where the antioxidative effects of vitamin C are mostly evident. The dermal layer of the skin provides strength and elasticity and further houses the neurovascular structures, glands and a network of collagen fibres3 (Figure 1).4 There is a marked difference in the levels of vitamin C in the different layers of the skin. The concentration of ascorbic acid in the epidermis is 425% higher than in the dermis.5,6 In the modern era, an accurate method of measuring vitamin C levels within the skin entails taking a skin biopsy. The sample is then analysed utilising high-performance liquid chromatography (HPLC).7 Within the epidermal keratinocytes, there is a concentration gradient of ascorbic acid with a sharp increase in concentration in the deeper layers of the stratum corneum, possibly reflecting depletion in the outer cells attributable to chronic exposure to the external environment. Literature also suggests significant uptake from the gut, rather than cutaneous application, as a source.8,9
Several reports have indicated that vitamin C levels are lower in chronologically aged and photo-damaged skin. Chronological ageing is defined as a natural ageing process through cumulated years, and photo-damage is because of accelerated skin ageing from chronic sun exposure. Whether the low levels of ascorbic acid reflect the cause or effect of ageing remains unclear to date; consequently, this warrants further research in this regard.1
The pharmaceutical industry has a variety of topical formulations with vitamin C contained; these predominantly include creams and gels.
In this article, we review the common physiological benefits of vitamin C on the skin, give an overview of related properties, the role of this vitamin in skin health and disease, homeostasis and the synergistic role with other vitamins, such as vitamin E (tocopherol).
To conduct this review, we utilised the search engines Google Scholar and PubMed, employing specific keywords to search for any relevant articles written in English from 1994 to 2024. A total of 204 articles were identified, with duplicates removed, resulting in 129 articles reviewed. Of the remaining articles, just over 80 were selected, with greater emphasis placed on the more recent publications because of the rapid pace of new developments in knowledge regarding this topic.
Discussion
The role of vitamin C in the prevention of skin ageing
In broad terms, skin ageing can be attributed to several factors, including, but not limited to, chronological and photoageing, smoking, chronic alcohol usage, chronic stress, some medical conditions and a lack of self-care. Normal (intrinsic) ageing contributes directly to loss of elasticity and wrinkle formation; it is largely an unavoidable process that can also be directly linked to genetics.2,10
Within the epidermis, lack of vitamin C can result in peroxidative damage to skin cells; furthermore, the epidermis is constantly exposed to ultraviolet (UV) radiation, further resulting in accelerated ageing because of reactive oxygen species (ROS). In the dermis, deficiencies in ascorbic acid can cause damage to the connective tissue structures, also because of peroxidative stress. Damage can also be as a result of ROS owing to the rich dermal blood supply. While it remains unclear whether high dietary vitamin C intake has better long-term benefits, research suggests that lack of it results in increased oxidative damage, especially in the presence of continuous UV exposure, thus leading to skin ageing.11,12,13
Intrinsic ageing tends to be a protracted natural process, and in the absence of other aggravating factors, changes are not usually apparent until advanced age is reached. The skin changes are typified by fine wrinkling, reduced elasticity, skin atrophy and occasional exaggeration of the Langer's lines expression may be evident. These skin signs may be seen independently, or they may be present in an overlapping sequence.14,15
As ageing progresses, there is a notable decline in the recoiling and elastic capacity of the skin; this is in direct relation with a collective number of factors, such as reduced fibrovascular support structure and a marked decline in extracellular matrix components like collagen and elastin.16,17
The ageing process also results in dry skin (xerosis) because of a gradual decline in glycosaminoglycans within the dermis; however, they help in forming part of the structural network and in retaining dermal moisture. In addition to the reduced ability to retain moisture, skin fragility and easy bruising become progressively apparent as ageing advances, more so in sun-exposed areas such as the face.18,19
The aged epidermis demonstrates a reduced barrier function and reduced repair properties following traumatic insults. In general, the dermis suffers greater age-related changes than the epidermis. Antioxidant capacity, immune regulation and melanin production appear to also be impaired in aged skin.20,21
The regular use of ascorbic acid-containing supplements, either orally or topically, has the potential to reverse skin ageing by regenerating the elastic fibre system and collagen within the dermis.22
Role in hyperpigmentation and skin lightening
Vitamin C has been shown to decrease melanin synthesis by inhibiting melanogenesis both in cultured melanocytes and in vivo.23
This is believed to be because of its ability to interfere with the action of tyrosinase, a rate-limiting enzyme in melanogenesis. Agents that decrease melanogenesis are used to treat skin hyperpigmentation in conditions such as melasma and post-inflammatory hyperpigmentation from different causes. These largely include hydroquinone, glutathione, azelaic acid, niacinamide, glycolic acid, kojic acid, vitamin E, retinoids and cannabidiol.24,25
Skin lightening treatments are steadily gaining traction in the beauty industry, two of the most common reasons being to treat widespread forms of non-segmental vitiligo and for those who find light skin complexion to be of superior appeal. A combination of intravenous glutathione and vitamin C is the popular choice for total eradication of the melanin pigmentation.26,27
Vitamin C and wound healing
Vitamin C acts as a cofactor for the amino acids proline and lysine. It stabilises collagen through hydroxylation, and it also promotes collagen gene expression. Vitamin C may prevent collagen degradation and inhibit the increase of matrix metalloproteinase-1 (MMP-1), which is the major collagenolytic enzyme responsible for collagen damage in UV-irradiated skin.28,29
Wound healing is generally characterised by three overlapping stages, namely inflammation, re-epithelialisation (new tissue formation) and remodelling. The inflammatory stage entails neutrophils as the first cells to the site to engulf damaged tissue and debris and signal macrophages to continue with the consumption of the debris, including spent neutrophils. Various cytokines continue onwards, coupled with fibrin and fibroblast proliferation as re-epithelialisation and remodelling takes place, mostly with scar tissue to a varying degree. Re-epithelialisation restores the skin's barrier function and occurs by a combination of migration and proliferation of the epidermal keratinocytes around the wound site.30,31,32
Vitamin C has been shown to regulate elastin synthesis in cultured fibroblasts and has a marked increase in turnover at the wound sites, because of both local inflammation and the demands of increased collagen production, supporting theories of supplementation being beneficial both in topical and oral intake. Studies have shown that supplementation with both vitamin C and vitamin E improved the rate of wound healing in individuals with extensive burns.33,34
Vitamin C and nutrition
From a nutritional perspective, vitamin C is water soluble, heat sensitive and easily oxidised. Refrigeration aids in retaining its nutritional value. Fruit and vegetable sources should be eaten unpeeled if possible and not be cut into smaller pieces to avoid exposing cells to oxidation. Soaking in water is also discouraged, along with cooking with excessive water or a poorly fitting pot lid. The best sources of vitamin C include citrus fruit, orange juice, spinach, cabbage, green pepper, Brussels sprouts, turnips, guavas, pineapples, sweet melons, fresh strawberries and correctly prepared potatoes. Smaller quantities of this vitamin can also be found in peaches, pears, apples, bananas and blueberries.35,36
Adequate vitamin C as part of a routine diet has been linked with enhanced skin barrier, thereby improving dry skin and smooth skin surface. Vitamin C concentration within the keratinocytes can double upon supplementation with certain foods or 3 g/day supplementation for 6 weeks, a dosage that is significantly higher than the recommended daily intake and would achieve plasma saturation and likely also tissue saturation.37,38
Vitamin C deficiency
Nutritional manifestations are largely in the form of insufficiency states. Scurvy is the clinical manifestation of vitamin C deficiency. Because vitamin C plays a central role in the protective functions of the skin, nutritional deficiency results in skin fragility, perifollicular petechiae, ecchymosis (easy bruising), gingivitis, corkscrew hairs and poor wound healing. Causes may include chronic alcohol abuse, chronic smoking, mental care users, patients on chronic dialysis and poor intake for a plethora of possible reasons.12,39,40
Promoting differentiation of keratinocytes
Through the process of differentiation, keratinocytes play a key role in skin barrier function, thus preventing water loss and microbial invasion to deeper layers. Vitamin C plays an important role in aiding with differentiation.41 Patients with atopic dermatitis have been reported to also suffer from food allergens as a potential trigger source. There is a plausible association between vitamin C deficiency and atopic eczema, resulting from certain food avoidance and precautionary food consumption.42,43,44,45
Furthermore, vitamin C can stimulate ceramide production within keratinocytes and improve overall epidermal barrier function. With increases in clinical symptoms of atopic dermatitis, vitamin C and ceramide levels were reduced; however, this suggests a positive correlation between this form of dermatitis, vitamin C and the natural skin lipids.46,47
Melanoma
The toxic effects of vitamin C on tumour cells may be related to the induction of oxidative stress in cells. Vitamin C can also increase 5-hydroxymethylcytosine (5-hmC) content in melanoma, and this has been demonstrated to reduce tumour growth.48,49
Moreover, cancer patients have been shown to have very low reserves of ascorbic acid, which is essential for the structural integrity of the intercellular matrix, as already alluded to. Degradation of the extracellular matrix correlates with the aggressiveness of tumour growth and invasiveness of a cancer. As part of adjuvant therapy, ascorbic acid supplementation has been found to significantly reduce the metastasis of melanoma in mice. Vitamin C can reduce tumour growth, invasion and metastasis of melanoma in mice by inhibiting the hypoxia-inducible factor-1 alpha (HIF-1α) transcriptional activity, which might play a key role in melanoma carcinogenesis.50,51
Epigenetic pathways
In addition to the gene regulatory activities, vitamin C has a role in epigenetic regulation of gene expression by functioning as a cofactor for the ten-eleven translocation (TET) family of enzymes, which catalyse the removal of methylated cytosine through its hydroxylation to 5-hydroxymethylcytosine.52
Because TETs have a specific requirement for vitamin C to maintain enzyme activity, this provides a further mechanism by which the vitamin may affect gene expression and cell function.53
Aberrant epigenetic alterations are thought to have a role in cancer progression, and there are data to suggest that a loss of 5 hmC occurs during the early development and progression of melanoma.54
Synergistic effects of vitamin C, vitamin E and selenium
The combination of vitamin E and vitamin C has been shown to reduce the incidence of oxidative stress-induced tumours, and their antioxidant effects are much better than the use of vitamin C alone.70,71 This synergy holds true also when ferulic acid and selenium are added as well.3
The combination of vitamin C and vitamin E inhibits melanocyte production more significantly than vitamin C alone.6
Research has also shown that the combination of vitamin A, vitamin C and zinc leads to quicker recovery in wound healing. This is also demonstrated in venous ulcers, as vitamin C stimulates fibroblast proliferation while vitamin A and zinc assist greatly in immune-related functions.72
In addition, vitamin C directly affects the immune system to reduce the chance of viral infection in the body, similar to the application of vitamin D, which can affect the immune mechanisms of the human body. Therefore, whether the combined use of vitamin C and vitamin D has a good and comprehensive therapeutic effect on the presence of herpes zoster and post-herpetic neuralgia is still a question worth exploring.73,74
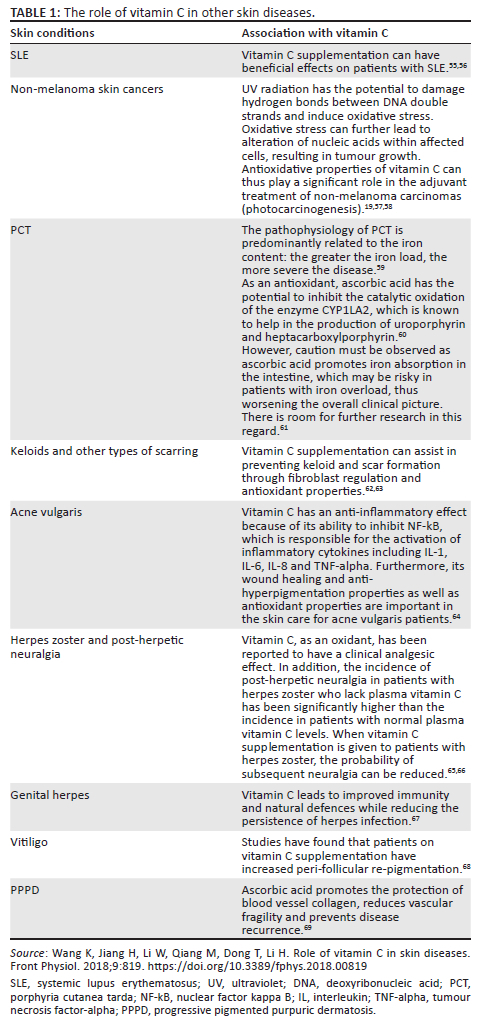
The role of ascorbic acid is also noted in other dermatology-related skin conditions, see Table 1.
Topical application
Vitamin C is a charged molecule that is repelled by the physical barrier of the terminally differentiated epidermal cells. Transcutaneous penetration occurs when the pH levels are below 4; this is when vitamin C is present as ascorbic acid, but whether this results in increased levels in the metabolically compromised stratum corneum is unknown. Furthermore, absorptive capacity also depends on the pH of the formulation that vitamin C is placed in.3,75
Vitamin C can be delivered to the epidermal layer by topical application although the efficacy of this is dependent on the formulation of the cream or serum used on the skin. This entails gentle rubbing of the vitamin, and in this regard, available literature leans more towards the cosmetic value of topical applications containing this vitamin, predominantly in anti-ageing, treatment of hyperpigmentation and skin lightening.
The main focus in current research is on the development of ascorbic acid derivatives for the purpose of topical application. Such derivatives need to ensure stabilisation of the molecule from oxidation and overcome the significant challenge of skin penetration. In addition, they must be converted to ascorbic acid in vivo to be effective. The addition of a phosphate group confers greater stability yet poor epidermal absorption.
Oral intake
Vitamin C is an affordable and available over-the-counter vitamin with low toxicity potential; this aids immensely in exploring all potential medicinal benefits. Oral intake depends on the objective because this vitamin is associated with a wide range of medicinal benefits; the duration, frequency and dosing largely depend on the desired outcome. With adequate dietary intake, oral supplementation has been found to be of limited value.12
There are no studies that have investigated the relationship between skin vitamin C content in relation to oral supply, be it from food or supplementation, when plasma levels are low. However, clinical improvement has been noted in the absence of active measuring of the cutaneous levels. Serum levels are also seldom measured, even in cases of proven clinical deficiencies in developing countries.3
For scurvy, a dosage of 100 mg - 500 mg per day for 2 weeks can result in satisfactory clinical outcomes but must be followed up with a review, and the cause of the deficiency must be identified. Low doses contained within a multivitamin supplementation tablet can be considered as part of health supplementation and optimised immunity. Larger studies are needed to evaluate the optimal formulation, dose, frequency and duration in treating other skin conditions as part of the adjuvant therapy.76
Intravenous intake
This is favoured when used in synergy with glutathione when aiming to universally lighten the skin for those lured by the cosmetic appeal. The appeal may be in those who perceive darker skin as unsatisfactory or those with widespread non-segmental vitiligo. This appeal is predominantly seen among the female gender.77
Toxicity
The recommended daily oral amount for vitamin C is 75 mg a day for women and 90 mg a day for men. During pregnancy, 120 mg a day is recommended because of higher demands of the gestational period. The upper limit for all adults is 2000 mg a day. There is scant and inconclusive data with regard to vitamin C toxicity or complications thereof.78
Topical vitamin C is available in the market as a variety of creams, sera and transdermal patches. Of these, only the serum contains active forms of this vitamin in an almost colourless form. It is unstable and, on exposure to light, gets oxidised to dehydroascorbic acid (DHAA), which imparts a yellow colour. Minor adverse reactions include a yellowish discolouration of the skin, hypopigmented hair and staining of clothes, which occur because of oxidative changes. Once applied, it cannot be fully washed or wiped off the skin. Rarely, stinging, erythema and dryness are observed after topical usage. These can easily be treated using a moisturiser.79,80,81,82
Conclusions
The ability to exclusively measure the efficacy of oral or topically applied vitamin C in preventing ageing remains practically challenging in the wake of other attributing factors.
There is limited evidence in the literature supporting a link between serum vitamin C levels and ageing changes. Vitamin C levels are also almost never measured in the skin, and this information is needed before we can improve our understanding of what level of intake might be beneficial for skin health and protection against ageing-related changes. With the increasing use of HPLC, the correlation between skin concentration and the general health of the skin becomes a key focus of future research output.
In conclusion, vitamin C has many plausible uses in medicine although further research is warranted with regard to dosages for different indications. In the main, past work has focused on the reasons why ascorbic acid can work through its properties and mechanisms of action clinically. Future research must be centred around dosage, frequency, duration, ideal formulation and in-depth monitoring of ideal cutaneous concentrations in relation to response to therapy or supplementation.
Acknowledgements
The author would like to acknowledge Annamarie Du Preez, who edited the article for grammar and presentation.
Competing interests
The author declares that he has no financial or personal relationships that may have inappropriately influenced him in writing this article.
Author's contribution
L.M. is the sole author of this research article.
Ethical considerations
An application for an ethics waiver was made to the University of the Free State, Health Sciences Research Ethics Committee, and an ethics waiver has been granted on 03 September 2024. The ethics waiver number is UFS-HSD2024/1779. The Health Sciences Research Ethics Committee issued an ethics waiver for the study because this article does not contain any studies involving human participants performed by the authors.
Funding information
The author disclosed receipt of the following financial support for this article. This work was supported by the University of the Free State and the South African Institute of Dermatology.
Data availability
The author confirms that the data supporting this study and its findings are available within the article.
Disclaimer
The views and opinions expressed in this article are those of the author and are the product of professional research. It does not necessarily reflect the official policy or position of any affiliated institution, funder or agency or that of the publisher. The author is responsible for this article's results, findings and content.
References
1.Crisan D, Roman I, Crisan M, Scharffetter-Kochanek K, Badea R. The role of vitamin C in pushing back the boundaries of skin aging: An ultrasonographic approach. Clin Cosmet Investig Dermatol. 2015;8:463-470. https://doi.org/10.2147/CCID.S84903 [ Links ]
2.Al-Niaimi F, Chiang NYZ. Topical vitamin C and the skin: Mechanisms of action and clinical applications. J Clin Aesthet Dermatol. 2017;10(7):14-17. [ Links ]
3.Pullar JM, Carr AC, Vissers MCM. The roles of vitamin C in skin health. Nutrients. 2017;9(8):866. https://doi.org/10.3390/nu9080866 [ Links ]
4.Makhakhe L. African atlas, synopsis and practical guide to clinical dermatology. 1st ed. Free State: African Brilliant Minds Publishers, 2020; p. 5. [ Links ]
5.Wang K, Jiang H, Li W, Qiang M, Dong T, Li H. Role of vitamin C in skin diseases. Front Physiol. 2018;9:819. https://doi.org/10.3389/fphys.2018.00819 [ Links ]
6.Shindo Y, Witt E, Han D, Epstein W, Packer L. Enzymic and non-enzymic antioxidants in epidermis and dermis of hunt an skin. J Invest Dermatol. 1994;102:122-124. https://doi.org/10.1111/1523-1747.ep12371744 [ Links ]
7.Abe-Matsumoto L, Sampaio G, Bastos D. Is titration as accurate as HPLC for determination of vitamin C in supplements? Titration versus HPLC for vitamin C analysis. Am J Anal Chem. 2020;11:269-279. https://doi.org/10.4236/ajac.2020.117021 [ Links ]
8.Weber SU, Thiele JJ, Cross CE, Packer L. Vitamin C, uric acid, and glutathione gradients in murine stratum corneum and their susceptibility to ozone exposure. J Invest Dermatol. 1999;113:1128-1132. https://doi.org/10.1046/j.1523-1747.1999.00789.x [ Links ]
9.Papaccio F, Arino AD, Caputo S, Bellei B. Focus on the contribution of oxidative stress in skin aging. Antioxidants (Basel). 2022;11(6):1121. https://doi.org/10.3390/antiox11061121 [ Links ]
10.Wong QYA, Chew FT. Defining skin aging and its risk factors: A systematic review and meta-analysis. Sci Rep. 2021;11(1):22075. https://doi.org/10.1038/s41598-021-01573-z [ Links ]
11.Lephart ED, Naftolin F. Factors influencing skin aging and the important role of estrogens and Selective Estrogen Receptor Modulators (SERMs). Clin Cosmet Investig Dermatol. 2022;15:1695-1709. https://doi.org/10.2147/CCID.S333663 [ Links ]
12.Maxfield L, Daley SF, Crane JS. Vitamin C deficiency [homepage on the Internet]. [updated 2023 Nov 12]. Treasure Island, FL: StatPearls Publishing; 2024 [cited 2024 Oct 16]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493187/ [ Links ]
13.Humbert P, Louvrier L, Saas P, Viennet C. Vitamin C, aged skin, skin health. In: Jean Guy L, editor. Vitamin C - An update on current uses and functions. London: IntechOpen, 2019; p. 29-30. [ Links ]
14.Cao C, Xiao Z, Wu Y, Ge C. Diet and skin aging - From the perspective of food nutrition. Nutrients. 2020;12:870. https://doi.org/10.3390/nu12030870 [ Links ]
15.Zhang S, Duan E. Fighting against skin aging: The way from bench to bedside. Cell Transplant. 2018;27(5):729-738. https://doi.org/10.1177/0963689717725755 [ Links ]
16.Shin JW, Kwon SH, Choi JY, et al. Molecular mechanisms of dermal aging and antiaging approaches. Int J Mol Sci. 2019;20(9):2126. https://doi.org/10.3390/ijms20092126 [ Links ]
17.Zorina A, Zorin V, Kudlay D, Kopnin P. Molecular mechanisms of changes in homeostasis of the dermal extracellular matrix: Both involutional and mediated by ultraviolet radiation. Int J Mol Sci. 2022;23(12):6655. https://doi.org/10.3390/ijms23126655 [ Links ]
18.Brown TM, Krishnamurthy K. Histology, dermis [homepage on the Internet]. [updated 2022 Nov 14]. Treasure Island, FL: StatPearls Publishing; 2024 [cited 2024 Oct 16]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535346/ [ Links ]
19.Engelke M, Jensen JM, Ekanayake-Mudiyanselage S, Proksch E. Effects of xerosis and ageing on epidermal proliferation and differentiation. Br J Dermatol. 1997;137(2):219-225. https://doi.org/10.1046/j.1365-2133.1997.18091892.x [ Links ]
20.Rinnerthaler M, Bischof J, Streubel MK, Trost A, Richter K. Oxidative stress in aging human skin. Biomolecules. 2015;5:545-589. https://doi.org/10.3390/biom5020545 [ Links ]
21.Chambers ES, Vukmanovic-Stejic M. Skin barrier immunity and ageing. Immunology. 2020;160(2):116-125. https://doi.org/10.1111/imm.13152 [ Links ]
22.Csekes E, Račková L. Skin aging, cellular senescence and natural polyphenols. Int J Mol Sci. 2021;22(23):12641. https://doi.org/10.3390/ijms222312641 [ Links ]
23.Boo YC. Ascorbic acid (vitamin C) as a cosmeceutical to increase dermal collagen for skin antiaging purposes: Emerging combination therapies. Antioxidants (Basel). 2022;11(9):1663. https://doi.org/10.3390/antiox11091663 [ Links ]
24.Choi JY, Ha JW, Boo YC. Multifaceted effects of L-cysteine, L-ascorbic acid, and their derivatives on the viability and melanin synthesis of B16/F10 cells under different conditions. Antioxidants. 2024;13:330. https://doi.org/10.3390/antiox13030330 [ Links ]
25.Ebanks JP, Wickett RR, Boissy RE. Mechanisms regulating skin pigmentation: The rise and fall of complexion coloration. Int J Mol Sci. 2009;10(9):4066-4087. https://doi.org/10.3390/ijms10094066 [ Links ]
26.Makhakhe L. Topical cannabidiol (CBD) in skin pathology - A comprehensive review and prospects for new therapeutic opportunities. S Afr Fam Pract. 2022;64(1):e1-e4. https://doi.org/10.4102/safp.v64i1.5493 [ Links ]
27.Davids LM, Van Wyk J, Khumalo NP, Jablonski NG. The phenomenon of skin lightening: Is it right to be light? S Afr J Sci. 2016;112(11-12):1-5. https://doi.org/10.17159/sajs.2016/20160056 [ Links ]
28.Juliano CCA. Spreading of dangerous skin-lightening products as a result of colourism: A review. Appl Sci. 2022;12:3177. https://doi.org/10.3390/app12063177 [ Links ]
29.Brennan M, Bhatti H, Nerusu KC, et al. Matrix metalloproteinase-1 is the major collagenolytic enzyme responsible for collagen damage in UV-irradiated human skin. Photochem Photobiol. 2003;78(1):43-48. https://doi.org/10.1562/0031-8655(2003)078<0043:mmitmc>2.0.co;2 [ Links ]
30.Offord EA, Gautier JC, Avanti O, et al. Photoprotective potential of lycopene, beta-carotene, vitamin E, vitamin C and carnosic acid in UVA-irradiated human skin fibroblasts. Free Radic Biol Med. 2002;32(12):1293-1303. https://doi.org/10.1016/s0891-5849(02)00831-6 [ Links ]
31.Wallace HA, Basehore BM, Zito PM. Wound healing phases [homepage on the Internet]. [updated 2023 Jun 12]. Treasure Island, FL: StatPearls Publishing; 2024 [cited 2024 Oct 16]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470443/ [ Links ]
32.Schultz GS, Chin GA, Moldawer L, et al. Principles of wound healing. In: Fitridge R, Thompson M, editors. Mechanisms of vascular disease: A reference book for vascular specialists [homepage on the Internet]. Adelaide: University of Adelaide Press, 2011 [cited 2024 Oct 16]; p. 23. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534261/ [ Links ]
33.Raziyeva K, Kim Y, Zharkinbekov Z, Kassymbek K, Jimi S, Saparov A. Immunology of acute and chronic wound healing. Biomolecules. 2021;11:700. https://doi.org/10.3390/biom11050700 [ Links ]
34.Bechara N, Flood VM, Gunton JE. A systematic review on the role of vitamin C in tissue healing. Antioxidants (Basel). 2022;11(8):1605. https://doi.org/10.3390/antiox11081605 [ Links ]
35.DePhillipo NN, Aman ZS, Kennedy MI, Begley JP, Moatshe G, LaPrade RF. Efficacy of vitamin C supplementation on collagen synthesis and oxidative stress after musculoskeletal injuries: A systematic review. Orthop J Sports Med. 2018;6(10):2325967118804544. https://doi.org/10.1177/2325967118804544 [ Links ]
36.Giannakourou MC, Taoukis PS. Effect of alternative preservation steps and storage on vitamin C stability in fruit and vegetable products: Critical review and kinetic modelling approaches. Foods. 2021;10(11):2630. https://doi.org/10.3390/foods10112630 [ Links ]
37.Lee S, Choi Y, Jeong HS, Lee J, Sung J. Effect of different cooking methods on the content of vitamins and true retention in selected vegetables. Food Sci Biotechnol. 2017;27(2):333-342. https://doi.org/10.1007/s10068-017-0281-1 [ Links ]
38.Michalak M, Pierzak M, Kręcisz B, Suliga E. Bioactive compounds for skin health: A review. Nutrients. 2021;13:203. https://doi.org/10.3390/nu13010203 [ Links ]
39.Carr AC, Maggini S. Vitamin C and immune function. Nutrients. 2017;9(11):1211. https://doi.org/10.3390/nu9111211 [ Links ]
40.Gandhi M, Elfeky O, Ertugrul H, Chela HK, Daglilar E. Scurvy: Rediscovering a forgotten disease. Diseases. 2023;11(2):78. https://doi.org/10.3390/diseases11020078 [ Links ]
41.Trapani S, Rubino C, Indolfi G, Lionetti P. A narrative review on pediatric scurvy: The last twenty years. Nutrients. 2022;14:684. https://doi.org/10.3390/nu14030684 [ Links ]
42.Joshi M, Hiremath P, John J, et al. Modulatory role of vitamins A, B3, C, D, and E on skin health, immunity, microbiome, and diseases. Pharmacol Rep. 2023;75:1096-1114. https://doi.org/10.1007/s43440-023-00520-1 [ Links ]
43.Boguniewicz M, Leung DY. Atopic dermatitis: A disease of altered skin barrier and immune dysregulation. Immunol Rev. 2011;242(1):233-246. https://doi.org/10.1111/j.1600-065X.2011.01027.x [ Links ]
44.Pareek A, Kumari L, Pareek A, et al. Unraveling atopic dermatitis: Insights into pathophysiology, therapeutic advances, and future perspectives. Cells. 2024;13:425. https://doi.org/10.3390/cells13050425 [ Links ]
45.Fania L, Moretta G, Antonelli F, et al. Multiple roles for cytokines in atopic dermatitis: From pathogenic mediators to endotype-specific biomarkers to therapeutic targets. Int J Mol Sci 2022;23:2684. https://doi.org/10.3390/ijms23052684 [ Links ]
46.Dhar S, Srinivas SM. Food allergy in atopic dermatitis. Indian J Dermatol. 2016;61(6):645-648. https://doi.org/10.4103/0019-5154.193673 [ Links ]
47.Kim KP, Shin KO, Park K, et al. Vitamin C stimulates epidermal ceramide production by regulating its metabolic enzymes. Biomol Ther (Seoul). 2015;23(6):525-530. https://doi.org/10.4062/biomolther.2015.044 [ Links ]
48.Shin J, Kim YJ, Kwon O, Kim NI, Cho Y. Associations among plasma vitamin C, epidermal ceramide and clinical severity of atopic dermatitis. Nutr Res Pract. 2016;10(4):398-403. https://doi.org/10.4162/nrp.2016.10.4.398 [ Links ]
49.Gustafson JL, Neklesa TK, Cox CS, et al. Small-molecule-mediated degradation of the androgen receptor through hydrophobic tagging. Angew Chem Int Ed Engl. 2015;54(33):9659-9662. https://doi.org/10.1002/anie.201503720 [ Links ]
50.Stojkovic-Filipovic J, Kittler H. Dermatoscopy of amelanotic and hypomelanotic melanoma. J Dtsch Dermatol Ges. 2014;12(6):467-472. https://doi.org/10.1111/ddg.12368 [ Links ]
51.Cha Y, Erez T, Reynolds IJ, et al. Drug repurposing from the perspective of pharmaceutical companies. Br J Pharmacol. 2018;175(2):168-180. https://doi.org/10.1111/bph.13798 [ Links ]
52.Miles R. Complexity, representation and practice: Case study as method and methodology. Issues Educ Res. 2015;25(3):309-318. [ Links ]
53.Pavlovic V, Ciric M, Petkovic M, Golubovic M. Vitamin C and epigenetics: A short physiological overview. Open Med (Wars). 2023;18(1):20230688. https://doi.org/10.1515/med-2023-0688 [ Links ]
54.Coker SJ, Smith-Díaz CC, Dyson RM, Vissers MCM, Berry MJ. The epigenetic role of vitamin C in neurodevelopment. Int J Mol Sci. 2022;23(3):1208. https://doi.org/10.3390/ijms23031208 [ Links ]
55.Sarkar D, Leung EY, Baguley BC, Finlay GJ, Askarian-Amiri ME. Epigenetic regulation in human melanoma: Past and future. Epigenetics. 2015;10(2):103-121. https://doi.org/10.1080/15592294.2014.1003746 [ Links ]
56.Constantin MM, Nita IE, Olteanu R, et al. Significance and impact of dietary factors on systemic lupus erythematosus pathogenesis. Exp Ther Med. 2019;17(2):1085-1090. https://doi.org/10.3892/etm.2018.6986 [ Links ]
57.Pesqueda-Cendejas K, Rivera-Escoto M, Meza-Meza MR, et al. Nutritional approaches to modulate cardiovascular disease risk in systemic lupus erythematosus: A literature review. Nutrients. 2023;15(4):1036. https://doi.org/10.3390/nu15041036 [ Links ]
58.McArdle JJ, Ferrer-Caja E, Hamagami F, Woodcock RW. Comparative longitudinal structural analyses of the growth and decline of multiple intellectual abilities over the life span. Dev Psychol. 2002;38(1):115-142. https://doi.org/10.1037/0012-1649.38.1.115 [ Links ]
59.Lin S, Reibman J, Jones RR, et al. Respond to 'assessment of respiratory symptoms after September 11'. Am J Epidemiol. 2005;162(6):511-512. https://doi.org/10.1093/aje/kwi235 [ Links ]
60.Sinclair PR, Gorman N, Shedlofsky SI, et al. Ascorbic acid deficiency in porphyria cutanea tarda. J Lab Clin Med. 1997;130(2):197-201. https://doi.org/10.1016/S0022-2143(97)90096-2 [ Links ]
61.Akram NA, Shafiq F, Ashraf M. Ascorbic acid - A potential oxidant scavenger and its role in plant development and abiotic stress tolerance. Front Plant Sci. 2017;8:613. https://doi.org/10.3389/fpls.2017.00613 [ Links ]
62.Gerster H. High-dose vitamin C: A risk for persons with high iron stores? Int J Vitam Nutr Res. 1999;69(2):67-82. https://doi.org/10.1024/0300-9831.69.2.67 [ Links ]
63.Hujoel PP, Hujoel MLA. Vitamin C and scar strength: Analysis of a historical trial and implications for collagen-related pathologies. Am J Clin Nutr. 2022;115(1):8-17. https://doi.org/10.1093/ajcn/nqab262 [ Links ]
64.Thomas A, Farah K, Millis RM. Epigenetic influences on wound healing and hypertrophic-keloid scarring: A review for basic scientists and clinicians. Cureus. 2022;14(3):e23503. https://doi.org/10.7759/cureus.23503 [ Links ]
65.Podgórska A, Puścion-Jakubik A, Markiewicz-Żukowska R, Gromkowska-Kępka KJ, Socha K. Acne vulgaris and intake of selected dietary nutrients - A summary of information. Healthcare (Basel). 2021;9(6):668. https://doi.org/10.3390/healthcare9060668 [ Links ]
66.Carr AC, McCall C. The role of vitamin C in the treatment of pain: New insights. J Transl Med. 2017;15(1):77. https://doi.org/10.1186/s12967-017-1179-7 [ Links ]
67.Chen HH, Chen YM, Chen TJ, Lan JL, Lin CH, Chen DY. Risk of herpes zoster in patients with systemic lupus erythematosus: A three-year follow-up study using a nationwide population-based cohort. Clinics (Sao Paulo). 2011;66(7):1177-1182. https://doi.org/10.1590/s1807-59322011000700009. Erratum in: Clinics (Sao Paulo). 2012;67(9):1123. [ Links ]
68.Hovi T, Hirvimies A, Stenvik M, Vuola E, Pippuri R. Topical treatment of recurrent mucocutaneous herpes with ascorbic acid-containing solution. Antiviral Res. 1995;27(3):263-270. https://doi.org/10.1016/0166-3542(95)00010-j [ Links ]
69.Jalel A, Soumaya GS, Hamdaoui MH. Vitiligo treatment with vitamins, minerals and polyphenol supplementation. Indian J Dermatol. 2009;54(4):357-360. https://doi.org/10.4103/0019-5154.57613 [ Links ]
70.Morquette AJ, Lee JB, Grossman SK, Hsu S. Rutoside and ascorbic acid in the treatment of schamberg pigmented purpuric dermatosis. Cureus. 2021;13(4):e14592. https://doi.org/10.7759/cureus.14592 [ Links ]
71.Traber MG, Stevens JF. Vitamins C and E: Beneficial effects from a mechanistic perspective. Free Radic Biol Med. 2011;51(5):1000-1013. https://doi.org/10.1016/j.freeradbiomed.2011.05.017 [ Links ]
72.Didier AJ, Stiene J, Fang L, Watkins D, Dworkin LD, Creeden JF. Antioxidant and anti-tumor effects of dietary vitamins A, C, and E. Antioxidants (Basel). 2023;12(3):632. https://doi.org/10.3390/antiox12030632 [ Links ]
73.Barchitta M, Maugeri A, Favara G, et al. Nutrition and wound healing: An overview focusing on the beneficial effects of curcumin. Int J Mol Sci. 2019;20(5):1119. https://doi.org/10.3390/ijms20051119 [ Links ]
74.Hemilä H. Vitamin C and infections. Nutrients. 2017;9(4):339. https://doi.org/10.3390/nu9040339 [ Links ]
75.Chao CT, Chiang CK, Huang JW, Hung KY. Vitamin D is closely linked to the clinical courses of herpes zoster: From pathogenesis to complications. Med Hypotheses. 2015;85(4):452-457. https://doi.org/10.1016/j.mehy.2015.06.027 [ Links ]
76.Telang PS. Vitamin C in dermatology. Indian Dermatol Online J. 2013;4(2):143-146. https://doi.org/10.4103/2229-5178.110593 [ Links ]
77.Abdullah M, Jamil RT, Attia FN. Vitamin C (ascorbic acid) [homepage on the Internet]. [updated 2023 May 01]. Treasure Island, FL: StatPearls Publishing; 2024 [cited 2024 Oct 16]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499877/ [ Links ]
78.Sanadi RM, Deshmukh RS. The effect of vitamin C on melanin pigmentation - A systematic review. J Oral Maxillofac Pathol. 2020;24(2):374-382. https://doi.org/10.4103/jomfp.JOMFP_207_20 [ Links ]
79.National Institutes of Health Office of Dietary Supplements. 2021, Health Information, Vitamin C Fact Sheet for Consumers [homepage on the Internet]. 2021 [cited 2024 Nov 17]. Available from: https://ods.od.nih.gov/factsheets/VitaminC-Consumer/ [ Links ]
80.Doseděl M, Jirkovský E, Macáková K, et al. Vitamin C - Sources, physiological role, kinetics, deficiency, use, toxicity, and determination. Nutrients. 2021;13:615. https://doi.org/10.3390/nu13020615 [ Links ]
81.Brasil. Resolução RDC n° 360, de 23 de dezembro de (2003) Aprova o Regulamento Técnico sobre Rotulagem Nutricional de Alimentos Embalados, tornando obrigatória a rotulagem nutricional. Brasília, DF: Ministério da Saúde; 2003. [ Links ]
82.Raatz SK, Jahns L, Johnson LK, et al. Smokers report lower intake of key nutrients than nonsmokers, yet both fall short of meeting recommended intakes. Nutr Res. 2017;45:30-37. https://doi.org/10.1016/j.nutres.2017.07.010 [ Links ]
 Correspondence:
Correspondence:
Lehlohonolo Makhakhe
makhakhel@ufs.ac.za
Received: 01 Dec. 2024
Accepted: 18 Mar. 2025
Published: 14 July 2025
