










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Psychiatry
On-line version ISSN 2078-6786Print version ISSN 1608-9685
S. Afr. j. psyc. vol.29 n.1 Pretoria 2023
https://doi.org/10.4102/sajpsychiatry.v29i0.2139
ORIGINAL RESEARCH
Knowledge, attitudes, and help-seeking behaviour for mental illness in a Christian community
Nomthandazo Hlongwane; Vidette Juby
Discipline of Psychiatry, School of Clinical Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Christian beliefs have a role in conceptualising mental illness, which determines help-seeking behaviour and treatment choices. The topic of mental illness is controversial in many Christian circles and is often avoided because of the beliefs and teachings stemming from the Christian faith. Inadequate and inaccurate knowledge about mental illness and its causes negatively impacts the attitudes towards mental illness, the mentally ill, and ultimately help-seeking behaviour.
AIM: This study aimed to explore knowledge, attitudes, and help-seeking behaviour for mental illness in a Christian community.
SETTING: A descriptive, quantitative cross-sectional survey was conducted, comprising 300 congregants from a Pentecostal Christian charismatic church - Assemblies of God in KwaZulu-Natal.
METHODS: A socio-demographic tool was used to capture the relevant social, demographic, and religious information. Existing self-administered questionnaires were used to collect information in four areas: Mental Health Knowledge Schedule, the Reported and Intended Behaviour Scale, Community Attitudes Towards Mentally Ill scale and the Dimensions of Religiosity Scale to determine the degree of religiosity.
RESULTS: The population studied demonstrates high levels of mental health knowledge and a tolerant attitude towards persons who have mental illness. There is a high preference for professional treatment.
CONCLUSION: The high knowledge in this Christian community is associated with a reduction in stigma and a positive attitude towards mental illness. If mental health awareness is encouraged, it helps to encourage positive help-seeking practices tolerance, and treatment outcomes.
CONTRIBUTION: This study highlights levels of knowledge and its influence on help-seeking practices and stigma in a Christian community.
Keywords: mental health; knowledge; attitudes; Christian community; help seeking.
Introduction
Mental illness is a major contributor to the global burden of disease.1 Results from the first nationally representative study of psychiatric morbidity in South Africa indicate that approximately 30% of adults will experience a psychiatric disorder in their lifetime. The majority of South Africans are likely to have a direct or indirect encounter with mental illness in their lifetime.1
Spirituality and religion play a significant role in mental health. Its significance is evident in individual consultations with mental healthcare users as some tend to rely on their faith to help them to recover and overcome their distress.2,3 However, there is a risk that the mental healthcare user will not comply with medical treatment modalities if his or her religious beliefs conflict with the medical approach. Spirituality has a significant influence on patients' attitudes and practices contributing to mental illness and recovery.2,3,4
Spiritual beliefs and practices can have a positive influence on mental health associated with better mental health outcomes.5 Involvement in a spiritual society results in enhanced social support and social interaction and can shape how one relates with others.3,5 Spiritual involvement also provides guidelines for lifestyle choices including healthy living choices. During trial and suffering, people derive meaning and purpose from their spiritual beliefs.
Although spiritual beliefs can relieve distress, they may be inadequate when symptoms are severe and professional intervention is needed.6 This was the finding of a systematic review on spiritual health by Harold Koenig which showed that, when a person's distress had progressed beyond a certain severity, spiritual beliefs may not be sufficient to bring about relief. In a state where there is an inability to mobilise adequate spiritual resources, professional mental health intervention is required to return the afflicted to the state of being able to draw comfort from their spiritual belief. It can be difficult to distinguish between mental and emotional disorders when they are entangled with spiritual believe. This poses a challenge in making a distinction between religious believing a cause of distress (liability) as opposed to it being a means of help (a resource).6,7
Studies show that conservative Christians, including charismatics, are more likely to attribute the cause of mental illness to spiritual factors and believe that faith is the most effective treatment option and thus encourages spiritual-based treatment modalities.8 Such teaching is associated with the attitude that mental illness does not exist, and once a person becomes a Christian, they are immune to mental illness.8,9
Charismatic Christianity is a fast-growing religious denomination that has special views that speak to miraculous acts as a solution to worldly problems including disease.10,11 According to the Bible, Jesus instructed his 12 disciples to heal the sick as he did when he was on earth (Bible Luke Chapter 9). Miraculous acts have since been attributed to the Holy Spirit. The modern Pentecostal religious movement began when a Methodist minister sought answers on how the miracles recorded in the Bible New Testament came about. This movement is associated with unabashed emotionality, belief in personal contact with the Holy Spirit as manifested by speaking in strange tongues, and healing through spiritual means.7,10
Religious beliefs are further influenced by ethnicity and culture in predicting attitudes and interpretation of mental illness.7,12 Even within a specified denomination, there are differences in beliefs and attitudes about mental illness, which are attributed to the specific ethnic group even when the general teachings are not different.13 The approach to addressing mental illness is often influenced by religious beliefs among African Christian and Muslim communities. This choice is guided by the belief in mental illness having a spiritual origin over organic cause.6,13,14 There are varying approaches to addressing mental health issues among Christians.3,12,15,16 Conservative Christians may turn to religious support, often citing sin and a lack of self-control as the root of mental illness. This perspective can sometimes create a reluctance to seek professional help, but many still find comfort in their faith. Meanwhile, liberal Christians tend to prioritise seeking assistance from trained health professionals who share their religious beliefs, to avoid being misunderstood. To better address mental health issues, promoting greater awareness and education about mental illness can help reduce the stigma associated with seeking professional help, while also encouraging individuals to seek the support they need.12,15
This study aimed to explore the knowledge, attitudes, and help-seeking behaviour for mental illness among congregants in a Pentecostal Christian charismatic church in KwaZulu-Natal.
Research methods and design
This was a descriptive, quantitative cross-sectional survey of congregants from a Pentecostal Christian charismatic church - Assemblies of God in KwaZulu-Natal.
The church members were approached with the permission of the church leadership using an existing communication method (WhatsApp Group) as well as directly.
As per the inclusion criteria, all members and leadership (Church Pastors and committee members) of the Assemblies of God church aged 18 years and above were eligible to participate. Furthermore, inclusion in the study required the participant to have the ability to give consent and have English literacy. The study was conducted with permission solely from KwaZulu-Natal branches, which resulted in the exclusion of church members residing outside the province.
The survey link is linked to a Google forms database https://docs.google.com/forms/d/e/1FAIpQLSer1BN4Is-2e3BSxSQj-QmTEJF8bukjGSvUQW4FxsHVhbVI9w/), which was forwarded to the participants via WhatsApp and email. Participants completed the survey online, and the results were entered into a database.
The sample size was based on the statistical parameters, of which the proportion was assumed to be 0.8 and the confidence interval 1.96; the required sample size for the study would be approximately 246. To make allowance for attrition, a 10% increase was made. It was assumed that this sample size would reduce the type 1 and type 2 errors as well as known and unknown confounding effects. Thus, power (1-beta) (the % chance of detecting difference) of the study was set at 80%. Given the aforesaid, the minimum sample size was set at 300 participants for this study.
The survey included a socio-demographic tool that was used to capture the relevant social, demographic, and religious history details. The following self-administered questionnaires were used to collect information on knowledge, attitude, and behaviour: Mental Health Knowledge Schedule (MAKS), The Reported and Intended Behaviour Scale (RIBS), Community Attitudes Towards Mentally Ill scale (CAMI) and the Dimensions of Religiosity scale (Appendix 1). It should be observed that the questionnaires used have yet to be formally validated in South Africa. However, it is important to mention that permission to utilise these tools through the Indigo network, which was obtained upon registration, was secured.
Mental Health Knowledge Schedule
The MAKS scale rates 12 items on a 5-point Likert scale (agree strongly, agree slightly, neither agree nor disagree, disagree slightly, disagree strongly). This scale covers stigma-related mental health knowledge as well as respondents' ability to recognise various conditions as mental illnesses. This tool has been used in several studies in the 'Time to Change' anti-stigma campaign in the UK and is a reliable and validated tool (internal consistency, Cronbach's alpha = 0.65; overall test-retest reliability, Lin's concordance statistic = 0.71).17
The Reported and Intended Behaviour Scale
This tool measures behaviour with regard to mental health about stigma. The RIBS is a measure of mental health stigma-related behaviour. It comprises eight items scored on a cardinal scale of 1-5. It is an existing tool that is validated, was developed in London, and can be used in conjunction with the MAKS tools. There is a strong consensus on the validity and comprehensibility as rated by users and international experts in the field of stigma research. Overall test-retest reliability of the RIBS was 0.75 (Lin's concordance statistic) and the overall internal consistency among items was 0.85 Cronbach's alpha.18
Community Attitudes towards Mentally Ill Scale
The CAMI scale consists of 27 items, which respondents are asked to rate on a five-point Likert scale from 1 (strongly agree) to 5 (strongly disagree). This scale evaluates the participants' attitude towards individuals with mental illness. Taylor and Dear's research yielded satisfactory alpha coefficients (AU, α = 0.68; BE, α = 0.76; SR, α = 0.80; CMHI, α = 0.88) for the internal consistency of the subscales. This scale evaluates the participants' attitude towards individuals with mental illness. Taylor and Dear's research yielded satisfactory alpha coefficients (AU, α = 0.68; BE, α = 0.76; SR, α = 0.80; CMHI, α = 0.88) for the internal consistency of the subscales.19
The Dimensions of Religiosity Scale
This is a 20-item tool self-report measure of religious pre-occupation, guidance, conviction, and emotional involvement. The 20-item Dimensions of Religiosity Scale (DR Scale) is scored on a 5-point Likert scale, ranging from strongly agree (5) to strongly disagree (1), with the scoring reversed for negatively worded items. The total scale was also highly internally reliable with a Cronbach's alpha of 0.95 (Cronbach, 1951). This tool has been validated and used in many research studies. It is easy to complete and takes approximately 5 min to complete.20
The total scores of CAMI, MAKS and RIBS scales, 25th, 50th and 75th percentile were considered as cut-off points for a low, medium and high scores (Table 1).

Ethical considerations
Ethical approval for the study was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (approval BREC/00002281/2021). Informed consent was obtained from all participants. The commencement of the online survey encompasses an introductory page that furnishes comprehensive particulars about the survey, comprising pertinent information concerning consent and ethical standards.
Statistical analysis
Data were captured on Excel spreadsheets and analysed using IBM SPSS version 27. Descriptive analysis statistics were performed for percentages, means and their corresponding standard deviation in data analysis. To determine if demographic variables can predict outcomes, logistic regression analysis was performed. Statistical significance was set at p < 0.05.
Results
Socio-demographic characteristics of the participants
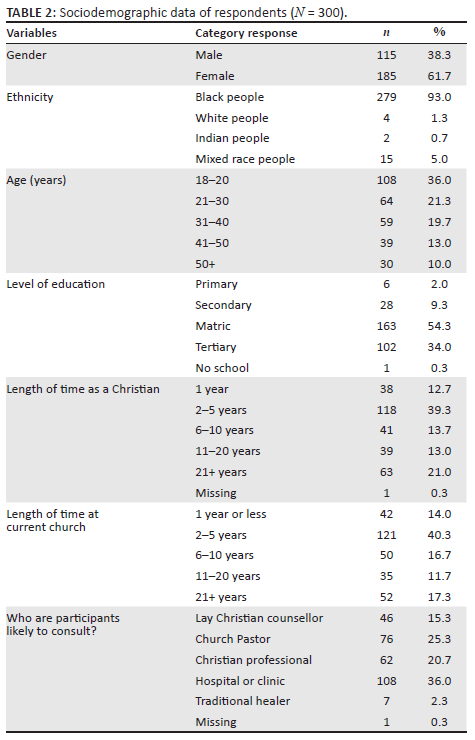
A total of 300 respondents met criteria and completed the questionnaires, of which 185 (61.7%) were female and 115 (38.3%) were male. The largest group of respondents were between 18 years and 20 years of age (n = 108, 36%), whereas only 10% of the group were over the age of 50 years. Most of the participants (n = 163, 54%) had completed high school while only one participant had no formal education. More than half of the respondents had been attending their current church for 5 years or less. The Sociodemographic data of respondents can be seen in Table 2.
Mental Health Knowledge Schedule
High knowledge scores were recorded for 141 (47%) participants and 110 (37%) respondents scored in the moderate knowledge range. There were 49 (16%) participants with low-level mental health knowledge and attitude. There were high levels of agreement that schizophrenia, bipolar and depression are types of mental illness. Schizophrenia and bipolar disorder were correctly identified as a mental illness by 76.3% and 71.7% of respondents, respectively. Depression and drug addiction were less often recognised as mental illnesses (61% and 58% of respondents, respectively).
Community Attitudes towards Mentally Ill scale
Higher CAMI scores indicate less stigma. Medium scores of public stigma towards mental illness were most common in respondents: 141 (46.8%) had a medium score while 96 (31.6%) had more favourable attitude (high score). Half of the male respondents (n = 58; 50%) scored in and above the 75th percentile indicating favourable attitudes towards mental illness and most females, that is, 96 (52%) had a medium attitude response. Across the ethnic groups, most scores were in the 50th percentile with intermediate attitude. The tabulated results of CAMI can be seen in Table 3.
Reported and Intended Behaviour Scale
Subscale A - indicates previous or past behaviours, with high scores indicating a higher contact with the mentally ill. There were 139 (46%) who scored medium and 95 (31.6%) who scored high indicating a fairly high community exposure to the mentally ill.
The majority of respondents (n = 154; 51.3%) reported either currently living with or previously having lived with someone with a mental health problem. However, 63% (n = 189) of respondents reported not having worked with someone with a mental illness, and a high number of participants, 186 (62%) reported no history of having neighbours with mental health problems (Table 4a).
Subscale B
Subscale B scores reflect positive attitudes towards individuals with mental illness, indicating a willingness to engage with and treat them with kindness. The mean score was 12.47 with a standard deviation of 5.78. However, a small percentage of participants (less than 25%) reported a lack of willingness to have any interaction with those experiencing mental illness (Table 4b).
Bivariate analysis
Bivariate analysis with MAKS scores as a dependent variable showed higher scores in males compared with females (45.78 vs 42.53, p < 0.001). The highest mean scores were in the 31-40-year age group while the lowest knowledge scores were found in the 50+ age group (43.41 vs 40.64, p < 0.001).
Level of education was significantly associated with knowledge levels. Finishing secondary school was associated with higher knowledge (r = 0.36, p < 0.005). There were 70 (43%) participants with high school qualification who scored in the 50th percentile (moderate knowledge) and 68 (42%) in the 75th percentile (high knowledge) and 54 (52%) participants with tertiary education scored in the 75th percentile (high knowledge). In comparison to other groups, those with only a primary school level of education had the lowest level of knowledge and secondary education respondents had the highest scores (39.5 vs. 44.62). Furthermore, it was found that individuals who have been practising Christianity for 11-20 years displayed the highest level of knowledge. Bivariate analysis of CAMI scores shows that the male gender is associated with higher scores and more favourable attitudes compared with females (92.0 vs 80.7). Stigma is lowest in the 31-40- and 41-50-year age groups and highest in the 18-20 age group (75.9 vs 95.98).
There was no significant correlation between attitude and age or length of time as a Christian.
There was a statistically significant relationship between the level of education and attitude towards mental illness. A level of education beyond high school predicted a favourable attitude (r = 0.015 p < 0.005). Of the respondents who had completed matric (n = 163; 54.3%), 52 (31.5%) had high scores and 64 (39%) had medium scores indicating intermediate attitudes. Of respondents with tertiary education (n = 102), 34 (33%) had high scores and 55 (53%) had medium scores.
There is a weak correlation between MAKS and CAMI, with a Pearson correlation of r = 0.02, p < 0.005.
The male gender was also associated with favourable behaviour compared with female (14.63 vs. 11.15). Favourable intended behaviour was higher in older age groups. The lowest RIBS scores (lower favourable behaviour) were found in the adolescent group and highest in the 50+ and above age group (8.99 vs 15.44). Primary education is associated with less favourable behaviours compared with having tertiary education (8.33 vs. 14.35). Community Attitudes towards Mentally Ill Scale scores were positively correlated with RIBS scores (r = 0.594, p < 0.05). A favourable community attitude is correlated with a positive intended behaviour for participants.
Logistic regression analysis suggests that the number of years as a Christian was not predictive of the level of knowledge of mental illness and did not predict attitude significantly (p = < 0.005, r = 0.188); however, respondents' level of education was significantly predictive of greater knowledge (p < 0.005, r = 0.361). The tabulated results of the bivariate analysis can be seen in Table 5.

Dimensions of religiosity score
The majority of respondents had high scores above 80%, indicating a high level of religiosity. There is a negative correlation between level of religiosity and attitudes, Pearson correlation (r = -0.203, p < 0.005). A high level of religiosity is associated with unfavourable attitude towards mental illness. There is a negative correlation between RIBS and religiosity (r = -0.175, p < 0.005). There is no significant correlation between level of knowledge (MAKS) and level of religiosity.
Discussion
The results show that there is a moderate to high level of knowledge in this Christian community regarding mental illness. There appears to be a tolerant attitude towards the mentally ill which is correlated with a positive intended behaviour. A high level of knowledge is associated with a reduced stigma.
Knowledge
This study has shown moderate to high levels of mental health knowledge. These results differ from other African studies, which have shown low levels of mental health knowledge.21,22 In the study, factors that were associated with high knowledge were male sex, level of education beyond high school and young age.
The results indicate that being male is associated with higher knowledge. According to this research conducted, it was observed that male participants had a greater level of education beyond matriculation in comparison to their female counterparts. Moreover, the male participants were generally of a younger age, which could have led to their increased exposure to educational campaigns and mental health literacy. There was a similar result in a study by Birkie et al.22, which showed that females had poorer knowledge of mental illness compared with males; it is speculated that females could have lower levels of knowledge because they tend to minimise symptoms and underreport.22,23,24,25 Mental health literacy rather than gender was the strongest predictor of positive mental health knowledge and attitude in a study by Lee et al.23 Older females, however, had lower levels of knowledge and negative mental health attitude.26
Having completed secondary level education is associated with better knowledge. This may imply that mental health knowledge is improved by education. This result is in keeping with other studies which show that higher education is associated with higher knowledge.21,22 A study evaluating anti-stigma social campaigns in Ghana and Kenya revealed that there was a low level of knowledge of mental illness as baseline, with some improvement after educational campaigns.21 This result of high knowledge in this study could be because the majority of respondents in our study have a higher level of education (matric and tertiary education). Studies have speculated that individuals with a low level of education have a less ability to understand health information and they also have limited access to this information.22 While a similar study carried out in Ethiopia by Jarso et al. (different region) revealed poor knowledge towards mental illness, the majority of respondents in that study had low level of education with only 27% having tertiary education.27
The increase in age was associated with higher levels of knowledge. The highest levels of mental health literacy were observed among individuals aged 31 years - 40 years, followed by those aged 41 years - 50 years. Although previous studies have suggested that adults are generally less skilled at recognising mental illness, this study yielded a different outcome. However, the reason for this discrepancy remains unclear. Recent research suggests that young adults have a tendency to over-identify with depression,28,29 potentially because of increased exposure to mental health education through social media campaigns that aim to raise awareness about depression and suicide.30 Other studies had similar results where younger age was associated with a low level of knowledge and a low level of stigma related knowledge.21 Other studies found no association between age and level of knowledge.22,30
Help seeking attitude
The majority of participants showed a preference for a hospital in help-seeking. Respondents had a moderate to high level of knowledge about mental illness with an inclination to refer to professionals for treatment. This is consistent with previous studies, which demonstrate that high levels of knowledge influence help seeking that favours westernised methods of treatment, but this does not negatively influence the congregant's attitude towards people who are mentally ill.15,31,32
The majority of participants prefer hospitals, clinics or professional help when dealing with mental illness. The difference could be attributed to the higher levels of knowledge, which increases preference for Westernised treatment instead of traditional methods. Based on the research conducted by Hugo et al.,33 it appears that a majority of the participants find medication and psychotherapy to be effective in treating mental illness.
In South African studies, low levels of knowledge with high stigmatisation is a common finding and it is observed to be influencing help seeking negatively. According to Hugo et al., the preferred treatment is talk therapy as mental illness is viewed as being stress-related rather than a medical disorder.33 According to recent research, it has been found that only a quarter of church members would approach their pastor for assistance with mental health concerns.11,34 This suggests that there is a growing recognition of the biological aspects of mental illness and its influence on individuals' willingness to seek support.
This could be attributed to the beliefs about mental illness in the Christian context. However, the sample in this study is a small representation as there are many Christian followers and different denominations. Considering the representation sample, the results are not a conclusive representation; they can be viewed as an explorative view. As the knowledge of mental illness increases, there is also an increase in favourable attitudes in the community, that is, less stigma.
There were low levels of stigma related to mental health knowledge in our study. Furthermore, there was a high score of benevolence demonstrated towards the mentally ill people and this finding is consistent with previous studies. A study carried out in Ethiopia assessing knowledge and associated factors towards mental illness also showed poor knowledge of mental illness and moderate to high levels of unfavourable attitudes.22
Behaviour and attitudes
Our study shows that respondents have a favourable attitude towards the mentally ill. The high level of knowledge is associated with moderately favourable attitude. This is not in keeping with a study by Jarso et al., which showed that higher knowledge does not predict favourable attitudes. There is no association between good knowledge and negative attitudes.30 In a study by Birkie et al., poor knowledge was associated with unfavourable attitude, which is consistent with our findings.22 Most survey participants are willing to live with and work with individuals facing mental health challenges and maintain friendships with them. Familiarity and exposure to mental illness is associated with an increase in knowledge and less desire for restrictiveness and distancing from the mentally ill. Similarly, in our study there are favourable attitudes towards those who have mental illness even though there is a negative attitude towards mental illness itself; this can be explained by the high level of exposure to mental illness in this group. A study by Robinson that investigated patterns of change in knowledge, attitudes, and social distancing with people with mental illness over years during an anti-stigma campaign found that women demonstrated a significant decrease in stigma after campaigns, which was associated with increased exposure to and familiarity with people with mental illness.27
Level of religiosity
According to a study conducted by Potts and Henderson,21 individuals who identify as Christians exhibited lower levels of knowledge pertaining to mental illness when compared with non-religious populations and other religions. Conversely, those who reported having no religious affiliation displayed a more positive attitude towards mental illness. This study, however, did not find a correlation between level of religiosity and level of knowledge. This finding could be as a result of generally high religiosity in the study participants.
Conclusion
Through this research, insight into the knowledge, attitudes, and help-seeking behaviours of a particular Christian community was gained. Findings indicate that a considerable number of individuals in this population have been impacted by mental illness, indicating a potentially high incidence rate. The high knowledge in this Christian community is associated with a reduction in stigma and a positive attitude towards mental illness. If mental health awareness is encouraged, it helps to encourage positive help-seeking practices, tolerance, and treatment outcomes.
Recommendations
There is an importance for mainstreaming mental health in church programme to de-stigmatise mental illness. Active involvement of Christian organisations in providing families and carers of those with mental illness to increase familiarity and involvement will also help in destigmatising the mentally ill. The Church community can help with mental health advocacy and promotion.
Limitations
The study employed anonymous self-reported questionnaires, which may not fully represent the Christian population. A potential limitation could be neutral response bias, where participants may not feel comfortable expressing their true attitudes and may therefore provide untruthful reporting. In addition, self-report questionnaires could result in a loss of introspective ability and reporting bias. It is worth noting that the instruments used in the study have yet to be validated in the South African context, and the study only included one denominational cluster, which reduces the generalisability of the results. To address this, future studies should consider including other denominations.
Acknowledgements
The authors would like to acknowledge Dr V. Juby for her guidance, support, and encouragement during the formulation of this research idea and the church leadership, especially Dr M. Shabalala for their active involvement and assistance with data collection.
Competing interests
The authors declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
Authors' contributions
N.H. was the principal investigator conceptualising the study and research design, developed the protocol, performed data collection, supervised the project, assisted with study conceptualisation, protocol development, writing up of this project, and was responsible for data analysis. V.J. also assisted with the writing of the article and acted as supervisor.
Funding information
The authors received no financial support for the research, authorship or publication of this article.
Data availability
The data supporting the findings of this study are available from the corresponding author upon request.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1.Kessler RC, Aguilar-Gaxiola S, Alonso J, et al. The global burden of mental disorders: An update from the WHO World Mental Health (WMH) surveys. Epidemiol Psichiatr Soc. 2009;18(1):23. https://doi.org/10.1017/S1121189X00001421 [ Links ]
2.Henderson C, Evans-Lacko S, Thornicroft G. Mental illness stigma, help seeking, and public health programs. Am J Public Health. 2013;103(5):777-780. https://doi.org/10.2105/AJPH.2012.301056 [ Links ]
3.Cornah D. The impact of spirituality on mental health: A review of the literature. Mental Health Foundation [homepage on the Internet]. 2006 [cited n.d.]. Available from: https://www.elament.org.uk/self-help-resources/the-mental-health-foundation-the-impact-of-spirituality-a-literature-review/ [ Links ]
4.Saunders SM, Miller ML, Bright MM. Spiritually conscious psychological care. Prof Psychol Res Pract. 2010;41(5):355. https://doi.org/10.1037/a0020953 [ Links ]
5.Ramlall S, Naidu T. Talk therapy toolkit: Theory and practice of counselling and psychotherapy. Cape Town: Van Schaik; 2016. [ Links ]
6.Koening HG. Research on religion, spirituality, and mental health: A review. Can J Psychiatry. 2009;54(5):283-291. https://doi.org/10.1177/070674370905400502 [ Links ]
7.Salifu Yendork J, Kpobi L, Sarfo EA. 'It's only "madness" that I know': Analysis of how mental illness is conceptualized by congregants of selected Charismatic churches in Ghana. Ment Health Religion Cult. 2016;19(9):984-999. https://doi.org/10.1080/13674676.2017.1285877 [ Links ]
8.Rogers EB, Stanford M, Garland DR. The effects of mental illness on families within faith communities. Ment Health Religion Cult. 2012;15(3):301-313. https://doi.org/10.1080/13674676.2011.573474 [ Links ]
9.Gray AJ. Attitudes of the public to mental health: A church congregation. Ment Health Religion Cult. 2001;4(1):71-79. https://doi.org/10.1080/713685617 [ Links ]
10.Favazza AR. Modern Christian healing of mental illness. Am J Psychiatry. 1982;139(6):728-735. https://doi.org/10.1176/ajp.139.6.728 [ Links ]
11.Stanford MS, McAlister KR. Perceptions of serious mental illness in the local church. J Religion Disab Health. 2008;12(2):144-153. https://doi.org/10.1080/15228960802160654 [ Links ]
12.Abi Doumit C, Haddad C, Sacre H, et al. Knowledge, attitude and behaviors towards patients with mental illness: Results from a national Lebanese study. PLoS One. 2019;14(9):e0222172. https://doi.org/10.1371/journal.pone.0222172 [ Links ]
13.Cinnirella M, Loewenthal KM. Religious and ethnic group influences on beliefs about mental illness: A qualitative interview study. Br J Med Psychol. 1999;72(4):505-524. https://doi.org/10.1348/000711299160202 [ Links ]
14.McCullough ME, Weaver AJ, Larson DB, Aay KR. Psychotherapy with mainline protestants: Lutheran, Presbyterian, Episcopal/Anglican, and Methodist. In: Richards PS, Bergin AE, editors. Handbook of psychotherapy and religious diversity. American Psychological Association, 2000; p. 105-129. https://doi.org/10.1037/10347-005 [ Links ]
15.Stanford M, Philpott D. Baptist senior pastors' knowledge and perceptions of mental illness. Ment Health Religion Cult. 2011;14(3):281-290. https://doi.org/10.1080/13674670903511135 [ Links ]
16.Moreno AN, Bartkowiski JP, Xu X. Religion and help seeking: Theological conservatism and preferences for mental health assistance. Religions. 2022;13(5):413. https://doi.org/10.3390/rel13050415 [ Links ]
17.Evans-Lacko S, Little K, Meltzer H, et al. Development and psychometric properties of the Mental Health Knowledge Schedule. Can J Psychiatry. 2010;55(7):440-448. https://doi.org/10.1177/070674371005500707 [ Links ]
18.Evans-Lacko S, Rose D, Little K, et al. Development and psychometric properties of the Reported and Intended Behaviour Scale (RIBS): A stigma-related behavior measure. Epidemiol Psychiatr Sci. 2011;20(3):263-271. https://doi.org/10.1017/S2045796011000308 [ Links ]
19.Taylor SM, Dear MJ. Scaling community attitudes toward the mentally ill. Schizophr Bull. 1981;7(2):225. https://doi.org/10.1093/schbul/7.2.225 [ Links ]
20.Joseph S, DiDuca D. The dimensions of religiosity scale; 20-item self report measure of religious preoccupation, guidance, conviction, and emotional involvement. Ment Health Religion Cult. 2007;10(6):603-608. https://doi.org/10.1080/13674670601050295 [ Links ]
21.Potts L, Henderson C. Evaluation of anti-stigma social campaigns in Ghana and Kenya: Time change global. BMC Public Health. 2021;21(1):886. https://doi.org/10.1186/s12889-021-10966-8 [ Links ]
22.Birkie M, Anbesaw T. Knowledge, attitude and associated factors toward mental illness among residents of Dessie town, Northeast Ethopia cross, sectional study. BCM Psychiatry. 2021;21(1):61. https://doi.org/10.1186/s12888-021-03609-0 [ Links ]
23.Lee HY, Hwang J, Ball JG, et al. Mental health literacy affects mental health attitude: Is there a gender difference? Am J Health Behav. 2020;44(3):282-291. https://doi.org/10.5993/AJHB.44.3.1 [ Links ]
24.Lefevor TG, Paiz JY, Milburn HE, et al. Religiousness and help seeking: Individual, congregational and clergy factors. Couns Psychol Q. 2022;35(1):89-109. https://doi.org/10.1080/09515070.2021.1874297 [ Links ]
25.Copeland-Linder N. Stress among Black women in a South African township: The protective role of religion. J Commun Psychol. 2006;34(5):577-599. https://doi.org/10.1002/jcop.20116 [ Links ]
26.Okafor IP, Oyewale DV, Ohazurike C, Ogunyemi AO. Role of traditional beliefs in the knowledge and perceptions of mental health and illness amongst rural -dwelling women in Western Nigeria. Afr J Prim Health Care Fam Med. 2022;14(1):e1-e8. https://doi.org/10.4102/phcfm.v14i1.3547 [ Links ]
27.Robinson EJ, Henderson C. Public knowledge, attitudes, social distance and reporting contact with people with mental illness 2009-2017. Psychol Med. 2019;49(16):2717-2726. https://doi.org/10.1017/S0033291718003677 [ Links ]
28.Lund C, Fisher AJ. Community/hospital indicators in South African public sector mental health services. J Ment Health Policy Econ. 2013;6(4):181-187. [ Links ]
29.Peltzer K. Religiosity, personal distress and minor psychiatric morbidity among Black students in South Africa. Soc Behav Pers. 2005;33(7):723-733. https://doi.org/10.2224/sbp.2005.33.7.723 [ Links ]
30.Jarso MH, Debele GR, Gezimu W, Nigan D, Mohammedhussein M, Jamal K. Knowledge, attitude and its correlates of the community toward mental illness in Mattu, South West Ethiopia. Front Psychiatry. 2022;13:1018440. https://doi.org/10.3389/fpsyt.2022.1018440 [ Links ]
31.Webb M. Toward a theology of mental illness. J Religion Disab Health. 2012;16(1):49-73. https://doi.org/10.1080/15228967.2012.645608 [ Links ]
32.Hartog K, Gow KM. Religious attributions pertaining to the causes and cures of mental illness. Ment Health Religion Cult. 2005;8(4):263-276. https://doi.org/10.1080/13674670412331304339 [ Links ]
33.Hugo CJ, Boshoff DE, Traut A, Zungu-Dirwayi N, Stein DJ. Community attitudes toward and knowledge of mental illness in South Africa. Soc Psychiatry Psychiatr Epidemiol. 2003;38(12):715-719. https://doi.org/10.1007/s00127-003-0695-3 [ Links ]
34.Darroch K. An investigative study of the influence of religion on help seeking behaviours in the field of mental health: Rowan digital works. New Jersey: NJ: Rowan University; 2011. [ Links ]
 Correspondence:
Correspondence:
Nomthandazo Hlongwane
nkosazane@yahoo.com
Received: 28 June 2023
Accepted: 24 Aug. 2023
Published: 07 Nov. 2023

Figure 1-A1 - Click to enlarge

Figure 2 - A1 - Click to enlarge


{kind=link}
{kind=link}
{kind=link}