










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Childhood Education
On-line version ISSN 2223-7682Print version ISSN 2223-7674
SAJCE vol.13 n.1 Johannesburg 2023
https://doi.org/10.4102/sajce.v13i1.1172
ORIGINAL RESEARCH
Teacher awareness of psychosocial support available as per the Integrated School Health Policy in South Africa
Jace PillayI; Leila PatelII; Rubina Setlhare-KajeeIII
ISouth African Research Chair in Education and Care in Childhood, Faculty of Education, University of Johannesburg, Johannesburg, South Africa
IIDepartment of Social Work, Faculty of Humanities, University of Johannesburg, Johannesburg, South Africa
IIIDepartment of Educational Psychology, Faculty of Education, University of the Western Cape, Cape Town, South Africa
ABSTRACT
BACKGROUND: In 2012, the South African government initiated the Integrated School Health Policy (ISHP) to serve as a national guideline on providing school health and support services from key stakeholders such as the Department of Health (DoH), Department of Basic Education (DBE) and Department of Social Development (DSD). However, despite the ISHP regulations, publications report that teachers in under-resourced government schools are not sufficiently equipped to address their learners' psychosocial challenges.
AIM: This study aimed to assess which psychosocial interventions implemented at the schools the school teachers are aware of.
SETTING: A total of 50 school teachers from five under-resourced primary schools in Gauteng school communities of Meadowlands, Ivory Park, Alexandra and Doornkop-Soweto completed a feedback questionnaire designed by the investigators.
METHODS: This descriptive study follows a quantitative descriptive design. A comparative descriptive analysis between schools using frequencies, percentages and graphs was used to analyse the results.
RESULTS: Results indicate that a school teachers' ability to support their learners varies per school and is based on their school's compliance to training their teachers on the school safety protocols and is not affected much by external training. Schools that follow the ISPH regulations on teachers' training of protocols, better equip their teachers to observe psychosocial challenges their learners face.
CONCLUSION: Despite the availability of guidelines, this study observes a gap in educators' observations of mental health concerns or external stakeholders responsible for non-physical assistance.
CONTRIBUTION: Findings of this study provide feedback to all relevant stakeholders to assist in their future recommendations planning. One recommendation the authors of this study suggest may be that further studies explore if the lack of mental health observations is a result of poor teachers-student relations or a need for school teachers to be educated on learner mental health risk factors.
Keywords: psychosocial support; psychosocial challenges; primary schools; under resourced; educator training; teachers feedback; children; Africa.
Introduction
Under-resourced South African schools are still undergoing various psychosocial stressors that affect their children and teachers' well-being (Setlhare, Wood & Meyer 2016). The most pertinent psychosocial stressors children face relate to family concerns of poverty, absent parents, domestic violence, parents' physical health and parents' mental health (Stats SA 2018); negative environmental factors in the schools such as gangsterism, bullying and stigma (Setlhare et al. 2016); personal factors such as teenage pregnancies and substance abuse (Department of Basic Education 2013) and lastly personal mental health factors of Attention Deficit Hyperactivity Disorder (ADHD), learning disorders (Grosser 2016), depression, anxiety and suicide ideation (Strydom, Pretorius & Joubert 2012). As a response to support schools in improving the overall well-being of their children and the community around them, the South African government initiated the Integrated School Health Policy (ISHP) in 2012 (South Africa 2012). The ISPH serves as a national guideline on the provision of school health and support services (South Africa 2012), just as has been done in other African countries, with the collaboration of various key stakeholders such as the Department of Health (DoH), Department of Education and Department of Social Development (DSD) with the school and its teachers (Rasesemola, Matshoge & Ramukumba 2019). To ensure that school teachers and learners are well supported, each school is responsible for ensuring the school teachers are up-to-date on the school safety policies and the ISHP (South Africa 2012). However, despite the ISHP regulations in place, some publications indicate that teachers in under-resourced government schools are not sufficiently equipped to address their learners' psychosocial challenges (eds. Donald et al. 2014; Setlhare et al. 2016; Spaull 2013). This study aims to establish the level of knowledge of the ISHP among the school teachers with a focus on the level of information and insights the school teachers have in terms of psychosocial challenges their learners face and the child-well-being interventions available to them at their schools, as provided by the Departments of Social Welfare, Health and Education.
Research feedback on psychosocial challenges observed in schools
In a recent population assessment of youth suicidal behaviour in South Africa, statistics confirm that approximately 22% of black South African youths endorsed suicide ideation or attempted suicide (Thornton, Asanbe & Denton 2019). The study reported that, on average, the country faces a range of 4.2% - 15.6% of adolescents engaging in suicidal ideation, 2.4% - 12.5% plan an attempt and 1.9% - 6.3% follow through on a suicide attempt (Thornton et al. 2019). The road to suicidal ideation is linked to depression and anxiety. Strydom et al. (2012) indicate that a substantial number (61.2%) of learners suffer from anxiety to varying degrees, which is much higher than the adult prevalence of anxiety in South Africa. Comparatively, they also report the prevalence of depression among learners to be only 19.7%. Even though the prevalence of depression is not as high as anxiety, it should be regarded as a cause for concern as it is higher than the 10% prevalence of depression among South African adults. In addition to the abovementioned mental health challenges, approximately 9620 (0.4%) children in Gauteng report to also be suffering from learning disabilities that serve as a psychosocial challenge (Department of Basic Education 2013; Grosser 2016).
Domestic instability, such as poverty, is one of the greater risk factors attributing to the children's psychosocial challenges (South Africa and Department of Education 2008). In 2015, three of five children (62.1%) aged 0-17 years were multi-dimensionally poor (Stats SA 2018). Additionally, children coming from households of adverse living conditions suffer from malnutrition, due to which 18% of South African school students present with stunted growth, 9.3% are underweight, 20% are overweight and 5.34% fall under the category of obese (Labadarios et al. 2005; Mafugu 2021; Okeyo et al. 2020). Another domestic instability of absent parents (19.8%) where children lived with neither their biological parents nor children with absent fathers (43.1%) also plays a significant role in adding to the psychosocial challenges the children face, for which they require interventions and support from schools and the government departments (Stats SA 2018).
In addition to mental health and domestic challenges, most under-resourced schools are also not safe from violence through gangsterism (South Africa and Department of Education 2008) and significant problems of sexual abuse (30%) and gender-based violence (Department of Basic Education 2018). Due to the prevailing violence and gangsterism in schools, recent statistics indicate that 21% of learners smoke tobacco at least once a month, and approximately 35% of learners consume alcohol at least once a month (Department of Basic Education 2013).
South African children, therefore, face various concerns related to mental health, poverty, domestic instability, violence in their schools and communities, abuse in their homes and schools and substance abuse.
The guidelines of the Integrated School Health Policy of 2012
Due to the various overlapping psychosocial challenges that learners simultaneously face, many South African teachers feel they are not sufficiently equipped to support their learners (Setlhare et al. 2016; South Africa and Department of Education 2008). As a response to the schools' needs for an integrated set of guidelines to support their learners, South Africa published the ISHP to serve as a national guideline on providing school health and support services (South Africa 2012). Key stakeholders include the DoH, Department of Education and DSD (Rasesemola et al. 2019; South Africa 2012). The ISHP was developed based on international evidence confirming that successful psychosocial school programme implementations depend on solid relationships between government, private sector, academic institutions, community, NGOs and other service providers such as the police (South Africa 2012; Stats SA 2018). The World Health Organization (WHO), an example of international evidence, established several multidisciplinary and collaborative healthcare approaches for schools within various parts of Europe, which have proven vital in advocacy for school health policies and programmes in many countries (Rasesemola et al. 2019). Implementation of the ISHP requires the successful multisectoral collaboration of the key role players. These role players and the school support structures such as the school governing bodies (SGB), learner organisations, learning support educator (LSE) and school-based support teams (SBST) are expected to contribute to the development of sustainable school health programmes (Rasesemola et al. 2019). Unfortunately, a recent study indicates that a widespread non-compliance of schools with integration and collaboration with different stakeholders for the delivery of the psychosocial support interventions (Rasesemola et al. 2019); however, a dearth of research exists on school teachers' feedback on the psychosocial challenges and interventions available to them. This study aims to see the level of insights the school educators have regarding psychosocial challenges learners face and the support interventions available at their schools to assess their compliance with the ISHP regulations.
According to the ISHP (South Africa 2012), the key government stakeholders involved are the National Departments of Basic Educations (DBE), the DSD and the DoH (South Africa 2012). The DBE is generally responsible for providing education tools and psychological support to schools and ensuring stakeholders needed for learner safety are partnered with. The DSD assists with the provision of social workers responsible for catering for children undergoing domestic instability and mental health concerns. The DoH provides free healthcare check-ups and vaccinations for all children to ensure adequate health for learning (South Africa and Department of Education 2008). Each National Department's partnership is regulated with the assistance of the provincial departments and the districts within each provincial department. The provincial departments oversee collaborations with external key stakeholders such as the South African Police Service (SAPS) and private sectors. The districts are responsible with ensure all schools have functioning SBSTs and that the principals, SGBs, educators and support teachers are familiar with the ISHP protocol and that the schools adhere to this protocol and use the prescribed monitoring tools appropriately.
The ISHP (South Africa 2012) also provides details of the school-based key stakeholders involved in supporting their learners. The principals are responsible for keeping relations with the district and NGOs that provide the school with assistance via the school feeding scheme, uniforms and other services. The principal is also responsible for ensuring the School Management Team (SMT), SGB and school teachers are aware of their responsibilities and are aware of the protocols in place to protect their children, among other duties. The SMT and SGB report to the principal and are responsible for safety plans, policies, discipline and problematic learners' assistance. The SBST, educators and learners are also considered stakeholders responsible for reporting on psychosocial challenges they observe in their learners to the SGB.
Lastly, the ISHP (South Africa 2012) requires the national and school bodies to partner with the community, NGOs, the SAPS and the South African Council for Educators (SACE) as key stakeholders in the provision of additional services that are actively responsible for the safety and support of the learners from the adverse psychosocial challenges. Particularly in concerns related to poverty and sexual abuse, the NGOs and SAPS are considered vital in protecting their learners. Table 1 provides a breakdown of stakeholders involved with various psychosocial challenges.

Methodology
A non-experimental descriptive quantitative design was followed for the data collection and analysis of this investigation. A total of 50 school staff, inclusive of principals, educators in the SBST and teachers were purposively recruited from five public primary schools registered under the second quintile in low-income communities in the Gauteng school communities of Meadowlands, Ivory Park, Alexandra and Doornkop-Soweto. All teachers' members enrolled at the school for more than 6 months were eligible for the study. Due to the coronavirus disease 2019 (COVID-19) restrictions at the schools, only 50 participants were assessed for the study. However, the study only reports on four of the schools as only one educator was assessed from School 5.
The investigators designed a feedback questionnaire to gather information on participants' demographic characteristics and insights on observed psychosocial challenges and child-wellbeing interventions implemented in their schools. The surveys included four open background questions on their position, time spent at the school, subjects taught and any additional psychosocial training received. These were followed by 15 binary close-ended questions for psychosocial challenges observed and four open-ended questions on their insights on the psychosocial interventions implemented and the organisations involved. The last question allowed feedback on any additional interventions the educators can propose that may address ongoing concerns at school and who they think should be responsible for its implementation. No items were reverse scored. The investigators reviewed the questionnaire for the face validity of the items and questions.
Approval for the study was obtained from the Ethics Committee of the Faculty of Humanities at the University of Johannesburg. Permission was also obtained from the Department of Education and the principals of the schools involved. Potential participants received information leaflets and consent forms at their schools. Participants were informed that participation was voluntary and anonymous, meaning that all personal information would be kept strictly confidential and could not be linked to any specific individual. Questionnaires were completed during the school day and were collected by the investigators. All information was coded into an Excel spreadsheet and saved on a password-protected computer.
Data were analysed using SPSS v.25 for descriptive data analysis for the trends observed generally and between schools. The open-ended questions were analysed for their content to create descriptive graphs. Frequencies and percentages were used to summarise results and compare them between schools. The study results analysis was divided into three parts to effectively answer the research question to compare the psychosocial challenges faced and interventions implemented. All data assessment was conducted by comparing schools as each school is responsible for ensuring the school teachers are up-to-date on the school safety policies and the ISHP (South Africa 2012).
Ethical considerations
Ethical clearance to conduct this study was obtained from the University of Johannesburg Faculty of Humanities Research Ethics Committee (No. RED-01-050-2020).
Results
Fifty forms were returned with more than 80% completion of the questionnaire. One school only had one respondent and was consequently removed from the analysis of the data. Only 49 questionnaires were analysed for in-depth insights into school teachers' members' awareness of psychosocial interventions implemented at schools and the challenges the learners face. Table 2 summarises the respondents' demographic data, indicating that 82% of the respondents were teachers and only 42% of the total respondents received additional training on psychosocial services offered at schools via external workshops.

School 1 had 10 of the 12 respondents (83.3%) who had received additional psychosocial training in terms of additional training received by personnel. Followed by School 3, nine of the 28 respondents (32.1%) received additional training. However, Schools 2 and 4 only had one trained respondent from each school (16.7% and 33.3%, respectively).
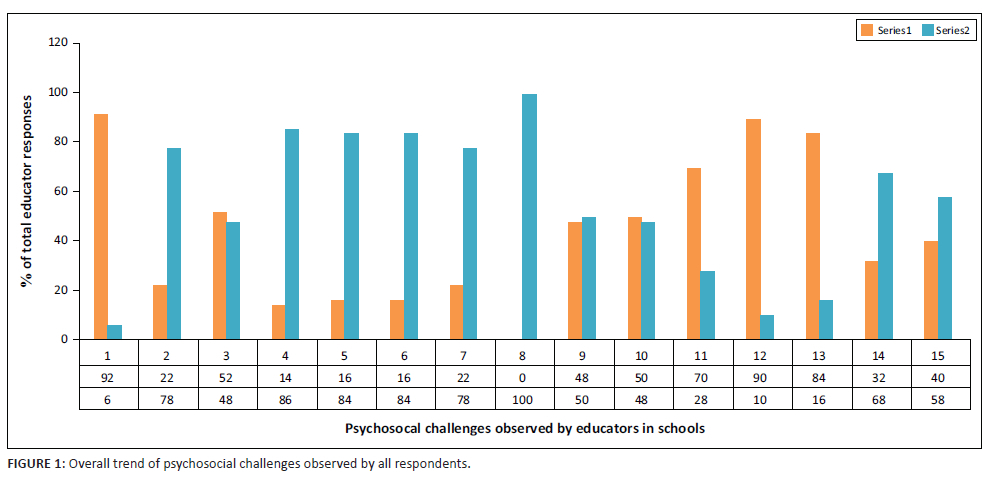
The first set of analysis describes which psychosocial challenges are prevalent in the schools as a whole - followed by a graphic comparison of the psychosocial challenges faced by each school, respectively. A comparative descriptive analysis of the psychosocial challenges observed by the school teachers is entered graphically in Figure 1 and Figure 2. Figure 1 illustrates the overall trend of psychosocial challenges observed from all the respondents, and Figure 2 illustrates a comparative graph of the psychosocial challenges experienced by each school, respectively.
Figure 1 indicates that overall, the biggest concerns observed relate to absent parents, poverty, learning challenges affecting self-esteem and bullying. Suicide ideation is not observed as a psychosocial challenge in all schools.
Additional feedback from an open-ended question reports that additional psychosocial problems observed are conduct disorder (4%), eating disorders (8%), impact of COVID-19 on family structures (8%), impact of HIV on family structures (4%), general lack of self-esteem (2%) and unresolved anger due to absent parents (8%).
The second approach to the descriptive analysis was to statistically compare schools on their feedback of the psychosocial interventions implemented and the departments and organisations involved in implementing learner support. These findings provide insights into if the schools follow procedures to educate their teachers members on ISHP processes.
Interventions and/or programmes that provide psychosocial support to learners
School 1 reported that they only received psychosocial support from social workers and the SBST (16.7%), of which 91.7% of the educators from School 1 reported that social workers provided psychosocial support to learners at the schools, and 16.7% of the educators acknowledged the role of the SBST in supporting students. The questionnaires asked educators to mention all providers of psychosocial support to learners from external bodies and from within the school. As teachers can also be providers of psychosocial support, the document implied that teachers too can be considered. However, the majority of the teachers' responses only acknowledged the support provided by social workers, despite the fact that 83.3% of them are trained in providing psychosocial support to learners within the school system.
Comparatively, School 2's teachers reported a significant amount of assistance from the DSD, which worked in collaboration with NGOs to add to the school's nutrition programme (66.7%), which is also part of the school health programme. As indicated in Table 1, the ISHP indicates that the problem of nutrition can be supported and provided for by NGOs, the School Feeding Scheme project, or district support teams, indicating that the DSD is assisting with the ISHP programme as a whole. School 2's teachers also acknowledge counselling services provided by other mental health practitioners in the area (50%), the SBST for providing support to troubled learners (33.3%) and the health clinics in the area who send nurses for vaccinations and check-ups (16.7%). As such, School 2 indicated more knowledge on the various stakeholders involved in providing psychosocial support to students despite only 16.7% of their teachers' members undergoing extra training on psychosocial support provided to the schools.
Responses from School 3 provided the most in-depth feedback of all the schools. In terms of key stakeholders, 36% of the teachers acknowledge the involvement of each key stakeholder, such as the DSD in the provision of social workers, the DoH in providing support from clinics and nurses and the SAPS. Approximately 39% of the educators emphasised the availability of the Support Needs Assessment (SNA) form, which is part of a programme provided by the DBE to assess and provide psychological support to the learners in need. School support is reported in terms of the availability of the SBST (32%), the SGB (11%) and the LSE educators (18%). Lastly, School 3 acknowledges the community key role players such as NGO's who assist with the feeding schemes and uniforms (4%), as well as the key involvement of parents in supporting their children (8%). Similarly, School 4 is 100% aware of the role of key stakeholders such as the NGOs, DoH, DSD, SAPS and DBE.
School 4 reports that the District Based Support Teams (DBST), the SAPS and psychologists or counsellors are involved in providing at least 33.3% of the psychosocial support for learners. Comparing to all schools, School 4's reported the highest learner support received from DBST's and psychologists.
How are the interventions implemented?
Regarding how interventions are implemented, findings on this question seemed slightly shifted for three of the four schools from their responses on which interventions or programmes provide psychosocial support. School 1's responses indicate a complete focus (100%) only on how the DoH organised for nurses and health practitioners to come to school to check the learners' health and provide them with injections. School 2 provided more diverse responses than School 1; they acknowledged the assistance of NGOs with the school feeding programme (67%), the assistance of the SBST with academic, behavioural problems (33%) and the role of the government departments mentioned above with the allocation of social workers (17%), nurses (33%) and mental health practitioners (33%). Similar to Schools 1 and 2, School 4 also indicates some shift in insights, narrowing only the DSD (33%) and the counselling services they provide, the SAPS (33%) and the DoH for its health talks (33%). Comparatively, School 3 provides responses on how interventions are implemented, consistent with the programmes involved in implementing the interventions. Approximately 18% of the respondents acknowledge the nutrition and feeding schemes provided by the NGOs that try to assist learners who are needy or coming from disadvantaged families with food parcels and school uniforms. The LSE educators support learners with special needs (11%) and work with different departmental professionals to promote inclusive education through training (11%). In terms of school support, the SBST support learners dealing with troubles at home or elsewhere (14%) and inform parents of the troubles their children face and the steps needed to support their children, whereas the SGB assists with absent parents (7%). Consistent with their educated insights, School 3 teachers also indicate that the SAPS assists with domestic violence and substance abuse cases (4%); social workers from the DSD assist troubled children facing concerns of parental mental health (4%) and address learners on the issue of substance abuse, teenage pregnancy and any other social support they need (11%). Lastly, the DoH provides support through clinics that aid in vaccinations and health checks for the children (14%).
Organisations and structures involved in intervention implementation
The following section indicates the results using two separate graphs. The first graph is a direct depiction of the organisations the schools indicated are involved in implementing the interventions and psychosocial programmes. Figure 3 illustrates an evident lack of acknowledgement of SBSTs, SGBs and LSE educators by all schools other than School 3. Additionally, no schools seem to acknowledge the DBE as an organisation responsible for psychosocial support in schools. Additionally, Schools 1 and 2 do not acknowledge psychological and counselling organisations involvement in their roles of psychosocial support.
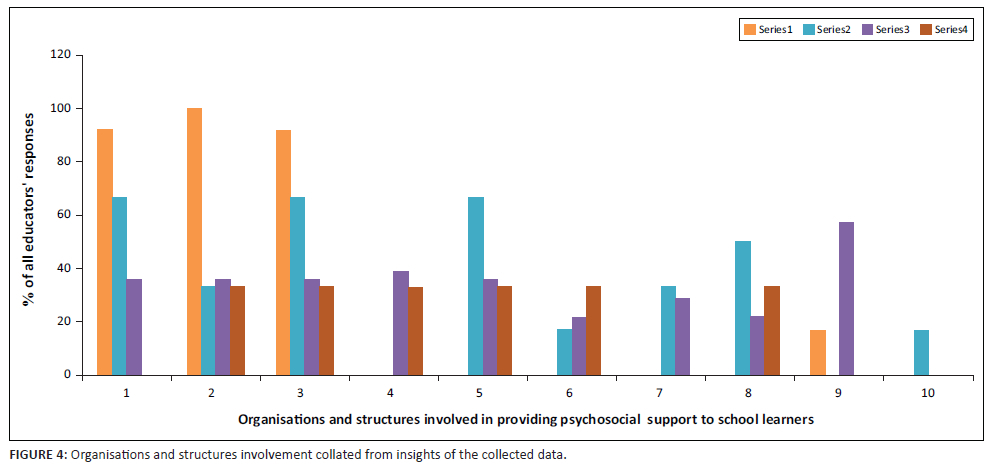
Comparatively, Figure 4 illustrates the involvement of all key stakeholders, as calculated using content analysis from the overall responses received for all the questions. Figure 4 indicates that despite 83% of teachers undergoing extra psychosocial training in School 1, their insights are limited to the involvement of NGOs, the DoH and the DSD. Schools 1 and 4 do not seem to acknowledge the importance and support of SBSTs in their schools. Overall, the support provided in schools by the DBE, school support systems and psychological support is acknowledged the least by all schools.
Discussion
This discussion reflects on the insights from the cross-examination of the observations in psychosocial challenges and interventions reported by the four schools to identify additional gaps where teachers members need to be educated on the ISHP regulations and the involvement of various stakeholders. The most prominent observation is that Schools 1 and 2 have an adequate level of external training on psychosocial support interventions; however, their responses on psychosocial interventions do not reflect a holistic training on all the key stakeholders and programmes available at the schools. Reflections on the questions asked indicate that the question's wording may not be responsible for the limited information provided by these two schools in the responses. Schools 3 and 4 understood the questions well and provided feedback indicating a well-educated teacher on the psychosocial interventions implemented by the key stakeholders involved. Schools 3 and 4 cover 62% of the total sample, and approximately 32% of the teachers in this sample partook in extra training compared with 82% of School 1. The responses seem to indicate that the school teachers are only as well equipped as the knowledge and training they receive from their school on the ISHP regulations of key stakeholders and their roles and responsibilities. According to the ISHP, schools' district support and principals are responsible for ensuring that all schools have functional SGB and SMTs and that all teachers are educated on the ISHP protocol. Findings indicate that not all schools are following policy protocol in educating all teachers on the psychosocial support available.
Regarding the observed psychosocial challenges, the descriptive comparisons between schools indicate that all the schools follow a similar trend on challenges observed. Psychosocial challenges such as absent parents (92%), poverty (90%), learning challenges (84%) and bullying (N = 70) were the most observed and reported by the respondents. However, substance abuse (22%), gangsterism (14%), teen pregnancies (16%), depression (16%) and anxiety (22%) were marked as the lowest challenges faced in the schools. Psychosocial challenges related to family show close to a 50% challenge in schools, such as domestic violence (52%), parental physical health (48%) and parental mental health (32%). However, teachers from all schools did not report suicide ideations among learners. These observations run contrary to the South African statistics of approximately 12.5% of all learners in South African public primary schools consider suicide at least once (Stats SA 2018). Additionally, in School 2, with 33% of the teachers who partook in external psychosocial training, observed no challenges of substance abuse, gangsterism and teenage pregnancy. These observations also run contrary to South African statistics where more than 30% of school learners face sexual abuse (Department of Basic Education 2018) and the schools face significant concerns of gangsterism and violence (South Africa and Department of Education 2008). One justification for this possible lack of insights on matters of mental health, sexual abuse and violence could be the high learners to teachers ratio, which in 2020 was reported to be an average of 1:36 in secondary schools (Botha 2020). With such high learners to teachers ratio, teachers and learners relations are negatively affected and significantly reduce learners' trust in teachers and learners' achievement (Koc & Celik 2015). As such, we may have to conclude that the high learners to teachers ratio in our public secondary schools reduce the chances of students approaching educators for assistance and that schools may need to consider introducing team-building exercises where learners and teachers interact in a manner that can slowly build trust and create a bond where learners reach out with their problems and concerns.
In terms of psychosocial interventions - in addition to the lack of school teachers' education on the ISHP regulations of key stakeholders and their roles and responsibilities - we observe a trend of overlooking the roles of stakeholders responsible for psychological support and support structures in schools. Findings indicate that although some teachers recognise the importance of caring for learner mental health, greater emphasis is given to physical health concerns relating to the learners' feeding schemes and medical health. As such, responses indicate that workshops need to be introduced, which acknowledge the organisations involved in providing counselling support, as well as the importance of caring for learner mental health and associated red flags.
Reflecting on the findings, the first recommendation would be to introduce students to the ISHP process and information steadily. This may assist in educating the students and can lead to learner buy-in in reporting to the correct authorities when concerns arise. Additionally, students may benefit from an information session, which focuses on the main areas of psychosocial concern (i.e. mental health problems, absent parents, poverty, learning challenges and bullying), and be educated on which support structures are in place, so that both learners and educators know how to use the ISHP protocol to its full effect.
Limitations of this study are the limited sample, due to which the results cannot be considered generalisable. Additionally, due to the open-ended nature of specific questions, the reliability could not be assessed. Although responses indicate adequate face validity of the questions, a rigorous validity check of the questionnaire may be beneficial for future explorations.
Conclusion
This study aimed to see the level of information and insights the school educators had regarding psychosocial challenges their learners faced and the child well-being interventions available to them at their schools provided by the DSD, DoH and DBE. Despite attending some external training on psychosocial interventions, the results indicate that school teachers lacked basic knowledge and insights on the psychosocial interventions and key stakeholders involved, as per the ISHP. Schools that conform to the requirements of educating their teachers on the ISHP regulations and maintaining transparent school support structures of the SGB and SBST equip their teachers with the tools they need to support their learners adequately. However, a general concern that remains is the lack of focus or observations on the psychological risk factors of gangsterism, substance abuse and teenage pregnancies of the students who may be at risk of suicide ideations. Findings of this study provide feedback to all relevant stakeholders to assist in their future recommendations planning. One recommendation the authors of this study suggest may be that further studies explore if the lack of mental health observations is a result of poor teachers-student relations or a need for school teachers to be educated on learner mental health risk factors. Teachers can only be equipped to handle psychosocial concerns at school through continuous knowledge and training.
Acknowledgements
The authors would like to acknowledge the contributions of Maham Hasan from Crescent Consultancies for her assistance with the data analysis of the article. The multiple research partners enabled access and provided invaluable support in data collection and implementation of intervention activities.
Competing interests
The author(s) declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
Authors' contributions
All authors were responsible for the conceptualisation, data analysis, reviewing and editing of the article. J.P. was responsible for the methodology, writing, investigation and project administration related to the article. All authors approved the submission of the manuscript.
Funding information
This work was funded by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation of South Africa. South African Research Chair, Education and Care in Childhood, Faculty of Education, University of Johannesburg South Africa. Grant Number: 87300.
Data availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to restrictions.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
Botha, L., 2020, Teacher absenteeism & learner/teachers ratio at schools in the province, YouTube, viewed 15 September 2021, from https://www.youtube.com/watch?v=nnPhlE6qTEM.
Department of Basic Education, 2013, Drug national strategy: For the prevention and management of alcohol and drug use amongst learners in schools, Department of Basic Education, Pretoria.
Department of Basic Education, 2018, Protocol on sexual abuse and harassment in schools. Department of Basic Education, Pretoria.
Donald, D., Lazarus, S., & Moola, N. (2014). Educational psychology in social context: Ecosystemic applications in Southern Africa, 5th edn., Oxford University Press, Oxford.
Grosser, M.M., 2016, 'An appreciation of learning disabilities in the South African context', Learning Disabilities 14(1), 79-92. [ Links ]
Koc, N. & Celik, B., 2015, 'The impact of number of students perteachers on student achievement', Procedia - Social and Behavioral Sciences 177, 65-70. https://doi.org/10.1016/j.sbspro.2015.02.335 [ Links ]
Labadarios, D., Steyn, N.P., Maunder, E., Macintryre, U., Gericke, G., Swart, R. et al., 2005, 'The National Food Consumption Survey (NFCS): South Africa', Public Health Nutrition 8(5), 533-543. https://doi.org/10.1079/PHN2005816 [ Links ]
Mafugu, T., 2021, 'Challenges encountered in a South African school nutrition programme', Journal of Public Health Research 10(1), 1-8. https://doi.org/10.4081/jphr.2021.1982 [ Links ]
Okeyo, A.P., Seekoe, E., De Villiers, A., Faber, M., Nel, J.H. & Steyn, N.P., 2020, 'The food and nutrition environment at secondary schools in the Eastern Cape, South Africa as reported by learners', International Journal of Environmental Research and Public Health 17(11), 4038. https://doi.org/10.3390/ijerph17114038 [ Links ]
Rasesemola, R.M., Matshoge, G.P. & Ramukumba, T.S., 2019, 'Compliance to the integrated school health policy: Intersectoral and multisectoral collaboration', Curationis 42(1), 1-8. https://doi.org/10.4102/curationis.v42i1.1912 [ Links ]
Setlhare, R., Wood, L. & Meyer, L., 2016, 'Collaborated understandings of context-specific psychosocial challenges facing South African school learners: A participatory approach', Educational Research for Social Change 5(2), 18-34. https://doi.org/10.17159/2221-4070/2016/v5i2a2 [ Links ]
South Africa, 2012, Integrated school health policy, Department of Health and Department of Basic Education, viewed 28 April 2021, from https://serve.mg.co.za/content/documents/2017/06/14/integratedschoolhealthpolicydbeanddoh.pdf.
South Africa and Department of Education, 2008, National strategy on screening, identification, assessment and support: School pack, Department of Education, Pretoria.
Spaull, N., 2013, 'Poverty & privilege: Primary school inequality in South Africa', International Journal of Educational Development 33(5), 436-447. https://doi.org/10.1016/j.ijedudev.2012.09.009 [ Links ]
Stats SA, 2018, Children's education and well-being in South Africa, 2018, Statistics SA, pp. 1-89, viewed 17 May 2021, from http://www.statssa.gov.za/publications/92-01-07/92-01-072018.pdf.
Strydom, M.A.A., Pretorius, P.J. & Joubert, G., 2012, 'Depression and anxiety among Grade 11 and 12 learners attending schools in central Bloemfontein', South African Journal of Psychiatry 18(3), 5. https://doi.org/10.4102/sajpsychiatry.v18i3.356 [ Links ]
Thornton, V., Asanbe, C. & Denton, E.-G., 2019, 'Clinical risk factors among youth at high risk for suicide in South Africa and Guyana', Depression and Anxiety 36. https://doi.org/10.1002/da.22889 [ Links ]
 Correspondence:
Correspondence:
Jace Pillay
jacep@uj.ac.za
Received: 11 Jan. 2022
Accepted: 02 Nov. 2022
Published: 03 Feb. 2023

{kind=link}
{kind=link}
{kind=link}
{kind=link}