










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Industrial Engineering
On-line version ISSN 2224-7890
S. Afr. J. Ind. Eng. vol.36 n.1 Pretoria May. 2025
https://doi.org/10.7166/36-1-2999
GENERAL ARTICLES
The State of Lean and Quality Improvement Methodologies in the South African Healthcare Sector: A Systematic Literature Review
S. Kazadi; O. Olanrewaju
Department of Industrial Engineering, Durban University of Technology, Durban, South Africa
ABSTRACT
Even though South Africa has developed a policy document on quality in the healthcare sector, the quality of service delivery continues to deteriorate. This study aimed to explore the application of lean and quality improvement (QI) methodologies in South African healthcare organisations, focusing on the periods before and after the introduction of the policy document. Using a systematic literature review (SLR) guided by the preferred reporting items for systematic reviews and meta-analysis (PRISMA) flowchart, 17 relevant studies were analysed from a total of 1,233 retrieved records. The results of the study show a strong focus on QI methodologies, particularly in preventive HIV care among health professionals, in contrast with lean methodologies, which mainly target patients' waiting times. The most frequently used tools were the plan-do-study-act (PDSA) and plan-do-check-act (PDCA) cycles, although their use often lacked clarity in distinguishing between lean and QI methodologies. To address these gaps, this study recommends appointing quality assurance personnel and developing a comprehensive framework to sustain lean healthcare and QI initiatives. These efforts aim to enhance the implementation of quality improvement practices and overall healthcare delivery in South Africa.
OPSOMMING
Al het Suid-Afrika 'n beleidsdokument oor gesondheidsorgsektor-kwaliteit ontwikkel, gaan die gehalte van dienslewering steeds agteruit. Hierdie studie het ten doel gehad om die toepassing van skraal- en kwaliteitverbetering (QI) metodologieë in Suid-Afrikaanse gesondheidsorgorganisasies te verken, met die fokus op die tydperke voor en na die bekendstelling van die beleidsdokument. Deur gebruik te maak van 'n sistematiese literatuuroorsig (SLR) wat gelei word deur die voorkeur-verslagdoeningsitems vir sistematiese oorsigte en meta-analise (PRISMA) vloeidiagram, is 17 relevante studies ontleed uit 'n totaal van 1 233 opgespoorde rekords. Die resultate van die studie toon 'n sterk fokus op QI-metodologieë, veral in voorkomende MIV-sorg onder gesondheidswerkers, in teenstelling met skraal metodologieë, wat hoofsaaklik pasiënte se wagtye teiken. Die instrumente wat die meeste gebruik word, was die plan-doen-studie-handeling (PDSA) en plan-do-check-act (PDCA) siklusse, alhoewel die gebruik daarvan dikwels nie duidelikheid gehad het om tussen maer en QI metodologieë te onderskei nie. Om hierdie leemtes aan te spreek, beveel hierdie studie aan om gehalteversekeringspersoneel aan te stel en 'n omvattende raamwerk te ontwikkel om skraal gesondheidsorg- en QI-inisiatiewe te onderhou. Hierdie pogings het ten doel om die implementering van gehalteverbeteringspraktyke en algehele gesondheidsorglewering in Suid-Afrika te verbeter.
1. INTRODUCTION TO THE SOUTH AFRICAN HEALTHCARE SYSTEM
The South African healthcare system, as in any other country, faces significant difficulties, including the unequal distribution of resources and inefficiencies that contribute to poor service delivery. About 8% of the country's gross domestic product (GDP) is spent annually on the healthcare sector. Sixty per cent of this budget is directed to the private sector, which serves only 20% of the population [1] - yet the public sector, which is responsible for 80% of the population, struggles with limited resources, resulting in higher infant and maternal mortality rates than in peer countries [2].
To address these issues, the National Department of Health (NDoH) introduced a quality of care policy in 2007 to strengthen the healthcare system through continuous quality improvement [1, 3]. While this policy provides a framework for improvement, its implementation relies heavily on individual healthcare organisations. However, the alignment of this policy with the practical application of lean and QI methodologies remains limited. This study therefore aims to assess the extent to which lean and QI methodologies have been implemented in South Africa's healthcare sector and to identify measurable outcomes achieved through these interventions.
A growing body of research highlights the application of lean and QI methodologies in healthcare systems globally. Lean methodologies, which originated in the manufacturing sector, aim to eliminate waste and enhance efficiency [4]. In contrast, QI methodologies focus on continuous improvements in processes and outcomes, often using tools such as PDSA cycles [5]. In South Africa, studies have emphasised the adoption of QI methodologies, particularly in addressing the challenges of HIV and tuberculosis (TB) care [6, 7]. For example, PDSA cycles have been widely used to streamline workflows and to reduce errors in patient management [8]. However, the application of lean methodologies remains limited, with most implementations targeting patient flow and the reduction of waiting times [8]. The limited adoption of lean in South African healthcare organisations is attributed to a lack of familiarity with lean principles and tools among healthcare professionals [9]. In addition, while the 2007 quality policy advocates continuous improvement, it does not explicitly incorporate lean methodologies, thus possibly contributing to the observed gaps [1].
Studies have also highlighted that, while QI is implemented more widely, lean methodologies provide long-term benefits that include cost reduction, process optimisation, and improved patient experiences [10]. Many healthcare facilities that have adopted lean methodologies have reported improvements in operational efficiency, with some achieving up to a 30% reduction in patient waiting times [4]. Despite this, problems such as resistance to change and insufficient training hinder the full integration of lean practices in the healthcare system [8]. However, according to Webster et al. [5], suggestions that combine the lean and QI approaches could provide a comprehensive framework for addressing inefficiencies in the South African healthcare sector.
The above review highlights the critical need to bridge the theoretical understanding of lean and QI with practical applications that are tailored to the South African healthcare context. By combining these insights, this study aimed to identify best practices and to address gaps in the field.
However, given the gaps in implementation, the sections that follow have adopted the research methodology approach of Mangaroo-Pillay and Coetzee [11], which uses an SLR to assess the application of lean and QI methodologies in SA. This is followed by an analysis of the key findings, which reflect the trends, difficulties, effectiveness, and clear differences between the lean and QI methodologies in improving healthcare service delivery. A discussion of these results in the context of the literature is then presented, drawing connections between South Africa's healthcare improvements and their broader implications. The study concludes with recommendations for policy and practice, highlighting opportunities to enhance the adoption of lean and QI in South African healthcare organisations.
2. METHOD
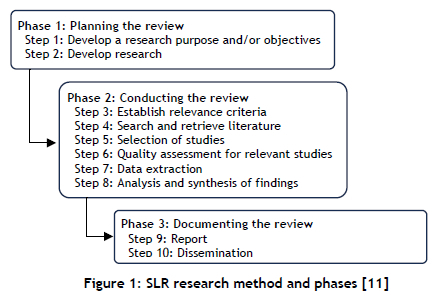
This study aimed to investigate the application of lean and QI methodologies in the South African healthcare sector in order to assess their effectiveness in addressing operational inefficiencies and improving service delivery. The method adopted for the SLR in this study used the approach proposed by Mangaroo-Pillay and Coetzee [11], which entails a sequence of ten steps that are grouped in research phases, as illustrated in Figure 1 below. A diagram illustrating the SLR would also have been required; but instead the researcher used a PRISMA flow chart adapted from the study of Tlapa et al. [3].
2.1. Step 1 : Develop the research objective (clearly stating the goal of the SLR)
The objective of the SLR is to investigate all studies of lean and QI methodologies in the South African healthcare sector in resolving problems. This is for the purpose of evaluating the studies of the pre- and post-development of the government policy on quality in healthcare SA.
2.2. Step 2: Develop a research procedure that defines the inclusion and exclusion criteria
in order to remove the researcher's bias and to increase the repeatability of the study. This will also include the keywords used in the search strategy and the quality assessment criteria in order to provide guidance to the research about what to search for and how to assess its quality.
2.3. Step 3: Establish relevance criteria
Inclusion criteria
- Studies or literature based in SA only.
- Theses, journal articles, or conference papers on lean or QI methodologies that have been implemented in the healthcare sector.
- Clear interventions and outcomes with empirical evidence.
- Experiences of Lean Healthcare interventions.
- All time ranges will be included from the years up to and including 2022, since the concept of lean healthcare in SA is still new.
- Government documents with lean or quality management interventions.
Exclusion criteria
- Literature referring to human body mass.
- Studies that are outside the field of the healthcare sector.
- Unclear interventions with no empirical evidence.
- Studies based in other countries.
- Non-accessible paper articles.
- Duplicate studies such as dissertations that have the same information on outcomes as journal articles and conference papers.
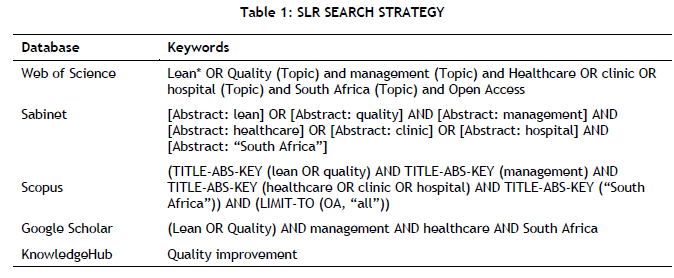
2.4. Keywords and databases
The study used five databases that are limited to academic studies in English (Table 1 below). The reason for using the keyword "quality" was to include all types of methodology, including studies of six sigma, as it is a quality management system. The keywords included studies based in SA because it would be advantageous for the researcher to investigate these studies from the researcher's own geographical location. However, the SLR also included government documents that record the implementation of lean or QI methodologies in the broader healthcare environment. The database used was KnowledgeHub. Furthermore, it would be important to note that KnowledgeHub is not as sophisticated as other scholarly databases; thus broad keywords were used to retrieve the government documents.
2.5. Quality assessment criteria
When applying quality assessment criteria, the first stage is to screen the studies, removing all duplicate studies in order to prepare for the second stage of screening, which is to establish their relevance to the research project. The study used the software EndNote X9 to eliminate duplicate studies.
Step 3: Establish relevance criteria
To establish the relevance criteria is to be specific about what the researcher wishes to achieve, keeping the goal in mind [3] and leaving room for as many studies as possible. Therefore, the relevance criteria that the researcher developed according to the three stages of screening were as follows:
- Stage 1 screening: Removing duplicate studies
- Stage 2 screening: Identifying the literature containing "Quality", "Lean", "Improvement", "Management", "Application", and "South Africa" in their titles, abstracts, or keywords.
- Stage 3 screening (final stage): Focusing on full-text studies with all document type ranges such as dissertations, journal articles, or conference papers that focus primarily on applying lean or any other quality tools in the South African private or public healthcare sectors with empirical measurable outcomes, whether quantitative, qualitative, or both, and the knowledge and experience of healthcare institutions post-implementation of lean techniques, since the research project is primarily about lean techniques.
Step 4: Search and retrieve
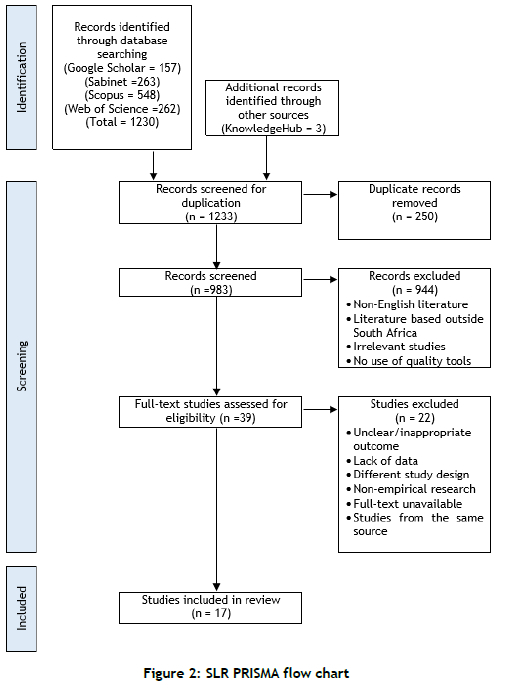
The search-and-retrieve step was initially done in step 2 of Table 1 (above) with the five databases, using the referencing manager software Endnote X9 to retrieve all the studies in the form of references that would also display abstracts. This step retrieved 1233 studies from which 250 duplicate studies were excluded. This led to the second stage of screening in order to assess the full-text eligibility of the studies in stage 3 of the screening.
Step 5: Select studies
Once all the referenced studies had been retrieved in Endnote, the second stage of screening was implemented to assess their eligibility for the third stage of screening. This was where the inclusion and exclusion criteria come into play. Stage 2 was a brief screening in which the researcher screened the title, abstract, and keywords, as explained in stage 3. Stage 2 excluded 944 studies and automatically met the exclusion criteria, which meant that the remaining 39 studies, consisting of dissertations, government documents, and journal articles, would be assessed for their eligibility in stage 3 of the screening.
Step 6: Assess quality of relevant studies
The quality assessment of relevant studies was the third and final stage of screening the studies for their eligibility for data extraction and analysis, as illustrated in the appendix and in the SLR PRISMA flow chart (Figure 2 below). In this final stage the researcher screened the full text of all 39 remaining studies to determine their relevance to the objectives of this SLR and, as a result, 22 studies were excluded.
Step 7: Extract data
After the researcher had finalised the list of studies that were found to be eligible, 17 studies remained for data extraction. The researcher used an Excel spreadsheet to extract the data from Endnote X9 in order to list the studies that were eligible to be reviewed. The appendix lists the 17 studies that the researcher analysed and interpreted. However, it would be important to note that the analysis focused on identifying patterns in lean and QI tool usage, their objectives, and their impact on healthcare performance.
2.6. Analysis
Step 8: Analyse and synthesise findings
This step analysed the data that was extracted in step 7 in order to address the objective of the SLR.
Step 9: Report
This step is where we report the review in detailed results in either graphical forms or written summaries to explain main findings.
Step 10: Dissemination
This is the final step where it is required to Publish the Systematic Literature Review.
2.6.1. Distribution of studies of lean and quality methodologies
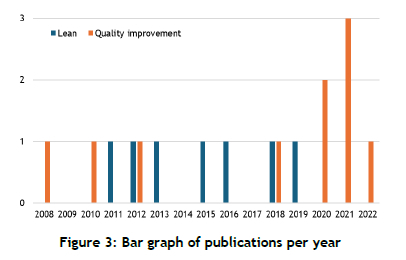
It was discovered that no studies of lean principles or QI studies had been published before the development of the SA national policy on quality in healthcare; the first such study appeared in 2008, after the policy document's publication. That study was in the context of applying QI; the earliest lean management study was published in 2011. As illustrated in Figure 3 below, there have been more quality management studies than lean management studies, which suggests that healthcare organisations are more familiar with quality tools.
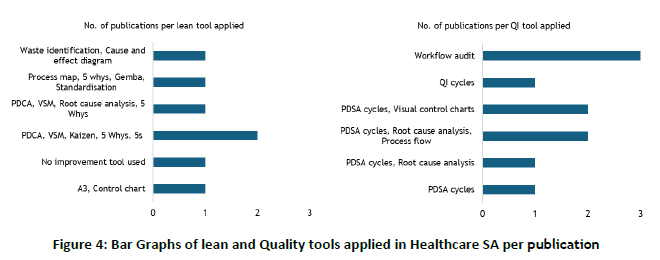
2.6.2. Common quality and lean tools applied in SA healthcare organisations
Figure 4 below illustrates the most frequently used continuous improvement tools in combination with other tools, such as PDCA combined with VSM. These are mostly used rather than quality tools that use PDSA cycles in combination with other tools, with root-cause analysis and visual control charts being the most frequently cited. Although the PDCA or PDSA cycles serve a similar function, there is a distinct difference between them: 'Check' focuses on assessing what was intended to be achieved vs what actually happened, while 'Study' is mostly used with QI initiatives that apply a 'trial-and-learning' method that allows the practitioner to test and evaluate the changes for a short-term period efficiently [10].
However, a study by Naidoo and Fields [8] (whose results are shown in the lean tool bar graph in Figure 4) did not aim to apply lean tools in healthcare organisations, but to determine the knowledge and experience of lean management among healthcare managers. That study concluded that, although there was limited knowledge of lean and its tools, the quality tools that were independent of the lean method - that is, the PDCA, 5-why, 5-S, and the A3 chart [8] - were commonly known to them. This supported the analysis of this SLR of the most frequently cited quality tools; however, it could be argued that those commonly known quality tools were used in the context of QI initiatives, as illustrated in Figure 8. Therefore, it would not be PDCA but rather PDSA that was widely used in healthcare organisations. This raised the question: Which quality tools are widely used, and which problems do they aim to solve?
2.6.3. The objectives of quality and lean tools
Objectives of lean methodology
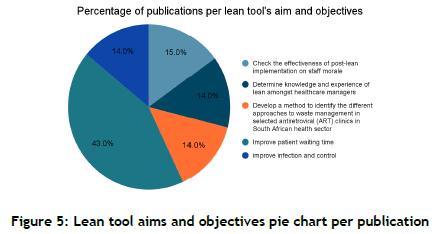
The pie chart in Figure 5 below shows what lean tools aim to achieve. From the studies analysed in our SLR, it was evident that 43% of them were focused on improving patient waiting time, primarily to improve the patient's experience and service delivery, while 28% of those studies focused just on the knowledge and experience and its effectiveness with staff morale. The overall conclusion was that, although there was little knowledge of lean management, there was empirical evidence that wherever it was being implemented, there would be an overall improvement not just in operational efficiency but also in staff morale, resulting in increased productivity and job satisfaction [11, 16].
What would be important to note in the majority of the studies that focused on improving patient waiting time is that they all focused on patient flow and that they commonly used PDCA in combination with VSM. Oddly enough, only one of those studies did a three-month follow-up on its project in an attempt to assess which lean efforts were being sustained. It found that only the one focused on an 18.2% reduction in waiting time had been sustained. This was relatively low, and also meant that eventually the other improvements would lapse [19].
2.6.4. The objectives of quality methodology in healthcare
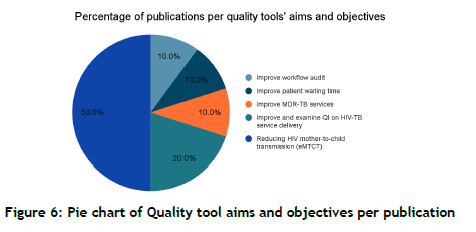
An analysis of the pie chart in Figure 6 below reveals that 50% of the quality improvement publications were studies that focused on reducing mother-to-child HIV transmissions using the PDSA cycles, which is closely associated with clinical studies. It is noticeable that 80% of the studies were focused on HIV and TB services, while only 20% focused on workflow and improving patient waiting time.
2.6.5. Research discipline
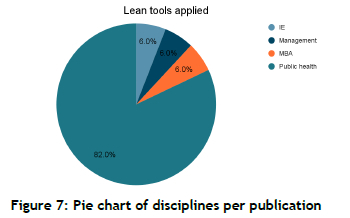
In the context of studies focused on improving healthcare organisations in SA, we found that 82% of those studies fell under public health, where healthcare professionals take a keen interest in using either quality or lean tools to improve their day-to-day activities. Although lean methodologies are a popular branch of industrial engineering (IE), only 6% of the discipline's studies contributed to the body of knowledge in the context of improving healthcare organisations, while management and Master's of Business Administration (MBA) degrees also contributed only 6%, as shown in Figure 7 below. However, it would be important to note that all the quality management studies stemmed from the public health discipline, which is an indicator that healthcare organisations are quite familiar with quality improvement initiatives.
2.6.6. Healthcare sectors
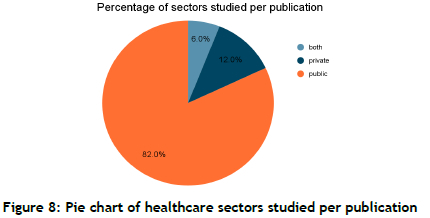
As illustrated in Figure 8, 82% of the studies of lean and quality management were in the public sector, and only 12% in the private sector. However, this does not mean that the private sector is perfect: even those 12% of the studies reveal similar problems to those in the public sector - they are just not as severe.
3. CONCLUSION AND FINDINGS
The analysis of the SLR revealed that there is a stronger emphasis on QI methodologies than on lean practices in healthcare in South Africa. As shown in Figure 6 above, around 50% of QI studies focused on preventive HIV care, often using PDSA cycles. In contrast, 43% of lean studies targeted patient waiting times, using tools such as PDCA cycles and value stream mapping (VSM), as shown in Figure 5. A significant finding was the lack of differentiation between lean and QI approaches in many studies. For example, while both methodologies use repetitive improvement tools, their objectives and contexts often overlap without
a clear delineation. Furthermore, only one study assessed the sustainability of lean interventions; this emphasises the need for long-term evaluation methods [9].
Moreover, as shown in Figure 8, 82% of the studies were conducted in the public healthcare sector, reflecting its pressing problems and resource constraints. However, the private sector's limited representation in the studies (around 12%) suggests that there is potential for a broader application of lean and QI methodologies.
4. RECOMMENDATIONS
Appointing dedicated quality assurance personnel to implement and monitor quality initiatives could bridge the gap between policy and practice. Future studies should also enhance methodological thoroughness by clearly defining and differentiating between lean and QI approaches in order to improve the validity of their findings. In addition, developing long-term sustainability frameworks with a focus on regular follow-ups and iterative improvements would ensure the durability of lean and QI interventions.
REFERENCES
[1] National Department of Health, "Quality improvement guide." 2012. Available Online https://shorturl.at/2g9wY (accessed 10 October 2022). [ Links ]
[2] D. P. S. Theunissen, "Improving service quality and operations at a South African private healthcare clinic through the implementation of lean principles," Nelson Mandela Metropolitan University, 2011. [Online]. Available: http://hdl.handle.net/10948/d1019943 [ Links ]
[3] D. Tlapa et al., "Effects of lean healthcare on patient flow: A systematic review," Value in Health, vol. 23, no. 2, pp. 260-273, 2020. [ Links ]
[4] J. Price, "Lean management in the South African public health sector: A case study," South African Health Review, vol. 2013, no. 1, pp. 191-199, 2013. [ Links ]
[5] P. D. Webster et al., "Using quality improvement to accelerate highly active antiretroviral treatment coverage in South Africa," BMJ Quality & Safety, vol. 21, no. 4, pp. 315-324, 2012. doi: 10.1136/bmjqs-2011-000381 [ Links ]
[6] L. M. Golden et al., "HIV retesting in pregnant women in South Africa: Outcomes of a quality improvement project targeting health systems' weaknesses," Southern African Journal of HIV Medicine, vol. 19, no. 1, e784, 2018. [Online]. Available: https://doi.org/10.4102/sajhivmed.v19i1.784 [ Links ]
[7] H. M. Yapa et al., "A continuous quality improvement intervention to improve antenatal HIV care testing in rural South Africa: Evaluation of implementation in a real-world setting," International Journal of Health Policy and Management, vol. 11, no. 5, pp. 610-628, 2022. doi: 10.34172/ijhpm.2020.178 [ Links ]
[8] L. Naidoo and Z. Fields, "Knowledge and experience of lean thinking amongst senior health care managers in selected South African public hospitals," SPOUDAI-Journal of Economics and Business, vol. 69, no. 4, pp. 21-37, 2019. [ Links ]
[9] L. Naidoo and O. H. Mahomed, "Impact of lean on patient cycle and waiting times at a rural district hospital in KwaZulu-Natal: Original research," African Journal of Primary Health Care and Family Medicine, vol. 8, no. 1, pp. 1-9, 2016. [Online]. Available: https://doi.org/10.4102/phcfm.v8i1.1084 [ Links ]
[10] PHAB, "Quality improvement methodologies: "Determining the best approach for incorporating QI into your agency's practice", Feb. 2020. Available at: https://phaboard.org/wp-content/uploads/ComparisonFrameworkFeb2020.pdf (accessed 10 November 2022). [ Links ]
[11] M. Mangaroo-Pillay and R. Coetzee, "Categorising South African lean implementation frameworks: A systematic literature review", in SAIIE31 Proceedings, 2020, pp. 395-427. [Online] Available: https://shorturl.at/ZdeES [ Links ]
[12] R. P. Abratt, M. Rautenbach, Y. Govender, and I. Oelofse, "A quality improvement programme in radiotherapy using workflow audits," South African Medical Journal, vol. 111, no. 2, pp. 106-109, 2021. [Online]. Available: https://doi.org/10.7196/samj.2021.v111i2.15310 [ Links ]
[13] K. Florman, J. Hudson, and M. Loveday, "Decentralisation of MDR-TB care in rural South Africa: Overcoming the challenges through quality improvement," Clinical Infection in Practice, vol. 7-8, 2020, 100020. [Online]. Available: https://doi.org/10.1016/j.clinpr.2020.100020 [ Links ]
[14] S. Gaga, N. Mqoqi, R. Chimatira, S. Moko, and J. O. Igumbor, "Continuous quality improvement in HIV and TB services at selected healthcare facilities in South Africa," Southern African Journal of HIV Medicine, vol. 22, no. 1, 2021, a1202. [Online]. Available: https://doi.org/10.4102/sajhivmed.v22i1.1202 [ Links ]
[15] S. Gengiah et al., "A quality improvement intervention to inform scale-up of integrated HIV-TB services: Lessons learned from Kwazulu-Natal, South Africa," Global Health Science and Practice, vol. 9, no. 3, pp. 444-458, 2021. [Online]. Available: https://doi.org/10.9745/ghsp-d-21-00157 [ Links ]
[16] H. Manisha Yapa et al., "The impact of continuous quality improvement on coverage of antenatal HIV care tests in rural South Africa: Results of a stepped-wedge cluster-randomised controlled implementation trial," PLoS Medicine, vol. 17, no. 10, e1003150, 2020. [Online]. Available: https://doi.org/10.1371/journal.pmed.1003150 [ Links ]
[17] M. S. Youngleson, P. Nkurunziza, K. Jennings, J. Arendse, K. S. Mate, and P. Barker, "Improving a mother to child HIV transmission programme through health system redesign: Quality improvement, protocol adjustment and resource addition," PLoS ONE, vol. 5, no. 11, e13891, 2010. [Online]. Available: https://doi.org/10.1371/journal.pone.0013891 [ Links ]
[18] S. Chatur, "Lean healthcare: A cross-section of South African ARV clinics," University of the Witwatersrand, Johannesburg, 2018. [Online]. Available: https://shorturl.at/rVS0C [ Links ]
[19] L. Naidoo, "The effect of lean on staff morale in a rural district hospital outpatient department in KwaZulu-Natal," Journal of Contemporary Management, vol. 12, no. 1, pp. 571-589, 2015. [Online]. Available: https://shorturl.at/K7MZ6 [ Links ]
[20] W. Rauf, J. J. Blitz, M. M. Geyser, and A. Rauf, "Quality improvement cycles that reduced waiting times at Tshwane District Hospital emergency department," South African Family Practice, vol. 50, no. 6, pp. 43-43e, 2008. [Online]. Available: https://doi.org/10.1080/20786204.2008.10873781 [ Links ]
Submitted by authors 9 Jan 2024
Accepted for publication 8 Mar 2025
Available online 30 May 2025
ORCID® identifiers
S. Kazadi
https://orcid.org/0000-0001-8824-9641
O. Olanrewaju
https://orcid.org/0000-0002-3099-9295
* Corresponding author: oludolapoo@dut.ac.za

{kind=link}
{kind=link}