










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.52 n.2 Pretoria Aug. 2022
https://doi.org/10.17159/2310-3833/2022/vol52n2a6
RESEARCH ARTICLE
Sensory modulation dysfunction in child victims of trauma from four residential care sites in southern Gauteng, South Africa
Rowena Yasmin JosephI, *; Janine van der LindeII; Denise FranzsenIII
IPrivate Practice, Johannesburg, South Africa http://orcid.org/0000-0002-4001-0479
IIDepartment of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand, Johannesburg, South Africa http://orcid.org/0000-0003-1067-9494
IIIDepartment of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand, Johannesburg, South Africa http://orcid.org/0000-0001-8295-6329
ABSTRACT
INTRODUCTION: The ability to modulate sensory input or the way an individual responds to sensory information, to create an appropriate adaptive response may be influenced by exposure to trauma. The study aimed to describe sensory modulation dysfunction in child victims of trauma in clinical settings in a residential urban South African setting.
METHOD: A descriptive quantitative research design was implemented. Using purposive sampling, child victims of trauma from four residential care sites were selected. The Child Sensory Profile"™ 2 was completed on 128 children by childcare workers.
RESULTS: Of the participants 91.4 % (117) were identified with sensory modulation dysfunction with only 8.6% (11) participants displaying no symptoms and scoring 'just like the majority of others' in all categories of the summary scores. More than 50% of the participants presented with sensory thresholds and self-regulation according to Sensory Avoidance, Sensory Sensitivity and Low Registration Quadrants that were 'more than others and much more than others'. Over 50% of participants also displayed difficulty in Touch Sensory Processing and Social-Emotional and Attentional Behaviours, in the 'more than others and much more than others' range. The sensory profile for this sample of Child Victims of Trauma, differed significantly from typical children 'just like the majority of others', indicating a vigilant sensory subtype with increased sensory sensitivity and sensory avoiding.
CONCLUSION: A high percentage of child victims of trauma presented with sensory modulation dysfunction, mostly with low thresholds for sensory input. Sensory Modulation dysfunction leads to a disruption in self-regulation and adaptive behaviour affecting participation in occupations
Keywords: sensory modulation, Child Sensory Profile 2 (CSPTM 2), (CVT), self-regulation, (SMD), Ayres Sensory Integration® (ASI), Child and Youth Centre (CYC), sensory profile, Sensory Sensitivity and Avoiding
INTRODUCTION:
Currently, in the researchers' experience, South African occupational therapists have noticed that an increasing number of children enter their practices with single or multiple types of trauma found to have associated neuroanatomical changes in the sensory cortex affecting visual and auditory cortices, and the limbic system2. Van der Kolk3 explained that continued exposure to trauma which includes flight, fight or freeze responses, affects how a child integrates sensory information that would usually allow for adaptive responses to the environment when stressors are perceived. Depending on a child's inbuilt physiology and neurology as well as external circumstances, the child's body will either 'shutdown', become dysregulated or adapt, when stressed by sensory input from the environment4. Research does indicate a relationship between sensory modulation and specific types of trauma in children5. This relationship influences their ability to self-regulate emotions and behaviour and experience satisfaction from participating in their occupations i.e. activities needed for schooling, self-care, socialisation and participating in extracurricular activities or hobbies6.
Trauma related stress in our communities is often a consequence of the violent and abusive nature of the South African context, compromising a child's ability to modulate and adapt. The need for intervention for emotional and behavioural challenges in Child Victims of Trauma (CVT) is increasing in South Africa due to the traumatised psyche of the South African nation. Children face the consequences of abuse and violence in all its forms7 and the trauma experienced may be a single trauma event or multiple traumas as a result of physical, emotional or sexual abuse. This may include being a witness to or a victim of abuse and violence, prolonged neglect in home situations, abandonment, and living in unsafe environments8. Whether a single incident or multiple incidents, trauma is a cause of stress in children, which literature associates with post-traumatic stress disorder and sensory modulation disorder (SMD)9. Although many of these children may be referred to occupational therapists for developmentally related problems, the skill and expertise of the therapist is required to link presenting problems with trauma backgrounds. Empirical research in this field of study will add rigour, clarity and sound scientific reasoning within the occupational therapy profession and thereby motivate therapists to expand their knowledge and skill in working with CVT.
Using Google Scholar and database searches (Pubmed, CINAHL, Proquest, Scopus and Cochrane), no empirical studies were found on the effects of trauma on sensory modulation, in CVT within the South African context. It is therefore critical that empirical evidence becomes available to provide a foundation for integrating sensory modulation evaluations and interventions within the treatment plan for a CVT.
Literature Review
Neurobiology of Trauma
Exposure to trauma and resultant post-traumatic stress disorder (PTSD) has been associated with persistent, abnormal adaptation of neurobiological systems to the stress, particularly if this occurs in children. The cascade model focuses on the effects of increased activation of the stress hormone systems on the developing brain, affecting the integration of sensory input10. If a child has been neglected or in a state of fear, in high or low arousal for a period of time, the child may either miss out on important sensory input or may misinterpret sensory information3. This has the potential to result in aggression, arousal dysregulation or shutting down if overwhelmed, sensory defensiveness, affect or behavioural dysregulation or running away11.
These aversive sensory responses are due to the limited ability of children to modulate sensory input and to manage their emotions and behaviour. Atchison4 explains that sensory modulation occurs when the central nervous system balances both excitatory and inhibitory inputs received by the sensory systems, internally, as well as those that occur externally from the environment. This balance is influenced by the autonomic nervous system which strives towards a 'calm alert state' with the parasympathetic and sympathetic nervous system working together to regulate the neurophy-siological state of the body. The limbic system responsible for regulating the autonomic nervous system, responds to a range of emotional stimuli and regulates behavioural responses12,13. The two main structures of the limbic system that influence our behavioural and emotional responses are the hippocampus that processes conscious memories and the amygdala that is involved in responses of fear and aggression. Research by van der Kolk14 on the neurobiology of trauma explains that trauma memories become 'stuck' in the amygdala thus not being processed through the hippocampus into the cortex, the pathway that normally assists to bring meaning to the extent of the trauma. Trauma memory symptoms can be observed in over arousal, sensory defen-siveness and sensory shutdown, which correlates with the influence on the limbic system and symptoms of sensory integration disorder, including sensory modulation disorder integral to the Ayres theory of Sensory Integration® (ASI®)12,13 According to Parham and Mailloux13 fear, anxiety or discomfort experienced in everyday situations by children with sensory modulation difficulties disrupt their daily routines.
Sensory Modulation
Sensory modulation reflects behaviours that have been researched and documented amongst others, as sensory seeking and sensory avoiding behaviours6,13-15. A sensory modulation disorder results in specific behaviours including impulsiveness, distractibility, hyperresponsitivity or hyporesponsitivity, increased arousal, hypersensitivity or hyposensitivity, hypervigilance, irritability, disorganisation, anxiety and poor self-regulation3,16-18. Based on the model of sensory processing and the theoretical foundation of ASI, Dunn19 proposed a framework for the processing of sensory information, or then sensory modulation, illustrating the interaction between the neurological threshold and the adaptive behavioural response that occurs.
According to Dunn19, modulation of sensory information can be placed on a continuum between the child's self-regulation behaviour (passive or active) and neurological thresholds (high or low), which results in appropriate behavioural responses to stimuli in the environment. The sensory modulation of typical children presents as 'just like the majority of others' with scores that range from 1 SD below the mean to 1 SD above the mean19. Fluctuations between habituation (high thresholds when the nervous system responds more slowly) and sensitisation (low thresholds when the nervous system responds quickly to stimulus) permit children to produce functional behaviour. Children with a high threshold are not easily activated by sensory stimuli and tend to be hypo-responsive. They take longer to respond to stimuli around them. Their responses present as 'less than others' or 'much less than others'. Children with a low threshold are easily activated by sensory stimuli and tend to be hyper-responsive. They are quick to notice and respond or are distracted by every stimulus. Their responses present as 'more than others' or 'much more than others' 19.
At one end of the continuum, a passive strategy towards sensory events is evident, where no action may be taken to change. At the other end of the continuum an active strategy is used, resulting in active control of the type and amount of sensory input, which allows a manageable amount of sensory input20.
Based on these constructs of neurological thresholds and behavioural response strategies or self-regulation according to the sensory input, Dunn proposed a Four Quadrant Model of Sensory Processing. According to Dunn19,21 individuals either use active self-regulating strategies depending on their neurological thresholds (engage in behaviours to limit exposure to the unpleasant stimuli or engage in sensory seeking behaviours to meet their sensory needs) or passive self-regulation strategies (disengage/withdrawing from circumstances around them or not noticing or reacting on sensory input). At both ends of the continuum these self-regulating behaviours can lead to distress for the child and the caregiver. The quadrant for high neurological thresholds and passive strategies is Low Registration, while Sensation Seeking represents active responding strategies within this threshold. The Sensory Sensitivity quadrant includes those children with a low neurological threshold and passive strategies while individuals within the active strategies quadrant and a low threshold fall into the Sensory Avoiding quadrant21.
A child's ability to process sensory information, inclusive of modulation, enables engagement in meaningful adaptive behaviours and facilitates participation in productive occupations15,22. For a child and adolescent these occupations are activities specifically related to school and education, personal care, play at school or as part of their leisure time out of school as well as social engagement. Early identification and treatment of sensory modulation difficulties contribute to improving the prognosis of children with sensory processing difficulties and could subsequently prevent or reduce emotional, behaviour, social and perceptual-motor difficulties in CVT23.
Sensory modulation dysfunction in CVT is also assessed using psychological evaluations. The Post Traumatic Stress Disorder Reaction-Index (PTSD- RI)24 has been used to identify disruptions in self-regulation and symptoms of sensory modulation disorder. According to this study, Re-experiencing, Avoidance and Over arousal were identified in 55% of adolescent victims of trauma25. In occupational therapy, specific sensory modulation assessments designed to determine the sensory input a child may have difficulty modulating or processing, as well as the emotional and behavioural components affected by their adaptation to sensory stimuli, are available. This assessment instrument can be used to determine how the child may respond to, or approach, participation in daily activities and include the Sensory Processing MeasureTM (SPMTM) developed by Parham et al.26 and revised by Parham et al.27 and the Sensory ProfileTM developed by Dunn28 and revised by Dunn19. These assessments have been used for evaluating sensory modulation in CVT to provide insight and clarity into their behaviour and emotional responses, as these relate to the child's daily living activities29. For the purpose of this research the Child Sensory ProfileTM 2 (CSPTM 2)19 was used.
The Effects of Trauma on Sensory Modulation
Yochman and Pat-Horenczyk23 examined the sensory modulation of 134 children exposed to continuous traumatic stress due to political violence. Using the Short Sensory Profile19 significant differences were found in these children, and according to their level of post-traumatic stress symptoms, with 62% experiencing clinical deficits in sensory modulation. Gorman and Kohl,30 reported similar results using the Short Sensory Profile19 on a sample of 900 child victims of trauma. They found that 53% of the participants presented with 'Probable difference' (more or less than others) and 'Definite difference' (much more or less than others) in sensory modulation. While 63% of the participants were under-responsive or sensory seeking, 42% were overresponsive to tactile sensation and 66% to auditory filtering30. In another study Vivano9 found that 80% of the children experiencing traumatic stress reaction and assessed with the Sensory ProfileTM28, had difficulties with sensory modulation, particularly sensory seeking, emotional reactivity and inattention.
Using the SPMTM, Sears et al.31 reported 81% of child victims of trauma had T-scores indicating 'Some Problems' to 'Definite Dysfunction' for sensory processing and presented with deficiencies in development, assessed to be extensive and complex. In the subtests for planning ideas and social participation, 84% and 100% of the participants respectively had various levels of dysfunction. They found that age, gender and length of stay in an institution for child victims of trauma did not affect the outcomes in terms of sensory processing dysfunction31. These studies highlight the importance of evaluating sensory modulation in CVT to determine the area of dysfunction that could be contributing to a child's difficulties in participating in daily activities.
The primary objective of this study was to identify and describe sensory modulation dysfunction in CVT within a South African context using the CSPTM 2.
METHODOLOGY
Research Design
A descriptive quantitative research design was used as the focus was on determining the quantity of possible sensory modulation responses on a large sample size while gaining a descriptive understanding of the areas of sensory processing most frequently affected in CVT.
Research context
The context of this study was four residential sites on the East Rand in Gauteng that care for CVT. They were identified from investigations conducted by the principal researcher with social workers delivering services on the East Rand, Gauteng. Children at risk are reported by members of the community, relatives of CVT, police services and educators. In some cases, children are brought directly to the centres by parents who are unable to care for them due to severe financial difficulties or violent circumstances in the home environment that are beyond their control. The 128 participants in this study resided in facilities which have dormitory type sleeping arrangements or single cottages with a housemother (childcare worker) in charge of a group of children. There was sufficient playground space for the children at these centres although there was a definite lack of play equipment. The safety and security of the children was a high priority at all centres. There was however a discrepancy between the residential sites in terms of human resources, equipment and daily supplies, professional services available as well as the consistency and commitment of the childcare workers.
Sample Selection
The child and youth residential sites were selected using convenience sampling and were in close proximity to the private practice of the principal researcher. This was done in an effort to reduce travelling time between the sites and ensure easier access during the research process. Using purposive sampling, a total sample of 128 children was selected from a population of children at the four residential centres, using the inclusion and exclusion criteria stated below
Inclusion Criteria
• CVT residing at the residential sites selected for this study.
• First or recurrent trauma
• Children aged between 6 years to 14 years
• All ethnic groups and socio-economic backgrounds
Exclusion Criteria
• Children with a diagnosed neurological condition or a severe mental disability who would not benefit from group intervention.
• Children who had received occupational therapy for the duration of the research study
Research instrument
The CSPTM 219 is a child report screening evaluation, which was completed by the childcare workers at each centre. This assessment instrument consists of 86 items that assess six sensory systems: auditory processing, visual processing, touch processing, movement processing, body position processing and oral sensory processing. There are also three items that assess behaviour, conduct, socio-emotional and attention. The child's score on the sensory systems is analysed according to the four quadrants of the CSPTM 2 as already discussed.
Based on a sample of 1791 children, the test-retest reliability for the CSPTM 2 is 0.83-0.97 and the inter-rater reliability is 0.69-0.8919. This indicates good to excellent stability in the test-retest reliability over time and mostly acceptable to good interrater reliability coefficients.
Ethical consideration, Data Collection and Data Management
Ethical clearance was obtained from the Human Research Ethics Committee at the University of the Witwatersrand (M180136). A letter of permission was submitted to the management of each care centre that caters for child and youth victims of trauma. Permission to include child participants and childcare workers in the research study was obtained from the management of the four residential centres. Permission was granted by the management of each centre in consultation with the senior social worker and head of the childcare workers. Due to two of the centres being under the Gauteng Department of Social Development, permission was also obtained from this department.
Prior to childcare workers completing the CSPTM 2, the research process was explained to the children at each residential site. Assent forms were completed according to two age categories, 6 to 10 years and 11 to 14 years of age. Each age category was seen in separate groups to allow for age-appropriate explanations of the research process. The assent form contained a simple written explanation that was communicated verbally by the principal researcher. Each child was invited to sign their names or use their thumbprint, if they had a challenge with writing. This would indicate their acceptance of being a part of the research process and would allow their childcare worker to provide the necessary information using the CSPTM 2. The childcare workers included in the study were invited to participate and complete the CSPTM 2 of the children under their care.
Each childcare worker needed to sign an informed consent form if they accepted the invitation to participate in the study. Thereafter they were provided with an information sheet that explained the study process. A group session with childcare workers was held prior to administration of the CSPTM 2, to demonstrate how to and provide a one-page guideline for completing the CSPTM 2. As the primary caregiver, the responses of the childcare workers were based on their knowledge and observations of the children for whom they care. A total of 71 childcare workers completed the CSPTM 2 forms of the identified 128 children selected for the study.
The principal researcher completed the scoring on the CSPTM 2 and did a first round of checks of the accuracy of the scoring and checked all forms were deidentified using participant codes or research identification (ID). Thereafter, the principal researcher's administrative assistant did a second round of checking of the accuracy of the scoring, ordered the screening forms into categories according to the research sites and captured the data on an Excel spreadsheet. A third round of checking was done by the principal researcher's administrative assistant to ensure that the research ID on each score sheet matched the research ID on the Excel spreadsheet. The Excel spreadsheet listed each child's research ID, gender, age at assessment, sensory section scores for each of the 52 items listed on the CSPTM2, behavioural section scores for the remaining 34 items on the CSPTM 2, summary quadrant scores, summary sensory section scores and summary behavioural section scores.
Data Analysis
Descriptive analysis using Statistica v13.3 was done using frequencies and percentages for demographic data of the children and the assessors. The frequencies and percentages were obtained from the calculations done on the excel spread sheet.
The raw scores on the CSPTM 2 were analysed according to the categories 'much less than others', 'less than others', 'just like the majority of others, 'more than others' and 'much more than others' on the sensory profile classification system, normal curve for the quadrants and sensory and behaviour sections to determine the percentage of CVT who presented with sensory modulation difficulties16. Some categories were combined as both indicated dysfunction and scores were recorded as either 'less than others and much less than others' or 'much more than others and more than others' A cut-off score above 50% of participants for the quadrants, sensory section and behaviour sections within these combinations of scores was set as identifying the frequency of sensory modulation dysfunction in this sample of CVT.
The mean scores for the quadrants, sensory and behaviour sections for the sample in this study were compared to the mean scores for typical children reported in the CSPTM 2 User's Manual19 to determine significant differences, using a chi-square test.
RESULTS
Demographic Information
All 71 childcare workers, from four research sites, had completed a Diploma in Child and Youth care. From the total of 71 childcare workers, 50.7% were between 40 to 49 years of age and 15.49% were in the process of additional tertiary education courses. Table 1 (below).

The sample of 128 child participants for whom the CSPTM 2 was completed consisted of 64 males and 64 females. They were in the first to eighth grade at school. Seven children were in a bridging class to assist with their individual barriers to learning. All children were admitted to the residential care facilities due to various types of trauma as indicated in Table ll (page above). From the background information of the children screened, the most frequent type of trauma in this study was neglect and abandonment. Although participants may have experienced more than one type of trauma, Table ll (above) indicates the primary trauma that resulted in a child being admitted to the residential care facility

Results of the Child Sensory ProfileTM 2
From the screening of the 128 participants, 11 participants' (8.6.%) scores were typical, 'just like the majority of others' on all 13 sections of the CSPTM 2. The remaining 117 participants (91.4%) presented with sensory modulation difficulties in the categories 'less than and much less than others' and 'more than and much more than others' in one or more areas of the summary scores i.e., quadrants, sensory sections and behavioural sections (Table lll, below).

From the Quadrant scores (Table lll, above), the highest percentage, (62.51%), of the children displayed Sensory Avoiding 'more than others and much more than others'. In this category of scores, more than 50% of participants presented with behaviours of Sensory Sensitivity and Low Registration.
From the Sensory Sections (Table III, page 50), the highest percentage, 58.60%, of the children displayed Touch Processing 'more than others and much more than others' and 50% displayed Sensitivity to Visual 'more than others and much more than others'. From the Behaviour Sections (Table lll, page 42), the highest percentage, 67.97%, of the children scored 'more than others and much more than others' for Social-Emotional Responses.
Data analysis revealed that the sample of CVT had a different pattern of sensory responsivity with the raw scores on the CSPTM 2 being higher than those reported by Dunn19 for the typically developing child, 'just like the majority of others,' indicating possible sensory processing difficulties in CVT (Table IV). The mean score patterns for the CVT that fell within the ranges for 'more than others' or 'much more than others' were for the Sensory Avoiding, Sensory Sensitivity and Low Registration Quadrants, the Touch Sensory Processing as well as the Socio-emotional and Attentional Behavioural sections.
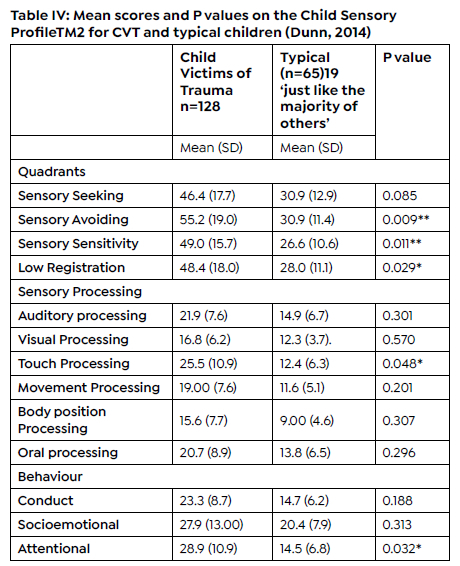
The quadrants indicating low thresholds (Sensory Sensitivity and Sensory Avoiding, high thresholds (specifically Low Registration) as well as the Touch Sensory Processing and the Attentional Behaviour had mean scores that were significantly higher than the mean scores of typical children. These are the sections and components of sensory modulation with which this sample of CVT experienced definite challenges.
DISCUSSION
A child's overall performance on the CSPTM 2 must be understood and related to their background, their living situation and school environment. The trauma backgrounds of the participants as stated in the social work files indicated abandonment, sexual abuse, neglect, death of a parent, witness of violence, abuse (not defined), physical abuse, emotional abuse, exposure to drugs, exposure to sexual abuse, victim of violence and exposure to alcoholism. The results of this study need to be understood within the context of these types of trauma backgrounds.
This study indicated that 91.4% of child victims of trauma from the four residential sites displayed responses that indicated sensory modulation dysfunction in one or more sections or components of the CSPTM 2. The findings of this research were supported by a number of studies indicating that dysregulation of the central nervous system in CVT results in difficulties in processing sensory information with either under or overreaction to sensory input2,5,23,32. The child may fluctuate between diminished awareness of sensory stimuli to hypersensitivity or avoidance4. The percentage of CVT in the current study was higher than the 80% indicated in studies by Howard et al.5, and Viviano9 using the Sensory Profile28, as well as the 53% to 62% indicated in the study by Gorman and Kohl30 and Yochman and Horenczyk23 respectively, using the Short Sensory Profile28. These differences may have been due to the environment in which the children in this study lived as Robinson and Brown33 highlighted the impact of the environmental aspects of sensory processing in trauma-affected children, specifically in relation to the physical environment of children's residential homes. They indicate that the environment in residential homes may exacerbate the sensory modulation dysfunction of CVT as they may not provide adequate input required to address these issues. Research also indicates a relationship between sensory modulation and specific types of trauma. Howard et al.5 found that children with a history of abuse and neglect had domain-specific sensory processing differences in comparison to children who had no history of maltreatment. This study used the Short Sensory Profile28 and indicated that children with a history of abuse (n=147) yielded impairments in tactile sensitivity (84.4%) and taste/smell sensitivity (47.6%). Children with a history of neglect (n=125) scored differently in underresponsive/seeks sensation (neglect =83.2%, abuse =57.8%)5.
According to the current research study, the sensory profile for CVT reflected significantly higher scores for Touch processing (indicating sensory profile characterised by an extreme response to tactile stimuli) as well as difficulties with Socio-emotional and Attentional Behaviours. Results suggest that the majority of CVT process sensory information differently from typical children presenting with low thresholds in the Sensory Sensitivity and Sensory Avoiding Quadrants as well as some presenting with high thresholds and specifically in the Low Registration quadrants. A higher percentage of the profile of CVT falls into the vigilant sensory subtype34 as the majority of CVT, avoid sensory experiences and show aversion to sensory input.
Sensory Profile of Child Victims of Trauma
Quadrant Sections
Sensory Avoiding and Sensory Sensitivity
In the Quadrant Section of the CSPTM 2 the low threshold scores for Sensory Avoiding were demonstrated by 60.94% of the participants and Sensory Sensitivity by 62.51% of the participants. For Sensory Avoiding (p=0.009) and Sensory Sensitivity (p=0.011) Quadrants, the mean scores of CVT were significantly higher compared to typical children, displaying behaviours that were 'more than others' (probable difference). These children will thus be more likely to over-respond to sensory input i.e., they will have enhanced awareness of important stimuli in the environment. Therefore, anticipation of harm and danger associated with a trigger or stimulus can generate immediate and powerful responses19, as is often seen in children who have experienced trauma. These children may understandably respond with protective responses associated with a lower inhibitory processes34 when exposed to any unfamiliar situation which they experience as a threat, due to their past exposure to traumatic environments.
Children who are sensory avoidant most often use active self-regulation strategies to manage situations that are overwhelming by actively withdrawing from a situation to reduce sensory input19. Evidence from literature19, supports the findings from this current study which indicates that CVT may go to great lengths to actively create order and routine in their environments in order to protect themselves, by reducing unanticipated sensory input to keep their environment predictable, or they may use avoiding patterns by keeping away from new stimuli and retreating from unfamiliar situations20. Ogden and Fisher35 concur that avoidance and withdrawal compose a core diagnostic cluster in trauma-related conditions.
Sensory Sensitivity Behaviours include the use of passive self-regulation strategies to manage situations and children may present with tantrums and aggressive behaviours. They are unable to block out stimuli and easily get overwhelmed. These children experience the environment as highly unpredictable, provoking anxiety20. They react more quickly and more intensely than others, have a high level of awareness of the environment, discriminate and attend to details as situations arise and are more discerning about the way they choose to respond to a particular situation19. For the CVT, their sensitivity may cause them to remain in a state of being overwhelmed, often responding negatively to their peer group or childcare worker. Clinical experience with CVT shows that triggers of past or present trauma can be in the form of facial expressions, words, tone of a voice or actions that would elicit immediate negative responses from a CVT, more easily than a typical child.
Low Registration and Sensory Seeking
Low Registration and Sensory Seeking Quadrants of the CSPTM 2 represent high neurological threshold scores and were displayed by 55.47% and 39.84% of participants respectively for responses as being 'more than others and much more than others.'
For the Low Registration Quadrant, the mean scores of CVT were significantly higher than that reported for typical children (p=0.029). Low registration indicates that these children use passive self-regulation strategies and often notice sensory input less than a typically responsive child. This results in not always attending to sensory information and having a low awareness of processing of sensory information and a low awareness of others19. They can demonstrate behaviour in which they seem uninterested in activities, unresponsive to others and appear overly tired. The results for the Low Registration Quadrant found in this study are similar to those found by Atchison4 and Howard et al.5 who reported that children who experience prolonged exposure to trauma or neglect present as more under-responsive. In some cases, this under-responsivity may be a reaction to the shutdown of an extremely over aroused system36. Neurologically when the body is under extreme stress as in the case of CVT, the sympathetic nervous system (arousal) either fights or flees in response to stress. When neither is possible for a child, the sympathetic system's (arousal) response can be extreme when the amount of stress is too much for the body to handle. It is at this point that the parasympathetic system (calming) spikes to such extreme levels that it overwhelms the sympathetic nervous system resulting in a freeze/shut down response. A child in shut down will dissociate, have an inability to think clearly in terms of accessing words and emotions or actively moving their bodies. This period of shutdown and underresponsivity can be momentary or last indefinitely especially if the perpetrator of the trauma continues to exist in the child's surroundings. The understanding of this response is vital for treatment planning as a bottom-up approach (sensory modulation intervention) would be more effective in the initial stages of a child's trauma therapy as compared to a top-down approach (talk therapy)36.
Sensory seeking behaviours are exhibited by using active self-regulation strategies in which the child always seeks more and more sensory input to stay alert19. Contrary to the findings of Viviano9, a lower percentage of children in the current study presented with sensory seeking, indicating that CVT with high thresholds, did not commonly use active self-regulation to obtain sensory input. This may also be as a result of the lack of sensory input available in their living environment33.
Sensory Sections
The CSPTM 2 consists of the Auditory, Visual, Touch, Movement, Body Position and Oral Processing Sensory Sections. The majority of children in this study presented with atypical Touch Sensory Processing and Visual Sensory Processing responses 'more than others and much more than others.'
Touch Sensory Processing
The processing of touch sensation is of high significance in child victims of trauma. It's influence on CVT has been widely researched30, 41. Warner et al.25 explains that the tactile system together with the vestibular and proprioceptive system have been found to be crucial in the regulation of the arousal state specifically with regards to achieving an organised and calming state in CVT. Nijenhuis et al.37 indicates that CVT have also reported excessive sensitivity to touch stimuli in particular, resulting in emotional or aggressive responses. This evidence indicates that the majority of children reflected difficulty in self-regulating activities and personal engagements with regards to touch sensation. In the Sensory Section of the CSPTM 2 58.60% of the children scored 'More than others and much more than others' for touch sensation. The mean score of CVT was significantly higher compared to typical children (p=0.048) in Touch Sensory Processing. The current research study supports Nijenhuis et al.37 indicating that CVT with low thresholds had significantly higher scores than typical children and were reported to become distressed during grooming, have an emotional or aggressive response to being touched and were distractible in social situations. Nijenhuis et al.37 and Sakson-Obada38 further explain that when children with low thresholds for touch processing are not able to avoid social situations, they may respond with frustration, anxiety and outbursts due to being in close proximity to others. This may affect their ability to form and maintain friendships.
Touch therefore has significant implications in treatment planning, especially occupational therapists who have the expertise to assess this area of sensory processing30. Warner et al.39 indicates that touch in therapy can trigger negative responses in CVT and it is important to have an advanced understanding of the potentially traumatic effects of touch for CVT so that therapy programmes are planned according to the individual child's needs. A child who is, for example, hypersensitive to touch can be first introduced to touch using only the sensory integration equipment, without the clinician's direct touch and then grading to situations allowing significant others to provide close touch to increase comfort and safety related touch experiences for the child.
Visual Processing
In this study 50% percent of children obtained a score 'more than others and much more than others' for Visual Sensory Processing. A comparison between CVT and typical children did not indicate a significant difference in visual processing (p=0.57). Mueller-Pfeiffer et al.40 found the alteration occurred in the ventral visual stream or the component of the visual system associated with processing objects in the visual sensory system of children associated with post traumatic stress disorder. This has been linked to dysfunctional attention processes and could have implications for the participation of CVT in functional activities related to school tasks, play, personal care and social engagements. In the current study, many CVT were reported to be distracted by visual details and movement of others in the residential care environments during homework and study time, resulting in poor attention, which in turn, affects their learning. Significant others in the child's environment need to understand the overreactivity or underreactivity to visual input including light and glare in the child's environment and make the necessary accommodations when there are high levels of emotional responses or there is decreased attention to an active environment.
Behavioural Sections
The Behavioural Section of the CSPTM 2 includes the responses to sensory input that are associated with the behaviour and the ability of the child to participate in their environmental. The 'probable difference' and 'definite difference' scores for CVT in this section ('more than others and much more than others' ) indicate difficulty with managing behaviours.
Socio-Emotional Behaviours
For Socio-Emotional Behaviour 67.97% of CVT scored 'more than others and much more than others'. Sensory modulation dysfunction for this behavioural section did not display a significant difference in comparison to typical children (p=0.313). The individual items from the CSPTM 2 highlighting the social emotional difficulties included challenges with changes in routine, strong emotional outbursts, needing protection from life and an inability to read others body language. According to Engel-Yeger et al.16, individuals with post-traumatic stress symptoms, scoring on the edge of the continuum (in this study 'more than others and much more than others') have elevated emotional burdens which negatively influences their affective state.
Therefore, it was not unexpected that the children in this study who had experienced or were exposed to trauma would have social emotional difficulties which could have affected their behaviour or adaptation to the environment. Their difficulty in dealing with change may be seen in acting out behaviours, aggression as a result of criticism, challenging activities and low frustration tolerance which affects their social and emotional responses19. van der Kolk3 reported that CVT, especially those who have been chronically abused, have problems regulating their arousal levels which contributes to their environmental sensitivity. This would imply that a child who is highly stressed, with sensory modulation difficulties, may react negatively to other children within a residential site, especially those with challenging behaviours and erratic emotions. Therefore, together with past traumatic experiences, commitment and care of childcare workers and peer group relationships could also impact on a child's socio-emotional responses at the residential sites.
Attentional Behaviours
In this research study, 53.91% of CVT displayed 'more than others and much more than others' responses in Attentional Behaviours. While distractibility has its roots in many neurological conditions, with CVT distractibility may indicate a high level of disengagement with the environment, in an attempt to avoid situations and people. Attentional behaviours in those who are hyper-responsive in this study were reported as an inability to pay attention and looking away from tasks due to being acutely aware of stimuli in their environment. This caused a distraction and prevented them from being productive when engaged in a task. These findings are supported by the significantly higher Attentional Behaviour mean score (p=0.032) when compared to typical children, 'just like the majority of others'.
Conduct Behaviours
Although 50% of the CVT demonstrated Conduct behaviours 'more than others and much more than others', the mean score for this behavioural section was not significantly higher from the mean score for typical children (p =0.188). Frequent conduct behaviours reported by childcare workers in this study was refusal to cooperate and temper tantrums.
Limitations of the study
Limitations of the study include the use of a carer report questionnaire which can be subjective. The childcare workers varied in how familiar they were with each child on whom they completed the questionnaire. This could have influenced the accuracy of their observations when completing the CSPTM 2.
Having educators also completing a questionnaire on the children included in this study could have strengthened the results on the data collected. This additional information would have informed a more in-depth understanding of the behaviour patterns presented on the CSPTM 2 and how they affect the children's participation in activities of daily living.
Considering the limitations of this study, the credibility of future research in this field could be enhanced by increasing the number of research assistants in the data collection phase and having a set standard or criteria for the choice of the childcare workers, based on their experience, level of education and the length of their relationship with each child participant.
CONCLUSION AND RECOMMENDATIONS
This study supports the findings of other studies which indicate that experience and exposure to trauma is linked to the behaviour and emotional patterns in children. The children in this study displayed a different sensory profile with significantly higher mean scores in the Sensory Sensitivity and Sensory Avoiding Quadrants. Sensory modulation dysfunction is neu-rogenic i.e., arising from changes within the nervous system. In this study these changes were consistent with sensory modulation related mostly to overresponsivity to sensory input, particularly Touch Sensory Processing, as well as Attentional Behaviours which can affect participation in everyday activities and socialisation. Thus, this study provided provisional advocacy for the assessment and treatment implications for CVT using sensory modulation intervention programmes. Confirming sensory modulation dysfunction in these CVT, adds credibility to the use of the CSPTM 2 as a screening evaluation in assessing this population of children. This implies that due to the growing pandemic of victimisation against children within the South African context and internationally, there is a need to assess sensory modulation dysfunction more extensively and be inclusive of sensory modulation intervention within occupational therapy programmes23.
AUTHOR CONTRIBUTIONS
Joseph R was the principal researcher and author of article contributing to: research, data collection and write up. van der Linde, J was a supervisor contributing: knowledge and expertise from the field of Paediatrics. Franzen, D was a supervisor contributing knowledge and expertise from the field of Research and Statistics.
ACKNOWLEDGEMENTS
Thank you to the co-authors of this article for their invaluable contribution and to all the caregivers who gave of their time for this research.
DECLARATION OF CONFLICTS OF INTEREST
The authors declare no conflict of interest. All funding was awarded after review of the study protocol by selection committees.
REFERENCES
1. Swingler H. Conflict leaves children traumatised, anxious - for life. UCT News. Available from: https://www.news.uct.ac.za/article/-2019-08-26-conflict-leaves-children-traumatised-anxious-for-life [ Links ]
2. Fraser K, MacKenzie D, Versnel J. Complex Trauma in Children and Youth: A Scoping Review of Sensory-Based Interventions. Occupational Therapy in Mental Health. Routledge; 2017;33(3): 199-216. Available from: doi:https://doi.org/10.1080/0164212X.2016.1265475 [ Links ]
3. van der Kolk BA. The neurobiology of childhood trauma and abuse. Child and Adolescent Psychiatric Clinics of North America. 2003;12(2): 293-317. Available from: doi:https://doi.org/10.1016/S1056-4993(03)00003-8 [ Links ]
4. Atchison BJ. Sensory Modulation Disorders Among Children With a History ofTrauma : ... Language, Speech, and Hearing Services in Schools. 2007;38(2): 109-116. Available from: doi: https://doi.org//10.1044/0161-1461(2007/011 [ Links ]
5. Howard ARH, Lynch AK, Call CD, Cross DR. Sensory processing in children with a history of maltreatment: an occupational therapy perspective. Vulnerable Children and Youth Studies. 2020;15(1): 60-67. Available from: doi: https://doi.org/10.1080/17450128.2019.1687963 [ Links ]
6. Mcintosh DN, Miller LJ, Shyu V, Hagerman RJ. Sensory-modulation disruption, electrodermal responses, and functional behaviors. Developmental Medicine and Child Neurology. 1999;41(9): 608-615. Available from: doi:https://doi.org/10.1017/S0012162299001267 [ Links ]
7. Gregorowski C, Seedat S. Addressing childhood trauma in a developmental context. Journal of Child and Adolescent Mental Health. 2013. p. 105-118. Available from: doi: https://doi.org//10.298 9/17280583.2013.795154 [ Links ]
8. Burton P, Ward C, Artz L, Leoschut L. The Optimus study on child abuse, violence and neglect in South Africa. 2015. Available from: https://www.saferspaces.org.za/resources/entry/the-optimus-study-on-child-abuse-violence-and-neglect-in-south-africa [ Links ]
9. Viviano A. The Incidence of Caregiver Reported Sensory Processing Disorders in Children Who Are Experiencing Traumatic Stress Reaction. Master's Theses. Western Michigan University; 2001. Available from: https://scholarworks.wmich.edu/masters_theses/4692 [ Links ]
10. Teicher MH, Andersen SL, Polcari A, Anderson CM, Navalta CP. Developmental neurobiology of childhood stress and trauma. Psychiatric Clinics of North America. 25(2): 397-426. Available from: doi:https://doi.org/10.1016/S0193-953X(01)00003-X [ Links ]
11. May-Benson TA, Koomar JA. Systematic Review of the Research Evidence Examining the Effectiveness of Interventions Using a Sensory Integrative Approach for Children. American Journal of Occupational Therapy. 2010;64(3): 403-414. Available from: doi:https://doi.org/10.5014/ajot.2010.09071 [ Links ]
12. Alers V. The 20th Vona du Toit Memorial Lecture 2007: Proposing the social atom of occupational therapy: Dealing with trauma as part of an integrated inclusive intervention. South African Journal of Occupational Therapy. 2008;38(3): 3-10. [ Links ]
13. Parham LD, Mailloux Z. Sensory integration. In: Case-Smith J, O'Brien J (eds.) Occupational therapy for children. 6th ed. Maryland Heights: Mosby; 2010. p. 325-372. [ Links ]
14. van der Kolk B. The body keeps the score: Mind, brain and body in the transformation of trauma. London: Penguin; 2014. [ Links ]
15. Dunn W. The sensations of everyday life: Empirical, theoretical, and pragmatic considerations. American Journal of Occupational Therapy. 2001;55(6): 608-620. Available from: doi:https://doi.org/10.5014/ajot.55.6.608 [ Links ]
16. Engel-Yeger B, Palgy-Levin D, Lev-Wiesel R. The Sensory Profile of People With Post-Traumatic Stress Symptoms. Occupational Therapy in Mental Health. 2013;29(3): 266-278. Available from: doi:https://doi.org/10.1080/0164212X.2013.819466 [ Links ]
17. Grayson J, Childress A, Baker W, Grayson P. Evidence - based treatments for Childhood Trauma. Virginia Child Protection Newsletter: Vol 95. 2012; 1-9. [ Links ]
18. Pechtel P, Pizzagalli DA. Effects of early life stress on cognitive and affective function: An integrated review of human literature. Psychopharmacology. 2011;214(1): 55-70. Available from: doi:https://doi.org/10.1007/s00213-010-2009-2 [ Links ]
19. Dunn W. Sensory Profile-2, Overview Presentation. New York: Psimas Learning. Pearson; 2014. [ Links ]
20. Duncan DF. Growing up under the gun: Children and adolescents coping with violent neighborhoods. Journal of Primary Prevention. 1996. p. 343-356. Available from: doi:https://doi.org/10.1007/BF02411740 [ Links ]
21. Dunn W. The Impact of Sensory Processing Abilities on the Daily Lives of Young Children and Their Families: A Conceptual Model. Infants & Young Children. 1997;9(4): 23-35. [ Links ]
22. Yochman A, Parush S, Ornoy A. Responses of preschool children with and without ADHD to sensory events in daily life. American Journal of Occu pational Therapy. 2004;58(3): 294-302. Available from: doi:https://doi.org/10.5014/ajot.58.3.294 [ Links ]
23. Yochman A, Pat-Horenczyk R. Sensory Modulation in Children Exposed to Continuous Traumatic Stress. Journal of Child and Adolescent Trauma. 2020;13(1): 93-102. Available from: doi:https://doi.org/10.1007/s40653-019-00254-4 [ Links ]
24. Steinberg AM, Brymer MJ, Kim S, Briggs EC, Ippen CG, Ostrowski SA, et al. Psychometric Properties of the UCLA PTSD Reaction Index: Part I. Journal of Traumatic Stress. 2013;26(1): 1-9. Available from: doi:https://doi.org/10.1002/jts.21780 [ Links ]
25. Warner E, Spinazzola J, Westcott A, Gunn C, Hodgdon H. The Body Can Change the Score: Empirical Support for Somatic Regulation in the Treatment of Traumatized Adolescents. Journal of Child and Adolescent Trauma. 2014;7(4): 237-246. Available from: doi:https://doi.org/10.1007/s40653-014-0030-z [ Links ]
26. Parham LD, Miller-Kuhaneck H, Ecker C, Henry DA, Glennon TJ. SPM Sensory Processing Measure. Los Angeles: Western Psychological Services; 2007. [ Links ]
27. Parham L, Miller-Kuhaneck H, Ecker C, Henry D, Glennon T. SPM sensory processing measure. Western Psychological Services; 2017. [ Links ]
28. Dunn W. Sensory Profile. San Antonio: The Psychological Cooperation; 1999. [ Links ]
29. Dunn W, Little L, Dean E, Robertson S, Evans B. The state of the science on sensory factors and their impact on daily life for children: A scoping review. OTJR Occupation, Participation and Health. 2016;36(2). Available from: doi:https://doi.org/10.1177/1539449215617923 [ Links ]
30. Gorman K, Kohl K. The Role of Sensory Integration in Recovery Oriented Trauma Informed Care. 13th Annual International Human Trafficking and Social Justice Conference. University of Toledo; 2016. [ Links ]
31. Sears AR, Apodaca J, Sanders H, Sears AR;, Jackolyn A; Sensory Processing Deficits in Children That Have Experienced Trauma or Neglect Recommended Citation. Albuquerque: Poster presented at the University of New Mexico Occupational Therapy Research Poster Day, April 20th; 2016. Available from: doi:https://doi.org/10.5014/ajot.51.7.500 [ Links ]
32. Da Silva K. The Sensory Treatment Approach in Dealing with Trauma in Children: Does it Work?. Providence College; 2011. Available from: http://digitalcommons.providence.edu/socialwrk_students/76 [ Links ]
33. Robinson C, Brown AM. Considering sensory processing issues in trauma affected children: The physical environment in children's residential homes. Scottish Journal of Residential Child Care. 2016;15(1). [ Links ]
34. McLaughlin KA, Sheridan MA, Lambert HK. Childhood adversity and neural development: Deprivation and threat as distinct dimensions of early experience. Neuroscience and Biobeha-vioral Reviews. 2014. p. 578-591. Available from: doi: https://doi.org/10.1016/j.neubiorev.2014.10.012 [ Links ]
35. Ogden P, Fisher J. Sensorimotor psychotherapy: interventions for trauma and attachment. New York: WW Norton & Company; 2015. [ Links ]
36. Lane S. Sensory modulation. In: Bundy A, Lane S, Murray E (eds.) Sensory integration: theory and practice. Philadelphia: F. A. Davis; 2002. [ Links ]
37. Nijenhuis ERS, Spinhoven P, Van Dyck R, Van der Hart O, Vanderlin-den J. Degree of somatoform and psychological dissociation in dissociative disorder is correlated with reported trauma. Journal of Traumatic Stress. 1998;11(4): 711-730. Available from: doi: https://doi.org/10.1023/A:1024493332751 [ Links ]
38. Sakson-Obada O. Changes in sensing, the basic function of body ego, as a result of trauma. In: Widera - Wysoczanska A, Kuczynska A (eds.) Interpersonal trauma and its consequences in adulthood. Cambridge: Cambridge Scholar Pubulications; 2010. p. 139-152. [ Links ]
39. Warner, E., Koomar, J., & Westcott, A. (2009). Arousal Regulation in Traumatized Children, Sensorimotor Interventions. International Trauma Conference. url: www.traumacenter.org/announcements/TConf.09_SMART_Handouts.pdf [ Links ]
40. Mueller-Pfeiffer C, Schick M, Schulte-Vels T, O'Gorman R, Michels L, Martin-Soelch C, et al. Atypical visual processing in posttraumatic stress disorder. NeuroImage: Clinical. 2013;3(2013): 531-538. Available from: doi: https://doi.org/10.1016/j.nicl.2013.08.009 [ Links ]
41. Kaiser EM, Gillette CS, Spinazzola J. A Controlled Pilot-Outcome Study of Sensory Integration (SI) in the Treatment of Complex Adaptation to Traumatic Stress. Journal of Aggression, Maltreatment & Trauma. 2010;19(7): 699-720. Available from: doi: https://doi.org/1 0.1080/10926771.2010.515162 [ Links ]
Submitted: 20/01/2021
Reviewed: 20/04/2021
Revised: 21-05-2021
Accepted: 25-05-2021
DATA AVAILABILITY: On reasonable request from Authors
FUNDING: Ruth Watson OTASA Research Grant
* Corresponding author: Rowena Joseph RowenaOT@telkomsa.net
